|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
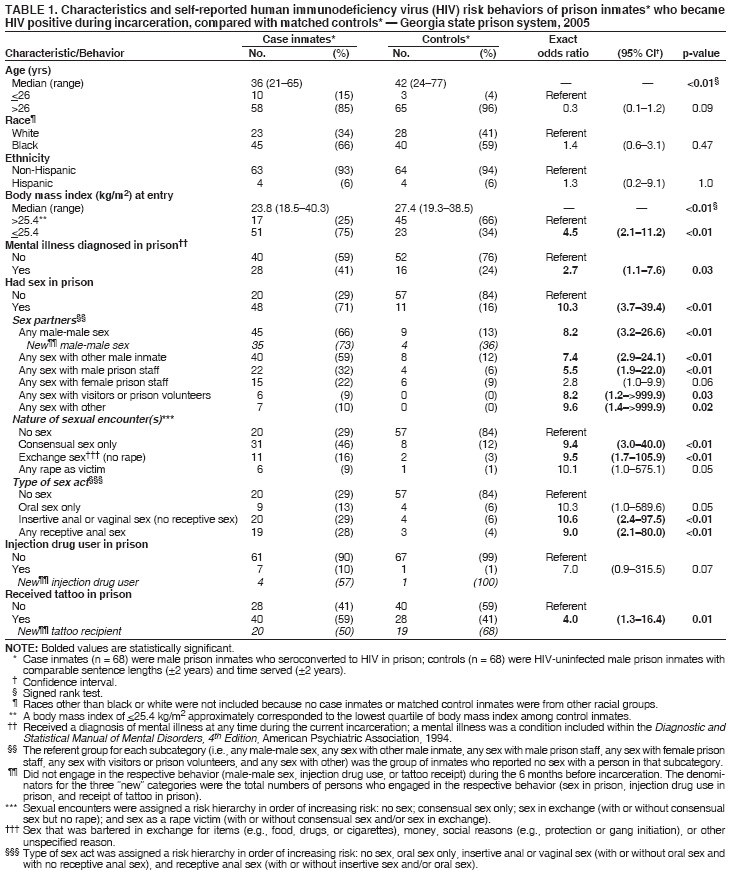
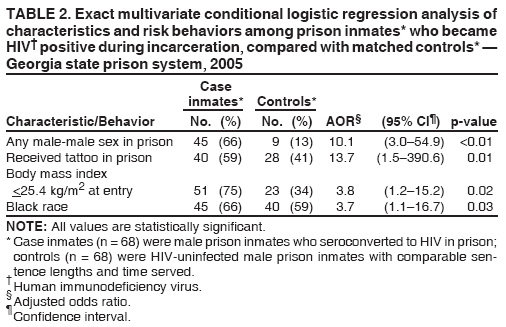
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. HIV Transmission Among Male Inmates in a State Prison System --- Georgia, 1992--2005The estimated prevalence of human immunodeficiency virus (HIV) infection is nearly five times higher for incarcerated populations (2.0%) (1) than for the general U.S. population (0.43%) (2). In 1988, the Georgia Department of Corrections (GDC) initiated mandatory HIV testing of inmates upon entry into prison and voluntary HIV testing of inmates on request or if clinically indicated. GDC offered voluntary HIV testing to inmates annually during July 2003--June 2005 and currently offers testing to inmates on request. During July 1988--February 2005, a total of 88 male inmates were known to have had both a negative HIV test result upon entry into prison and a subsequent confirmed positive HIV test result (i.e., seroconversion) during incarceration. Of these 88 inmates, 37 (42%) had had more than one negative HIV test result before their HIV diagnosis. In October 2004, GDC and the Georgia Division of Public Health invited CDC to assist with an epidemiologic investigation of HIV risk behaviors and transmission patterns among male inmates within GDC facilities and to make HIV prevention recommendations for the prison population. This report describes the results of that investigation, which identified the following characteristics as associated with HIV seroconversion in prison: male-male sex in prison, tattooing in prison, older age (i.e., age of >26 years at date of interview), having served >5 years of the current sentence, black race, and having a body mass index (BMI) of <25.4 kg/m2 on entry into prison. Findings from the investigation demonstrated that risk behaviors such as male-male sex and tattooing were associated with HIV transmission among inmates, highlighting the need for HIV prevention programs for this population. To describe the state's male inmate population and the 88 inmates known to have become HIV positive while in prison (i.e., seroconverters), investigators analyzed summary demographic data for all inmates and prison-movement and HIV-testing histories of seroconverters, all of which had been routinely collected for GDC administrative purposes. The HIV-testing and prison-movement histories of seroconverters were also analyzed to identify the facility in which HIV transmission occurred, defined as one in which a seroconverter had a negative HIV test followed by a subsequent positive HIV test confirmed by Western blot while incarcerated in the same facility. To identify demographic characteristics and behavioral risk factors associated with HIV seroconversion, both an unmatched and a matched case-control study were conducted. Male inmates aged >18 years were eligible to participate in both studies. Case inmates had documented HIV seroconversion during the incarceration period. Control inmates had a negative result on their most recent HIV test (during 1997--2005) and had their HIV-negative status confirmed by repeat HIV testing on enrollment in the investigation. For the unmatched study, control inmates were randomly selected from a list of eligible inmates in the seven prisons in which the largest proportion of seroconverters were believed to have become infected with HIV. For the matched case-control study, to compare inmates with the same duration of exposure to risk for HIV transmission, control inmates were selected from the 31 prisons currently housing the case inmates and matched by sentence length (±2 years) and time already served (±2 years). After giving written, informed consent, inmates completed audio computer-assisted self-interviews (ACASI). No personally identifying information was collected in these interviews. To determine how behavioral risks for HIV infection changed during incarceration, the interview asked about sex, drug use, and tattooing behaviors during the 6 months before incarceration and during the incarceration period. Questions were also asked about knowledge regarding HIV transmission. Exact multivariate logistic regression was used to analyze unmatched data, and exact multivariate conditional logistic regression was used to analyze matched-pair data. After ACASI, investigators asked open-ended questions about strategies to reduce HIV transmission among inmates. In October 2005, GDC housed 44,990 male inmates in 73 facilities; median age was 34 years (range: 15--88 years). A total of 28,350 (63%) were black, 16,364 (36%) were white, 50 were American Indian (0.1%), and 47 (0.1%) were Asian; race was not reported for 179 (0.4%). A total of 856 (1.9%) were known to be HIV infected, of whom 780 (91%) were infected before incarceration, and 732 (86%) were black.* During July 1988--February 2005 (the month in which the last seroconverter included in the investigation was identified), 88 male inmates had both a negative HIV test result upon entry into prison and a subsequent HIV seroconversion during incarceration. Of these 88 inmates, the median age at time of HIV diagnosis was 32 years (range: 21--58 years). Fifty-nine (67%) were black, and 29 (33%) were white. Diagnoses were made during September 1992--June 2003 for 47 (53%) inmates and during July 2003--February 2005 for 41 (47%). For 26 (30%) of the 88 seroconverters, the facility in which HIV transmission occurred was identified; for 34 (39%) seroconverters, the facility in which transmission occurred was narrowed to two. Of the 88 seroconverters, 11 were released from prison and two died before the start of the case-control study. Of the remaining 75 inmates, 68 (91%) were enrolled in both the unmatched and matched case-control studies as case inmates. Sixty-five (87%) unmatched control inmates and 70 (79%) matched control inmates who were eligible agreed to participate. In multivariate analysis of the unmatched study, variables significantly associated with HIV seroconversion were male-male sex in prison, older age, having served >5 years of the current sentence, and having a BMI of <25.4 kg/m2 on entry into prison. Univariate analysis of matched case-control study data identified multiple demographic characteristics and risk behaviors as significantly associated with HIV seroconversion (Table 1). However, in the final multivariate logistic regression model, only four covariates were significantly associated with HIV seroconversion during incarceration: male-male sex in prison, receipt of a tattoo in prison, BMI of <25.4 kg/m2 on entry into prison, and black race (Table 2). Among 54 inmates (45 case and nine control) reporting male-male sex while in prison, 35 (78%) of 45 case inmates and four (44%) of nine control inmates reported no male-male sex during the 6 months immediately before incarceration. Among 54 inmates (case and control) who reported any male-male sex during incarceration, 39 (72%) reported consensual sex and 48 (89%) reported sex with other inmates. Exchange sex (e.g., for money, food, or cigarettes) and rape were also reported. Of 43 inmates (34 case and nine control) who reported any consensual sex, 13 (30%) reported using condoms or other improvised barrier methods (e.g., rubber gloves or plastic wrap). Of 14 (12 case and two control) inmates who reported any exchange sex, three (21%) reported using improvised barrier methods but not condoms; no barrier methods were used during rape. Of 59 inmates (48 case and 11 control) who reported having sex in prison, 36 (75%) case inmates and six (55%) control inmates reported intent to tell sex partners outside prison about unprotected sex in prison. Of 68 inmates who reported receiving a tattoo in prison, 59 (87%) used clean tattooing equipment for at least one tattoo, 52 (76%) used bleach to clean tattooing equipment, two (3%) used tattooing equipment that was not cleaned, and seven (10%) did not know whether tattooing equipment was cleaned before they received at least one tattoo. Most inmates correctly identified that HIV can be transmitted through unprotected sex (88%), needle sharing (83%), and infected blood (78%). In 181 responses to open-ended questions about how to reduce HIV transmission in prison, inmates suggested that condoms be made available in prison (38%), that inmates receive HIV education (22%), and that inmates practice safe tattooing (13%). Reported by: J Taussig, MPH, Georgia Dept of Corrections and Georgia Dept of Human Resources, Div of Public Health; RL Shouse, MD, Georgia Dept of Human Resources, Div of Public Health. M LaMarre, MN; L Fitzpatrick, MD, P McElroy, PhD, CB Borkowf, PhD, R MacGowan, MPH, AD Margolis, MPH, D Stratford, PhD, E McLellan-Lemal, MA, K Robbins, W Heneine, PhD, A Greenberg, MD, P Sullivan, PhD, Div of HIV/AIDS Prevention, National Center for HIV, Hepatitis, STD and TB Prevention; Z Henderson, MD, K Jafa, MBBS, EIS officers, CDC. Editorial Note:This report indicates that HIV transmission among inmates in Georgia's prison system was associated with male-male sex and tattooing and highlights the need for more effective HIV prevention among inmates. Sex among inmates occurs (4), and laws or policies prohibiting sex among inmates have been difficult to implement or enforce. However, GDC might consider certain HIV prevention options (e.g., education, testing, and prevention counseling) proven to be effective for nonincarcerated populations; some of those prevention measures are being used in correctional settings within and outside the United States (4). CDC recommends that HIV education, testing, and prevention counseling be made available to populations at increased behavioral or clinical risk for HIV infection, including inmates in correctional facilities (5,6). HIV prevention education in state prisons should address male-male sex, tattooing, and injection drug use that occurs during incarceration and risk behaviors that occur after release. Case studies of inmate-led HIV prevention interventions suggest that these interventions might engender more inmate trust of and cooperation with intervention staff (4). HIV education might also benefit correctional facility staff. CDC recommends that HIV screening be provided upon entry into prison and before release and that voluntary HIV testing be offered periodically during incarceration. This investigation demonstrates that annual voluntary testing is useful; 41 (47%) of 88 HIV seroconverters were identified during the 2 years in which annual testing was offered. Prison HIV testing programs allow inmates to learn their HIV status and, if not infected, to learn protective behaviors to reduce their HIV infection risks (7). Inmates who test HIV positive should receive antiretroviral treatment and care in addition to prevention counseling to protect future sex partners; before release, they should receive discharge planning and linkages to care in the community. GDC provides treatment and care for HIV-infected inmates, provides a 30-day supply of antiretroviral drugs on release and, in 12 of 73 facilities, undertakes enhanced HIV discharge planning, which includes individualized case management, housing placement, substance abuse and mental health treatment referrals, enrollment in benefit programs, and referrals for assistance with employment and other social services. Approximately 15% of inmates reported using improvised barrier protection methods during sex, and 38% recommended making condoms available in prisons. Providing condoms to sexually active persons is an integral part of HIV prevention interventions outside prisons. However, in most prison and jail settings, condoms are considered contraband (4). Condoms are provided to some inmates in state prisons in Mississippi and Vermont and jails in Los Angeles, New York, Philadelphia, San Francisco, and the District of Columbia (4). A recent survey in a large jail in a U.S. city reported that condom distribution was acceptable to most inmates and correctional officers (8). Departments of corrections with existing condom distribution programs should evaluate those programs to determine their effectiveness; departments of corrections without condom distribution programs should assess relevant state laws, policies, and circumstances to determine the feasibility and benefits and risks of implementing such programs. Although no case of HIV transmission via tattooing has been documented, the procedure carries a theoretical risk for transmission if nonsterile equipment is used. In this investigation, receipt of a tattoo was associated with HIV seroconversion. Further investigation is required to explore commonalities in time frames, tattoo artists, or equipment among HIV-infected inmates who reported tattooing as their only risk behavior and to determine whether the association between tattooing and HIV seroconversion identified in this investigation is causal. Black race was significantly associated with HIV seroconversion, although no differences in risk behaviors were identified among racial groups. HIV disproportionately affects blacks in the general population, and 86% of males who were already infected with HIV when they entered GDC facilities were black. Black-only sex or tattooing networks might exist in prisons, given that 63% of all male inmates and 86% of HIV-infected men in GDC facilities are black. If so, then black race might be a marker in the analysis for the choice of sex or tattooing partners within these networks. Having a BMI of <25.4 kg/m2 also was significantly associated with HIV seroconversion, but the implications of this finding for HIV transmission and prevention are unclear. Although BMI was explored in the analysis as a physical characteristic associated with HIV seroconversion, insufficient data are available to determine whether a statistically significant association existed between lower BMI and reported rape. The findings in this report are subject to at least three limitations. First, risk behaviors might differ between seroconverters identified through voluntary HIV testing and those refusing voluntary HIV testing, limiting representativeness. Second, recall bias might have affected the reporting of HIV risk behaviors. Finally, although ACASI interviews were conducted to provide privacy and reduce social desirability bias, inmates might have inaccurately reported HIV risk behaviors because sex between inmates, sex with correctional staff, injection drug use, and tattooing are illegal or forbidden by policy in this prison system. In response to this investigation, GDC is evaluating options to modify existing HIV prevention education and house HIV-infected inmates in a limited number of facilities. Three state prison systems (Alabama, Mississippi, and South Carolina) house HIV-infected inmates in separate facilities to provide focused medical care. At least three other state prison systems (California, Florida, and Texas) house some HIV-infected inmates with advanced disease or those requesting separate housing in "centers of excellence" for medical care; HIV-negative and HIV-infected inmates mix for education, vocational training, religious, and other prison programs. However, separate housing of HIV-infected inmates is limited in that it 1) does not reduce the spread of other sexually transmitted, opportunistic, and bloodborne infections, 2) might increase the risk for tuberculosis outbreaks (9), 3) raises concerns about disclosure of inmates' HIV status and access to prison programs, and 4) does not prevent transmission by inmates who are unaware that they are infected or by HIV-infected corrections staff. No data are available on the effectiveness of separate housing for HIV-infected inmates as an HIV prevention strategy. Although this investigation was conducted in a single state prison system, incarcerated populations in other correctional settings are at risk for HIV infection, both while in prison and after release into the community. Corrections officials, in partnership with public health officials, should assess the adequacy of existing programs and services for incarcerated populations and develop strategies to reduce HIV infection, both in prisons and in the community. This recommendation is consistent with one recently issued by the Presidential Advisory Council on HIV/AIDS, which called for improved HIV prevention in U.S. prisons, jails, and correctional facilities (10). Acknowledgments This report is based, in part, on contributions by staff members of the Georgia Dept of Corrections; D Crippen, D Duran, MPH, Georgia Dept of Human Resources, Div of Public Health; L Cohen, MD, F Kamara, MD, MT Morgan, MD, Dept of Community Health and Preventive Medicine, Morehouse School of Medicine, Atlanta; Recovery Consultants of Atlanta, Inc.; Stand, Inc., Decatur, Georgia; S Broadwell, PhD, JT Brooks, MD, M Clay, F Cowart, M Ed, M Durham, MS, A Edwards, MA, V Goli, MPH, D Gnesda, MPH, K Henny, PhD, M Kalish, PhD, S McDougal, MD, SM Owen, PhD, B Parekh, PhD, RH Potter, PhD, J Prejean, PhD, L Reid, MS, S Richard, MPH, S Watson, K Williams, PhD, C Yang, PhD, A Youngpairoi, Div of HIV/AIDS Prevention, National Center for HIV, Hepatitis, STD and TB Prevention; S Bartley, MMSc, D Hemmerlein, Serum Bank, Div of Scientific Resources, Center for Prevention, Detection, and Control of Infectious Diseases; F Forna, MD, EIS Officer, CDC. References
* Black persons are disproportionately affected by HIV/AIDS. Although blacks represent 12% of the U.S. population, an estimated 43% of all persons living with AIDS in the United States are black (3). In Georgia, an estimated 76% of new AIDS cases reported in 2004 were among blacks (additional information is available at http://dhr.georgia.gov/DHR/DHR_FactSheets/AIDS%20in%20Georgia%20Jan%2006%20rev.pdf). Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 4/20/2006 |
|||||||||
|