Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Revised Guidelines for HIV Counseling, Testing,
and Referral
Please note: This guideline document is obsolete and may not reflect current evidence or best practice and likely contains out-of-date information. Updated information on this topic may be found here.
Technical Expert Panel Review of CDC
HIV Counseling, Testing, and Referral Guidelines
February 18--19, 1999
Atlanta, Georgia
Terje J. Anderson
National Association of People with AIDS
Washington, D.C.
David Atkins, M.D., M.P.H.
Agency for Healthcare Research and Quality
Rockville, Maryland
Catherine Baker-Cirac
California Office of AIDS
Sacramento, California
Ronald Bayer, Ph.D.
Columbia University
New York, New York
Frank K. Beadle de Palomo, M.A.
Academy for Educational Development
Washington, D.C.
Gail A. Bolan, M.D.
California Department of Health
Berkeley, California
Carol A. Browning, M.S.
Rhode Island Department of Health
Providence, Rhode Island
Scott Burris, J.D.
Temple University
Philadelphia, Pennsylvania
Amy S. DeGroff, M.P.H.
Centers for Disease Control and Prevention (CDC)
Atlanta, Georgia
John M. Douglas, M.D.
Denver Public Health
Denver, Colorado
Martin Fishbein, Ph.D.
University of Pennsylvania
Philadelphia, Pennsylvania
Alice A. Gandelman, M.P.H.
California STD Control Branch
Berkeley, California
Cynthia A. Getty
CDC
Atlanta, Georgia
Lawrence O. Gostin, J.D., L.L.D.
Georgetown University
Washington, D.C.
Khurram S. Hassan, M.P.H.
United Way of Metro Atlanta
Atlanta, Georgia
Thomas L. Hearn, M.S., Ph.D.
CDC
Atlanta, Georgia
Michael P. Johnson, M.D., M.P.H.
Health Resources and Services Administration
Rockville, Maryland
William J. Kassler, M.D., M.P.H.
New Hampshire Department of Health
& Human Services
Concord, New Hampshire
Marlene LaLota, M.P.H.
Florida Department of Health
Tallahassee, Florida
Michael K. Lindsay, M.D., M.P.H.
Emory University
Atlanta, Georgia
Michael H. Merson, M.D.
Yale University
New Haven, Connecticut
Stephen F. Morin, M.A., Ph.D.
University of California, San Francisco
San Francisco, California
James Pearson, M.P.H., Ph.D.
Division of Consolidated Laboratory Services
Richmond, Virginia
Beny J. Primm, M.D.
Urban Resources Institute
Brooklyn, New York
Joel Rosenstock, M.D., M.P.H.
Infectious Disease Solutions, P.C.
Atlanta, Georgia
Peter Salovey, Ph.D.
Yale University
New Haven, Connecticut
Charles A. Schable, M.S.
CDC
Atlanta, Georgia
Kathleen J. Sikkema, Ph.D.
Yale University
New Haven, Connecticut
Edith Springer, M.S.W.
Edith Springer Associates
Brooklyn, New York
Janis Spurlock-McLendon, M.S.W.
Connecticut Department of Public Health
Hartford, Connecticut
Lee Trevithick, M.A.
Cocoon House
Everett, Washington
James Welch
Division of Public Health
Dover, Delaware
The following CDC staff members prepared this report: Beatrice T. Divine, M.A.
Stacie M. Greby, D.V.M., M.P.H.
Kenneth V. Hunt
Mary L. Kamb, M.D., M.P.H.
Richard W. Steketee, M.D., M.P.H.
Lee Warner, M.P.H.
Division of HIV/AIDS Prevention --- Surveillance and Epidemiology
National Center for HIV, STD, and TB Prevention
in consultation with
Liisa M. Randall, M.A.
National Alliance of State and Territorial AIDS Directors
Summary
These guidelines replace CDC's 1994 guidelines,
HIV Counseling, Testing, and Referral Standards and
Guidelines, and contain recommendations for
public- and private-sector policy makers and service providers of
human immunodeficiency virus (HIV) counseling, testing, and referral (CTR). To
develop these guidelines, CDC used an evidence-based approach advocated by the
U.S. Preventive Services Task Force and public health practice guidelines.
The recommendations are based on evidence from all available scientific
sources; where evidence is lacking, opinion of "best practices" by specialists in the
field has been used.
This revision was prompted by scientific and programmatic advances in
HIV CTR, as well as advances in prevention and the treatment and care of
HIV-infected persons. These advances include a) demonstrated efficacy of
HIV prevention counseling models aimed at behavioral risk reduction; b)
effective treatments for HIV infection and opportunistic infections; c) effective
treatment regimens for preventing perinatal transmission; and d) new test technologies.
Although the new guidelines include many aspects of the previous ones
(e.g., encouragement of confidential and anonymous voluntary HIV testing, need
for informed consent, and provision of HIV prevention counseling that focuses
on the client's own risk), the new guidelines differ in several respects, including
giving guidance to all providers of voluntary HIV CTR in the public
and private sectors;
using an evidence-based approach to provide specific
recommendations for CTR;
underscoring the importance of early knowledge of HIV status and
making testing more accessible and available;
acknowledging providers' need for flexibility in implementing
the guidelines, given their particular client base, setting HIV prevalence
level, and available resources;
recommending that CTR be targeted efficiently through risk screening
and other strategies; and
addressing ways to improve the quality and provision of HIV CTR.
INTRODUCTION
Purpose of the Guidelines
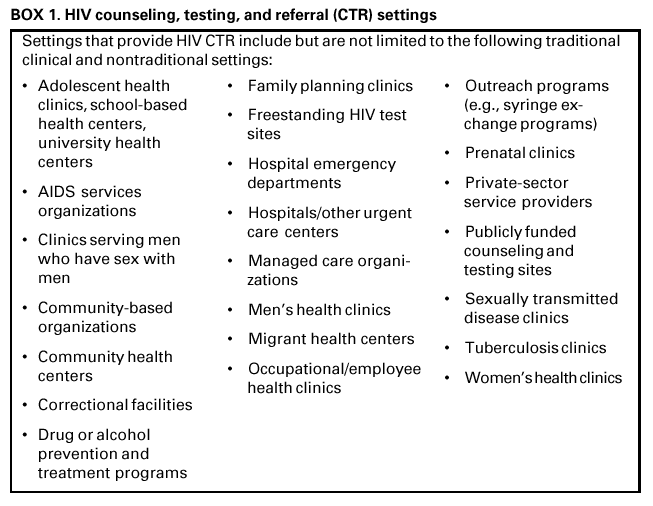
These guidelines were developed for policy makers and service providers in
the many settings that offer voluntary human immunodeficiency virus (HIV)
counseling,
testing, and referral (CTR) --- public and private, urban and rural, and those with
high and low HIV prevalence (Box 1). The guidelines are intended to be used to
develop CTR services and policies in traditional clinical settings (e.g., sexually
transmitted disease [STD] clinics, private physicians' offices) and nontraditional settings
(e.g., community-based or outreach settings [homeless shelters, bars]), which can
be important places to provide access to CTR to persons at increased HIV risk. The
Public Health Service is responsible for ensuring the quality of services in publicly
funded programs, and many aspects of these guidelines focus on such programs.
The guidelines could also be useful for CTR in other settings (e.g., for insurance,
military, and blood donation purposes). Recommendations should be tailored to fit the needs
of clients, communities, and programs within local, state, and federal rules
and regulations.
Evolution of the Guidelines
These guidelines revise and update several sets of CDC guidelines for HIV CTR.
The first CDC guidelines, published in 1986, highlighted the importance of
offering voluntary testing and counseling and maintaining confidential records
(1). In 1987, new guidelines emphasized the need to decrease barriers to counseling and
testing, especially disclosure of personal information
(2). In 1993, an additional report described the model of HIV prevention counseling currently recommended ---
an interactive rather than didactic model focusing on a personalized HIV
risk-reduction plan (3). In 1994, HIV Counseling, Testing and Referral Standards and
Guidelines focused on standard counseling and testing procedures and reiterated the
importance of the HIV prevention counseling model and the need for confidentiality of
counseling (4).
Because of recent advances in HIV treatment and prevention
(5--32, Revised Recommendations for HIV Screening of Pregnant
Women), CDC consulted with multiple partners to revise the 1994 guidelines using an evidence-based
approach (33,34) and to expand the target audience to all providers of HIV CTR in the
United States (33). Where scientific findings were lacking, recommendations were guided
by "best practices" from specialists in the field. These guidelines were developed
through the following five-step approach:
Address user needs. A survey was conducted of publicly funded sites that
offer HIV CTR to assess user satisfaction with the 1994 CDC guidelines for HIV
CTR. Internal and external content specialists were consulted on key areas to address.
Review scientific
literature. Approximately 5,000 abstracts were screened
and approximately 600 relevant publications were reviewed and synthesized
where appropriate. Approximately 20 previously published CDC guidelines related
to HIV CTR also were summarized.
Obtain technical opinion.
A panel of technical specialists from public and
private sectors; governmental and nongovernmental agencies; and legal, ethics,
and policy fields was convened to review the recommendations.
Obtain user input. Internal CDC comments, public and private
provider assessments, key consultant interviews, broad external reviews, and
public comments through the Federal Register were obtained.
Publish electronically and in hard
copy. Single copies of this report are
available from CDC's National Prevention Information Network (NPIN) website at
<http://www.cdcnpin.org> or by calling (800) 458-5231. The guidelines are also
available at the HIV Counseling, Testing, and Referral website at
<http://www.cdc.gov/hiv/ctr>. They will be updated and posted periodically.
Similarities and Differences Between Current and
Previous Guidelines
Aspects of previous CDC HIV guidelines that are unchanged include
encouraging availability of anonymous as well as confidential HIV testing;
ensuring that HIV testing is informed, voluntary, and consented;
emphasizing access to testing and effective provision of test results;
advocating routine recommendation of HIV CTR in settings (e.g., publicly
funded clinics) serving clients at increased behavioral or clinical risk for HIV infection;
recommending use of a prevention counseling approach aimed at personal
risk reduction for HIV-infected persons and persons at increased risk for HIV; and
stressing the need to provide information regarding the HIV test to all who
take the test.
Differences in the new guidelines include
giving guidance to all providers of voluntary HIV CTR in the public and
private sectors;
using an evidence-based approach to provide specific recommendations for CTR;
underscoring the importance of early knowledge of HIV status and making
HIV testing more accessible and available;
acknowledging providers' need for flexibility in implementing the
guidelines, given their particular client base, setting HIV prevalence level, and
available resources;
recommending that CTR be targeted efficiently through risk screening and
other strategies; and
addressing ways to improve the quality and provision of HIV CTR.
Advances in HIV/AIDS Prevention and Treatment Interventions
During the past 2 decades, HIV infection and severe HIV-related diseases
(e.g., acquired immunodeficiency syndrome [AIDS]) have become a leading cause of
illness and death in the United States. As of December 31, 2000, a total of 774,467
persons were reported with AIDS, and 448,060 of these persons had died; the number
of persons living with AIDS (322,865) was the highest ever reported
(35). Approximately
800,000--900,000 persons in the United States are infected with HIV,
and approximately 275,000 of these persons might not know they are infected
(36).
Since the last CTR guidelines were published, many advances have been made
in HIV/AIDS prevention and treatment, including development of effective
antiretroviral therapies that have reduced HIV-related illness and death. However, although
medical treatment has improved the quality and length of life for HIV-infected persons,
it cannot cure HIV disease. Furthermore, the successes of new medical therapies
might have led to relaxed attitudes toward safer sex (e.g., increased incidence
of unprotected anal sex by young men who have sex with men) by HIV-infected
persons and uninfected persons at increased risk
(36,37). Additional advances include improved understanding of HIV transmission; a wider array of HIV test
technologies; effective prevention counseling approaches; and practical, beneficial
referral strategies --- all of which could reduce the impact of the HIV epidemic in the
United States.
Early knowledge of HIV infection is now recognized as a critical component
in controlling the spread of HIV infection
(38). Cohort studies have demonstrated that many infected persons decrease behaviors that transmit infection to sex or
needle-sharing partners once they are aware of their positive HIV status
(39--46). HIV-infected persons who are unaware of their infection do not reduce risk behaviors
(42,47--49). Persons tested for HIV who do not return for test results might even increase their
risk for transmitting HIV to partners (50). Because medical treatment that lowers HIV
viral load might also reduce risk for transmission to others
(51), early referral to medical care could prevent HIV transmission in communities while reducing a person's risk
for HIV-related illness and death.
The array of HIV test technologies available has expanded, possibly enhancing
a person's willingness to be tested and learn his or her HIV status. HIV tests can
use specimens collected by less-invasive methods (e.g., oral fluid, urine, and
finger-stick blood), in addition to serum specimens collected by venipuncture. Rapid HIV
testing allows clients to receive results the same day, which is useful in urgent
medical circumstances and settings where clients tend not to return for HIV test results
(e.g., some STD clinics). HIV testing can also be conducted using commercially
available home sample collection devices
(52).
Also during the 1990s, randomized controlled trials demonstrated that, for
persons at increased HIV risk, certain prevention counseling approaches can be effective
in reducing high-risk behaviors and new sexually transmitted infections
(5,18--21). The counseling approach used is critical to effectiveness; interactive
counseling approaches directed at a client's personal risk and the situations in which risk
occurs are more effective than didactic, informational approaches
(5). Because personalized prevention counseling can require more provider time and training than
traditional counseling approaches, providing it to everyone receiving HIV testing might not
be feasible. This recognition has led to a new area of health services research
--- developing strategies that effectively target CTR services to persons most likely
to benefit from them.
The improved health of HIV-infected persons on antiretroviral therapy, along
with new test technologies and effective counseling approaches, has contributed to
an improved understanding of the importance of referral to needed services. In
addition,
new guidelines for partner counseling and referral services (PCRS)
(27) and prevention case management
(28) were developed specifically for publicly
funded clinics and could also be useful to providers in other settings. Specialists in the
field have also identified situations in which additional counseling or psychosocial
support services might benefit HIV prevention efforts. Finally, advances in several areas
have led to new guidelines for preventing mother-to-child transmission (see
Revised Recommendations for HIV Screening of Pregnant
Women), treating opportunistic infections
(23,53) and other sexually transmitted
(29) and bloodborne diseases (30--32), and managing occupational and nonoccupational exposure and
prophylaxis (54,55). These developments were considered in the formulation of the new
CTR guidelines.
Despite these advances in HIV prevention and care, a substantial number
of opportunities for HIV prevention through CTR are missed. At publicly funded
sites, approximately 70% of persons tested received their results and information
regarding the test, but fewer persons likely received HIV prevention counseling and referrals.
In private settings, a lower proportion of all clients are tested, and few
receive prevention counseling and referrals
(56--59). In many potential testing settings
(e.g., emergency departments), HIV prevention counseling and testing are not
uniformly offered, and data regarding types, completion, and effectiveness of referrals are
not routinely collected.
Goals of HIV CTR
Ensure that HIV-infected persons and persons at increased risk for HIV
have access to HIV testing to promote early knowledge of their HIV status;
receive high-quality* HIV prevention counseling to reduce their risk
for transmitting or acquiring HIV; and
have access to appropriate medical, preventive, and psychosocial
support services.
Promote early knowledge of HIV status through HIV testing and ensure that
all persons either recommended or receiving HIV testing are provided
information regarding transmission, prevention, and the meaning of HIV test results.
Principles of HIV CTR
Effective HIV CTR is based on the following principles:
Protect confidentiality of clients who are recommended or receive HIV
CTR services. Information regarding a client's use of HIV CTR services should
remain private (i.e., confidential). Personal information should not be divulged to
others in ways inconsistent with the client's original consent.
Obtain informed consent before HIV
testing. HIV testing should be voluntary and free of coercion. Informed consent before HIV testing is essential.
Information regarding consent may be presented orally or in writing and should
use language the client can understand. Accepting or refusing testing must not
have detrimental consequences to the quality of care offered. Documentation
of informed consent should be in writing, preferably with the client's
signature. State or local laws and regulations governing HIV testing should be followed.
Information regarding consent may be presented separately from or
combined with other consent procedures for health services (e.g., as part of a package
of tests or care for certain conditions). However, if consent for HIV testing
is combined with consent for other tests or procedures, the inclusion of HIV
testing should be specifically discussed with the client. For a discussion of HIV testing
in pregnant women, consult the guidelines for HIV screening of pregnant
women (see Revised Recommendations for HIV Screening of Pregnant
Women).
Provide clients the option of anonymous HIV
testing. Anonymous testing (i.e., consented voluntary testing conducted without a client's identifying
information being linked to testing or medical records, including the request for testing or
test results) has been used widely and effectively. Anonymous testing can benefit
the health of individual persons and the public by prompting earlier entry
into medical care (60). Persons who would otherwise not be tested might
seek anonymous HIV testing and learn their HIV status. Consistent with public
health best practices, states in which anonymous testing is not available
should reconsider their policy. When the client has no clear preference regarding
testing type, confidential testing (i.e., information documented in client's record)
should be recommended to promote receipt of test results and linkage to
follow-up counseling and referral for needed services. Clients opting for
anonymous testing should be informed that the provider cannot link the client's test result
to the client by name. Therefore, if the client does not return for test results,
the provider will not be able to contact the client with those results.
Provide information regarding the HIV test to all who are recommended
the test and to all who receive the test, regardless of whether
prevention counseling is provided. The information should include a description of ways
in which HIV is transmitted, the importance of obtaining test results, and
the meaning of HIV test results.
Adhere to local, state, and federal regulations and policies that govern
provision of HIV services. Laws at the local, state, and federal levels might
address aspects of HIV services or regulate how services are provided to
particular persons (e.g., minors). In addition, policies, local ordinances, funding
source requirements, and planning processes could also affect a provider's
decisions regarding which services to provide and how to provide them.
Provide services that are responsive to client and community needs
and priorities. Providers should work to remove barriers to accessing services
and tailor services to individual and community needs. To ensure that clients
find services accessible and acceptable, services can be offered in
nontraditional settings (i.e., community-based or outreach settings); hours of operation can
be expanded or altered; unnecessary delays can be eliminated (e.g.,
integrating counseling and testing for STDs/HIV with counseling and testing for
hepatitis); test results can be obtained more easily (e.g., with rapid testing or by
telephone in certain situations); and less-invasive specimen collection can be used
(e.g., oral fluid, urine, or finger-stick blood).
Provide services that are appropriate to the client's culture, language,
sex, sexual orientation, age, and developmental
level. These factors could affect how the client seeks, accepts, and understands HIV services. Providers
should consider these factors when designing and providing HIV services to
increase the likelihood of return for test results and acceptance of counseling and
referral services.
Ensure high-quality
services. To ensure ongoing, high-quality services that
serve client and community needs, providers should develop and implement
written protocols for CTR and written quality assurance and evaluation
procedures. Many state and local health departments have substantial expertise in
providing and monitoring the quality of HIV CTR services and can be a resource to
private providers or community-based or outreach settings initiating these services.
TARGETED VERSUS ROUTINELY RECOMMENDED HIV CTR
Providers in all settings (traditional and nontraditional) should ideally
recommend CTR to all clients on a routine basis to ensure that all clients who could benefit
from CTR receive these services. However, resources might be insufficient to permit
this practice. Therefore, these guidelines contain recommendations aimed at ensuring
that as many persons as possible who are HIV-infected or at risk for HIV who do not
know their HIV status have access to testing, prevention counseling, and referrals.
Routinely Recommending CTR to All Clients Versus
Targeting CTR to Selected Clients
Studies have documented that, in settings serving clients at increased
behavioral and clinical risk for HIV infection, targeting HIV testing based on reported risk
factors will miss many HIV-infected clients
(61--69). However, in low prevalence
settings, where most clients have minimal risk, targeting clients for HIV testing based on
risk screening might be more feasible for identifying small numbers of
HIV-infected persons (70). Providers should consider three factors in determining whether
to recommend HIV CTR to all clients or to target only selected clients.
Type of setting.
HIV prevalence of the setting.
Behavioral and clinical HIV risk of the individual clients in the setting.
Although certain types of settings serve populations at increased risk (e.g.,
STD clinics), others might serve individual clients at increased risk (e.g., private
physicians'
offices in areas of low prevalence). Individual risk can be ascertained through
risk screening. Under certain circumstances --- perinatal transmission, acute
occupational exposure, and acute nonoccupational (i.e., high-risk sexual or
needle-sharing) exposure --- providers should recommend HIV CTR regardless of setting prevalence
or behavioral or clinical risk, based on the respective guidelines
(Revised Recommendations for HIV Screening of Pregnant
Women,54,55).
Using Prevalence Data to Establish Service Priorities
Few data exist to define "high" and "low" HIV prevalence and describe how
these definitions could help develop and prioritize HIV CTR services. A study conducted in
the early 1990s for acute care hospitals with
>1% HIV prevalence reported that routine voluntary HIV testing of all patients within a specific age range could be a feasible
way to identify a large proportion of HIV-infected patients
(71). This 1% prevalence can be used as general guidance for whether to routinely recommend or target
HIV counseling and testing in other settings.
The threshold of HIV prevalence that should lead to routine recommendations
for HIV testing of all clients within a setting can vary within and across settings and
should be set in consideration of available resources. Services could be
routinely recommended in settings with HIV prevalence rates <1% but higher than
other settings in the community, according to U.S. prevalence data
(72). If HIV prevalence data are outdated or unknown, providers should consult their local or state
health department for assistance in determining appropriate HIV CTR
strategies. Alternatively, providers could employ routine voluntary testing to obtain
information on prevalence in their particular settings.
Because of the availability of antiretroviral therapy to reduce the risk for
perinatal HIV transmission, all pregnant women should be recommended HIV testing
regardless of setting prevalence or behavioral or clinical risk (see
Revised Recommendations for HIV Screening of Pregnant
Women).
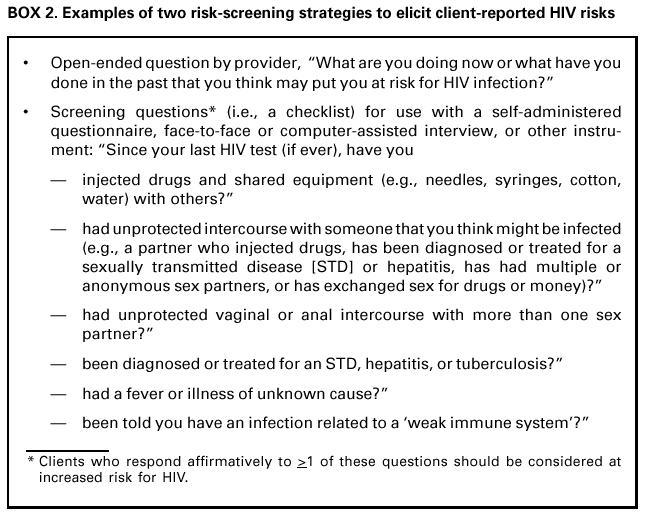
Determining Individual HIV Risk Through Risk Screening**
A client's individual HIV risk can be determined through risk screening based
on self-reported behavioral risk (Box 2) and clinical signs or symptoms. Behavioral
risks include injection-drug use or unprotected intercourse with a person at increased
risk for HIV. Clinical signs and symptoms include STDs, which indicate increased risk
for HIV infection, or other signs or symptoms (e.g., of acute retroviral or
opportunistic infections), which might suggest the presence of HIV infection. Insufficient data exist
to support the efficacy of any one risk-screening approach over others (e.g.,
face-to-face discussion or interviews, self-administered questionnaires,
computer-assisted interviews, or simple open-ended questions asked by providers) (Box 2)
(61,70).
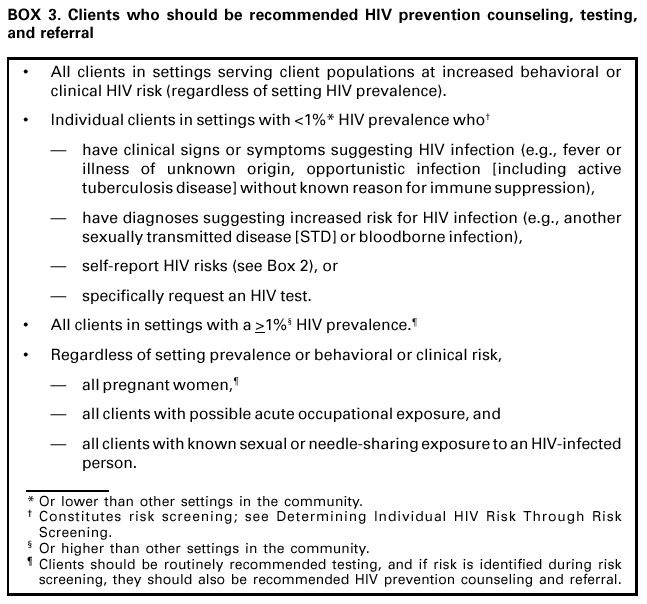
Recommendations for Routinely Recommended and
Targeted CTR by Setting and Circumstance
Decisions regarding whether to recommend routine or targeted services are
based on the behavioral and clinical HIV risk of the client population in the setting, the level
of
HIV prevalence of the setting, and the behavioral and clinical HIV risk of
individual clients (Box 3). These factors should not be used to determine recommendations
for CTR in circumstances in which treatment potential exists (i.e., perinatal
transmission and acute occupational or nonoccupational exposure).
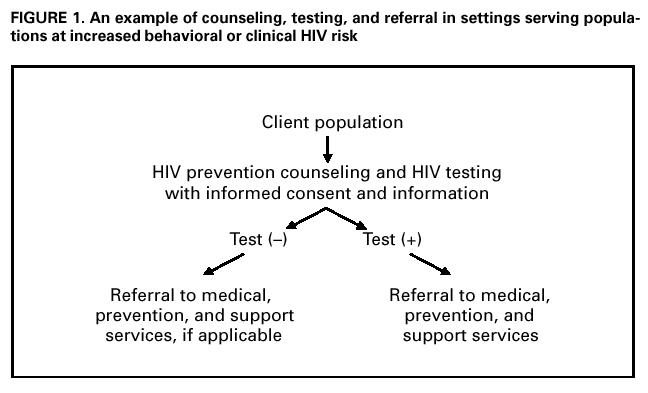
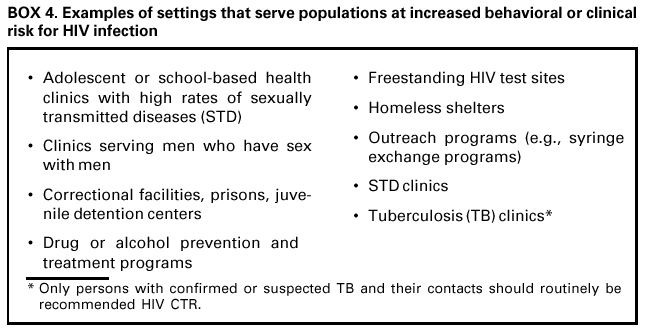
Settings Serving Populations at Increased Behavioral or Clinical Risk
HIV CTR should be routinely recommended for all clients in settings where
the client population is at increased behavioral or clinical risk for acquiring or
transmitting HIV infection, regardless of setting prevalence (Box 4 and Figure 1). These
services should be provided on-site. In these settings, clients with ongoing risk behaviors
should be linked to additional HIV prevention and support services (e.g., PCRS, drug or
alcohol prevention and treatment), as appropriate. HIV-infected clients should receive
ongoing HIV prevention counseling applicable to their personal situation.
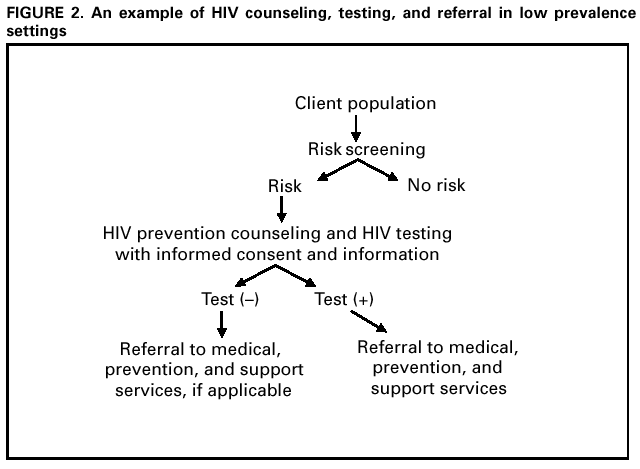
Low Prevalence Settings
In low prevalence settings (e.g., <1%, see Using Prevalence Data to
Establish Service Priorities) where the client population is generally not at increased
behavioral or clinical HIV risk, CTR should be targeted to clients based on risk screening (Figure 2). Prevention counseling and referral are recommended for persons at increased
risk even if HIV testing is declined. Any client who requests HIV testing should receive
it, regardless of risk. These settings likely represent most health-care settings.
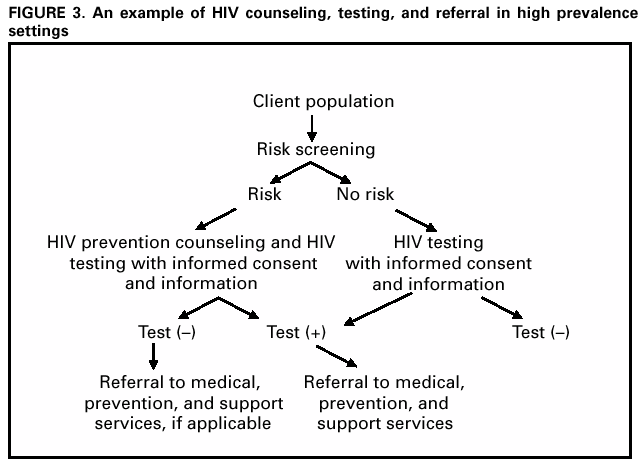
High Prevalence Settings
In high prevalence settings (e.g., >1%), all clients should be routinely
recommended HIV testing (Figure 3). Risk screening should be used to determine if HIV
prevention counseling and referral should also be recommended. CTR should be provided
on-site. In these settings, clients with ongoing risk behaviors identified during risk
screening should be linked to additional HIV prevention and support services (e.g., PCRS
and drug or alcohol prevention and treatment), as appropriate.
Circumstances For Which HIV Preventive Treatment Exists
Prophylaxis exists for a limited number of situations: perinatal transmission,
acute occupational exposure, and acute nonoccupational (i.e., high-risk sexual or
needle-sharing) exposure. Regardless of population risk, setting prevalence, or
individual behavioral or clinical risk, voluntary HIV testing should be routinely recommended
to a) all pregnant women, b) clients with acute occupational exposure, and c) clients
with acute nonoccupational (e.g., high-risk sexual or needle-sharing) exposure.
Regardless of whether a client receives an HIV test, HIV prevention counseling and referral
should target pregnant women based on risk screening and be routinely recommended
to clients with either acute occupational or nonoccupational exposures. For
further information, consult the respective guidelines on perinatal transmission,
acute occupational exposure, and acute nonoccupational exposure
(Revised Recommendations for HIV Screening of Pregnant
Women,54,55).
A Framework for Implementing HIV CTR
CTR are interrelated interventions that ideally should be integrated and offered
in all settings. However, these guidelines acknowledge public and private
providers' needs for flexibility. Certain providers might be able to offer prevention counseling
but not an HIV test, whereas others might be able to offer an HIV test but not
prevention counseling. Although all providers in settings serving populations at
increased behavioral or clinical risk for HIV (e.g., STD clinics) should provide HIV CTR on-site,
not all can. These providers should maintain clear and appropriate methods of referral
to providers of prevention counseling or testing elsewhere. To ensure client
referral, providers who offer HIV counseling and testing should collaborate with
providers serving populations at increased risk for HIV who might not provide these services.
HIV COUNSELING
HIV counseling seeks to reduce HIV acquisition and transmission through
the following:
Information. Clients should receive information regarding HIV transmission
and prevention and the meaning of HIV test results. Provision of information
is different from informed consent.
HIV prevention
counseling. Clients should receive help to identify the
specific behaviors putting them at risk for acquiring or transmitting HIV and commit
to steps to reduce this risk. Prevention counseling can involve
>1 sessions.
Information
All clients who are recommended or who request HIV testing should receive
the following information, even if the test is declined:
Information regarding the HIV test and its benefits and consequences.
Risks for transmission and how HIV can be prevented.
The importance of obtaining test results and explicit procedures for doing so.
The meaning of the test results in explicit, understandable language.***
Where to obtain further information or, if applicable, HIV prevention counseling.
Where to obtain other services (see Typical Referral Needs).
In certain settings where HIV testing is offered, other useful information includes
a) descriptions or demonstrations of how to use condoms correctly; b)
information regarding risk-free and safer sex options
(73); c) information regarding other
sexually transmitted and bloodborne diseases; d) descriptions regarding the effectiveness
of using clean needles, syringes, cotton, water, and other drug paraphernalia;
e) information regarding drug treatment; and f) information regarding the possible
effect of HIV vaccines on test results for persons participating in HIV vaccine trials
(see Additional Counseling Considerations for Special Situations and Positive HIV
Test Results).
For efficiency, information can be provided in a pamphlet, brochure, or video
rather than a face-to-face encounter with a counselor. This approach allows the provider
to focus face-to-face interactions on prevention counseling approaches proven
effective with persons at increased risk for HIV infection. Information should be provided in
a manner appropriate to the client's culture, language, sex, sexual orientation, age,
and developmental level. Certain informational videos and large-group presentations
that provide explicit information regarding correct use of condoms have proven effective
in reducing new STDs (19--21,74) and could be effective in reducing HIV.
HIV Prevention Counseling
HIV prevention counseling should focus on the client's own unique
circumstances and risk and should help the client set and reach an explicit behavior-change goal
to reduce the chance of acquiring or transmitting HIV. HIV prevention counseling
is usually, but not always, conducted in the context of HIV testing. The
client-centered**** HIV prevention counseling model involves two brief sessions
(4,5,75), whereas other effective models are longer or involve more sessions
(5--8,10,11,13--18,76--79). Regardless of the model used, in HIV prevention counseling, the counselor or
provider focuses on assessing the client's personal risk or circumstances and helping the
client set and reach a specific, realistic, risk-reduction goal. These guidelines avoid using
the terms "pretest" and "posttest" counseling to underscore that prevention counseling
is a risk-reduction process that might involve only one or >1 session.
Several models for HIV prevention counseling in conjunction with HIV testing
have been developed, evaluated in controlled studies, and documented to be efficacious
in changing behavior or reducing sexually transmitted infections, including
individual face-to-face counseling (5,12), large- and small-group counseling with a
facilitator (6,16,18,79), and video-based counseling
(19). For more information regarding interventions, see
The Compendium of HIV Prevention Interventions with Evidence
of Effectiveness at <http://www.cdc.gov/hiv/pubs/hivcompendium.pdf>.
Client-Centered HIV Prevention Counseling
Since 1993, CDC has recommended one interactive counseling model, called
client-centered HIV prevention counseling
(3,4), which involves two face-to-face
sessions with a provider or counselor
(3--5,75,80). This model has traditionally used a
two-step HIV testing approach in which clients are physically present at a setting for the HIV
test (initial session) and then return for HIV test results (follow-up session). Each
session might require 15--20 minutes (including testing and referral) for clients at
increased risk for HIV, but could take only a few minutes for those at lower risk. In the
first session, a personalized risk assessment***** encourages clients to identify,
understand, and acknowledge the behaviors and circumstances that put them at increased risk
for acquiring HIV. The session explores previous attempts to reduce risk and
identifies successes and challenges in these efforts. This in-depth exploration of risk allows
the counselor to help the client consider ways to reduce personal risk and commit to
a single, explicit step to do so. In the second session, when HIV test results are
provided, the counselor discusses the test results, asks the client to describe the
risk-reduction
step attempted (and acknowledges positive steps made), helps the client identify
and commit to additional behavioral steps, and provides appropriate referrals (e.g.,
to PCRS).
In one large, randomized, controlled trial, this model was reported to be
effective at reducing high-risk sexual behaviors and new STDs
(5);
feasible to use even in busy publicly funded clinics;
acceptable to clients, counselors, and health-care providers
(80); and
cost-effective at preventing STDs in persons at increased risk for HIV
(81--83).
The model was reported to be especially effective among adolescents and
persons with ongoing sexual risk behaviors (e.g., newly diagnosed STDs)
(5). Although the benefits of client-centered HIV prevention counseling in reducing high-risk
drug behaviors are unknown, studies have indicated that similar counseling
approaches that help clients explore risks and set specific risk-reduction goals reduce risky
drug use behaviors (39--41,84).
Observational studies and reviews of programs in various settings have
indicated that many counselors are still unfamiliar with the specific goals of the
client-centered HIV prevention counseling model
(75,85) (Amy S. DeGroff, M.P.H., written communication, 2000). Because "client-centered" is sometimes misinterpreted
as "face-to-face," providers in many HIV test sites deliver face-to-face
informational messages in response to a generic checklist risk assessment. This type of
counseling provides advice rather than encouraging client participation or discussion of
personal risk; it seldom focuses on personal goal setting. "Client-centered" can also
be misinterpreted to mean that the counselor should avoid directing the session.
Although attentive listening and respect for clients' concerns are important elements of
effective counseling, the primary goal of client-centered HIV prevention counseling is
risk reduction. HIV prevention counseling usually requires provider training and
support and ongoing quality assurance to achieve optimal benefit. Providers can contact
their state health department's HIV/AIDS program office for information on local
training opportunities. For information on client-centered counseling with rapid testing,
see Addressing Barriers to HIV Prevention Counseling.
Elements of HIV Prevention Counseling
Regardless of the HIV prevention counseling model used, some
counseling elements have been used repeatedly in effective interventions and are recognized
by many specialists as critical in counseling success (Technical Expert Panel Review
of CDC HIV Counseling, Testing, and Referral Guidelines; February 18--19, 1999;
Atlanta, Georgia).
The following elements should be part of all HIV prevention counseling sessions:
Keep the session focused on HIV risk
reduction. Each counseling session should be tailored to address the personal HIV risk of the client rather than providing
a predetermined set of information. Although counselors must be willing
to address problems that pose barriers to HIV risk reduction (e.g., alcohol use
in certain situations), counselors should not allow the session to be distracted
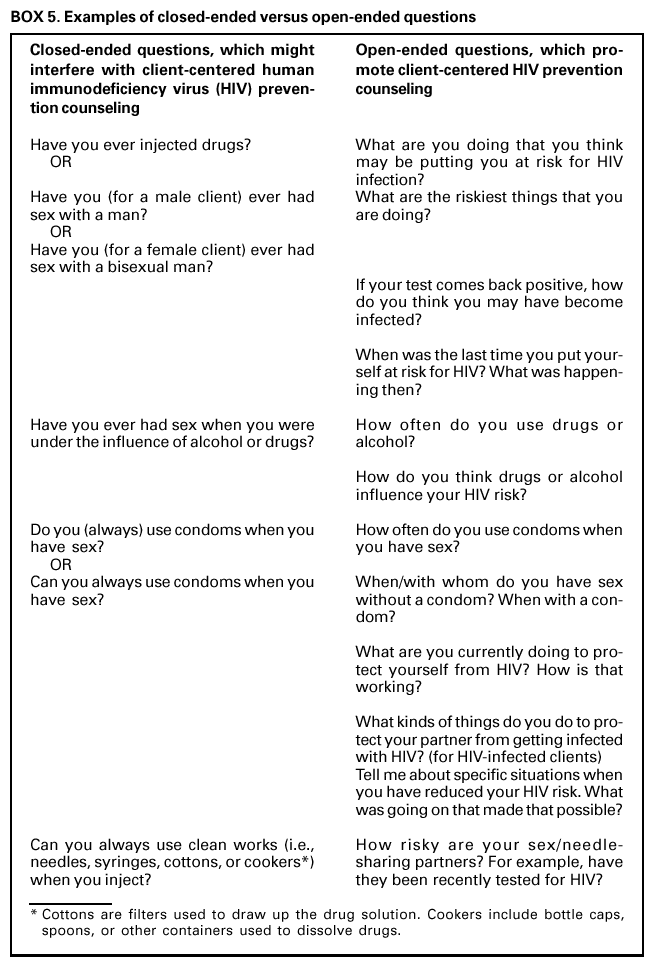
by the client's additional problems unrelated to HIV. Certain counseling
techniques (e.g., open-ended questions [Box 5], role-play scenarios, attentive listening, and
a nonjudgmental and supportive approach) can encourage the client to
remain focused on personal HIV risk reduction.
Include an in-depth, personalized risk
assessment. Sometimes called "enhancing self-perception of risk," risk assessment allows the counselor
and client to identify, acknowledge, and understand the details and context of
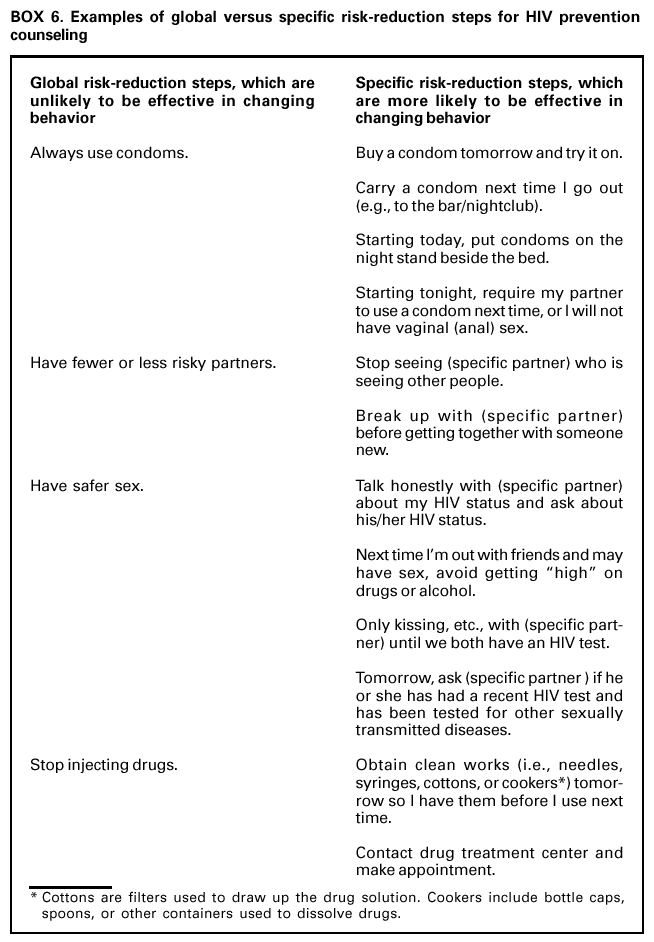
the client's HIV risk (17,86,87). Keeping the assessment personal, instead of
global, will help the client identify concrete, acceptable protective measures to
reduce personal HIV risk (Box 6). The risk assessment should explore previous
risk-reduction efforts and identify successes and challenges in those efforts.
Factors associated with continued risk behavior that might be important to
explore include using drugs or alcohol before sexual activity, underestimating
personal risk, perceiving that precautionary changes are not an accepted peer
norm, perceiving limited self-efficacy for successful change efforts,
receiving reinforcement for frequent unsafe practices (e.g., a negative HIV test result
after risk behaviors), and perceiving that vulnerability is associated with "luck"
or "fate" (86--89).
Acknowledge and provide support for positive steps already
made. Exploring previous risk-reduction efforts is essential for understanding the strengths
and challenges faced by the client in reducing risk. Support for positive steps
already taken increases the clients' beliefs that they can successfully take further
HIV risk-reduction steps. For some clients, simply agreeing to an HIV test is
an important step in reducing risk (5,75).
Clarify critical rather than general
misconceptions. In most situations, counselors should focus on reducing the client's current risk and
avoid discussions regarding HIV transmission modes and the meaning of HIV
test results. However, when clients believe they have minimal HIV risk but
describe more substantial risk, the counselor should discuss the HIV transmission
risk associated with specific behaviors or activities the clients describe and
then discuss lower-risk alternatives (73). For example, if clients indicate that
they believe oral sex with a risky sex partner poses little or no HIV risk, the
counselor can clarify that, although oral sex with an infected partner might result in
lower HIV transmission risk than anal sex, oral sex is not a risk-free
behavior, particularly when commonly practiced. If clients indicate that they do not need
to be concerned about HIV transmission among needle-sharing partners if they
use clean needles, the counselor can clarify that HIV can be transmitted through
the cooker, cotton, or water used by several persons sharing drugs. With
newly identified or uninformed HIV-infected clients, the counselor should discuss
HIV transmission risks associated with specific sexual or drug-use activities,
including those in which the client might not be currently engaged.
Negotiate a concrete, achievable behavior-change step that will reduce
HIV risk. Although the optimal goal might be to eliminate HIV risk behaviors,
small behavior changes can reduce the probability of acquiring or transmitting
HIV. Behavioral risk-reduction steps should be acceptable to the client
and appropriate to the client's situation. For clients with several high-risk
behaviors, the counselor should help clients focus on reducing the most critical risk they
are willing to commit to changing. The step does not need to be a personal
behavior change. For many clients, knowledge of a partner's recent HIV status (and
talking with the partner about getting an HIV test) might be more critical than
personal behavior changes. The step should be relevant to reducing the client's own
HIV risk and should be a small, explicit, and achievable goal, not a global goal
(Box 6). Identifying the barriers and supports to achieving a step, through
interactive discussion, role-play modeling, recognizing positive social supports, or
other methods will enhance the likelihood of success
(90). Writing down the goal might be useful. For clients with ongoing risk behaviors, referral to
additional prevention and support services is encouraged.
Seek flexibility in the prevention approach and counseling
process. Counselors should avoid a "one-size-fits-all" prevention message (e.g., "always
use condoms"). Behaviors that are safe for one person might be risky for
another (91). For example, unprotected vaginal intercourse might be unsafe
with anonymous partners whose HIV status is unknown, but safe for
uninfected persons in a mutually monogamous relationship. The length of
counseling sessions will vary depending on client risk and comfort (e.g., adolescents
might require more time than adults).
Provide skill-building
opportunities. Depending on client needs, the
counselor can demonstrate or ask the client to demonstrate problem-solving
strategies such as a) communicating safer sex commitments to new or continuing
sex partners; b) using male latex condoms properly; c) trying alternative
preventive methods (e.g., female condoms); d) cleaning drug-injection equipment if
clean syringes are unavailable; or e) communicating safer drug-injection
commitments to persons with whom the client shares drug paraphernalia
(86,92--94).
Use explicit language when providing test
results. Test results should be provided at the beginning of the follow-up session. Counselors should never
ask the client to guess the test results. Technical information regarding the test
can be provided through a brochure or other means so the session can focus
on personal HIV risk reduction for clients with negative tests and
other considerations for clients with positive or indeterminate test results
(see Additional Counseling Considerations for Special Situations). In-depth,
technical discussions of the "window period (i.e., the time from when a person is
infected until they develop detectable HIV antibody) should be avoided because
they could confuse the client and diffuse the importance of the HIV
prevention message. Counselors should clarify that negative test results do not mean
the client has no HIV risk and work with the client to reconsider ongoing HIV
risk behaviors and the benefits of taking steps to reduce those risks. A client
with ongoing risk behaviors should not be given a false sense of the safety of
those behaviors (i.e., avoid statements like "whatever you were doing seems to
be safe" or "continue to do whatever you are doing now").
These counseling elements are considered necessary for high-quality
counseling. Specialists in the field (Technical Expert Panel Review of CDC HIV Counseling,
Testing, and Referral Guidelines; February 18--19, 1999; Atlanta, Georgia) also
suggested adoption of the following:
Ensure that the client returns to the same
counselor. Consistency of the client and counselor relationship helps the client feel secure,
reduces misunderstanding, and promotes the likelihood of effective risk
reduction. Effective counseling models tended to use the same counselor for all
sessions. When follow-up prevention counseling sessions must be provided by a
different counselor, careful record-keeping is recommended to ensure
high-quality counseling. See The Compendium of HIV Prevention Interventions with
Evidence of Effectiveness at <http://www.cdc.gov/hiv/pubs/hivcompendium.pdf>.
Use a written protocol to help counselors conduct effective
sessions. A structured protocol outlining session goals can help keep the counselor
focused on risk reduction. The protocol can include examples of open-ended questions
(to help a new counselor avoid closed-ended questions) and a list of explicit
risk-reduction steps (to help a new counselor avoid accepting a client's suggestion
of global risk-reduction steps) (95).
Ensure ongoing support by supervisors and
administrators. Supervisory support is essential for effective counseling. Training in HIV counseling approaches
that focus on personal risk reduction is recommended for persons
supervising counselors. Staff appraisals should acknowledge that completion of
critical counseling elements has higher priority than completion of paperwork.
Avoid using counseling sessions for data
collection. If required, paperwork should be completed at the end of the counseling session or by staff
members who are not counseling. Checklist risk assessments driven by data
collection forms are detrimental to effective counseling because they can encourage
even skilled counselors to use closed-ended questions, limit eye contact, and
miss critical verbal and nonverbal cues. The relevance of any routinely collected
data should be periodically assessed.
Avoid providing unnecessary
information. An emphasis on providing
information might prompt counselors to miss critical HIV prevention opportunities and
cause clients to lose interest. Discussion of theoretical HIV risks (e.g., sex with a
person with hemophilia or needle exposures through tattoos) tends to shift the
focus away from the client's actual HIV risk situations to topics that are
more "comfortable" or easy to discuss but irrelevant to the client's risk.
Who Should Deliver Prevention Counseling
In any setting where HIV testing is provided, existing personnel can be
effective counselors if they have the desire and appropriate training and employ the
essential counseling elements (5,80). Advanced degrees or extensive experience are
not necessary for effective HIV prevention counseling, though training is
(80). Training in counseling is available (see Ensuring High-Quality HIV Prevention Counseling).
In situations where primary health-care providers (e.g., physicians) might not be able
to provide prevention counseling, auxiliary health professionals trained in HIV
prevention counseling models can provide this service. Although peer counseling has
been successful in certain situations (18), research does not support an explicit
risk-reduction need or benefit to matching clients with counselors based on same or
similar backgrounds, sex, ethnicity, age, or peer group for intervention efficacy
(96--98). The following skills and counselor characteristics were identified by specialists in the
field as important for effective HIV prevention counseling (Technical Expert Panel Review
of CDC HIV Counseling, Testing, and Referral Guidelines; February 18--19, 1999;
Atlanta, Georgia):
Completion of standard training courses in client-centered HIV
prevention counseling or other risk-reduction counseling models.
Belief that counseling can make a difference.
Genuine interest in the counseling process.
Active listening skills.
Ability to use open-ended rather than closed-ended questions (Box 5).
Ability and comfort with an interactive negotiating style rather than a
persuasive approach.
Ability to engender a supportive atmosphere and build trust with the client.
Interest in learning new counseling and skills-building techniques.
Being informed regarding specific HIV transmission risks
(73).
Comfort in discussing specific HIV risk behaviors (i.e., explicit sex or
drug behaviors).
Ability to remain focused on risk-reduction goals.
Support for routine, periodic, quality assurance measures.
Additional Counseling Considerations for Special Situations
Persons with newly identified HIV
infection. Clients with newly identified HIV infection have immediate and long-term needs. Some clients might be
better prepared to receive positive test results than others. The emotional impact
of hearing an HIV-positive test result might prevent clients from
clearly understanding information during the session in which they receive their
results. Providers should provide appropriate referrals (see Typical Referral Needs)
and, when necessary, additional sessions.
When a client receives the test result, the provider should ensure that the
client understands it. As part of HIV prevention counseling, providers should
explicitly discuss and clarify any misconceptions regarding HIV transmission risk
to partners associated with specific sexual or needle-sharing activities.
Clients should be advised to refrain from donating blood, plasma, or organs.
For sexually active clients who are not in mutually monogamous
partnerships, providers should also address strategies to prevent other sexually
transmitted or bloodborne infections (e.g, gonorrhea, syphilis, chlamydia, herpes
simplex virus, human herpes virus type 8 [the virus linked to Kaposi sarcoma], hepatitis
B virus, hepatitis C virus, and cytomegalovirus).
The first few months after persons learn they are HIV infected are important
for accessing medical and other support services to help them obtain treatment
and establish and maintain behavior changes that reduce the likelihood
of transmitting the virus to others. For example, persons with ongoing risks
might be referred for prevention counseling to prevent transmission to others or
for prevention case management. For all newly identified clients, a
follow-up appointment 3--6 months after diagnosis is recommended by some
specialists (99) to assess whether clients were able to initiate medical care,
minimize transmission risk to uninfected partners, and access other needed services
(e.g., partner counseling and referral services). See guidance on partner
counseling and referral services (27) and prevention case management
(28).
Persons with a single, recent nonoccupational HIV
exposure. After a reported sexual, injection-drug use, or other nonoccupational exposure to HIV
(55), providers should refer clients for prompt initiation of evaluation, counseling,
and follow-up services. Early postexposure prophylaxis could reduce the likelihood
of becoming infected with HIV, although the degree to which early treatment
can prevent new infection after acute nonoccupational HIV exposure is
unclear. Further guidance on nonoccupational HIV exposure is available
(55).
Persons with indeterminate HIV test
results. Until follow-up test results are available, persons with an indeterminate result should receive
information regarding the meaning of test results. HIV prevention counseling should be
the same as for a person with newly identified HIV infection. Behaviors that
minimize the risk for HIV transmission to sex and needle-sharing partners should
be emphasized, even if the client reports no risk behaviors. Clients with
repeated indeterminate test results >1 month apart are unlikely to be HIV-infected and
can be provided test results in the same way as clients with negative test
results, unless recent HIV exposure is suspected (see Indeterminate Test Results).
Persons seeking repeat HIV
testing. In addition to brief prevention
counseling sessions, ongoing HIV prevention counseling aimed at personal risk
reduction might be useful for persons seeking repeated HIV testing who have
continued HIV risk. Counselors should encourage clients to explore alternative
prevention strategies and to identify and commit to additional risk-reduction steps.
Clients with ongoing risk behaviors might benefit from referral to other HIV
prevention and support services because their current risk behavior might be reinforced
by repeated negative HIV test results or they might view HIV testing as
protective (100). More information on prevention case management is available
(28) (see Ongoing Exposure).
Persons who use drugs. Persons who inject drugs might also be at increased
risk for acquiring HIV through unprotected sex with an HIV-infected partner
(101--103). For injection-drug users (IDUs), intervention studies indicate
that personalized, interactive prevention counseling models using
goal-setting strategies might be effective in reducing injection-drug and sexual-risk
behaviors (39--41,84). Evidence also supports the efficacy of community strategies
(e.g., methadone maintenance programs or other drug treatment programs,
outreach programs, and syringe exchange) to reduce new HIV infections among
IDUs (104--108). Specialists in the field advocate recommending such strategies,
along with individual HIV prevention counseling, to persons who inject drugs.
Sex or needle-sharing partners of HIV-infected
persons. Sex or needle-sharing partners of HIV-infected persons should be encouraged to have HIV
prevention counseling and testing. Partners who are HIV discordant (i.e., one person is
HIV-infected and the other is uninfected) should receive counseling aimed
at preventing HIV transmission from the infected to the uninfected
partner, including explicit discussion and clarification of any misconceptions
regarding HIV transmission risk associated with specific sexual or needle-sharing
activities. In addition, many HIV-discordant couples benefit from ongoing HIV
prevention counseling aimed at personal risk reduction or from couples counseling
that teaches safe sexual practices and proper condom use
(27,109--111). Little evidence exists to conclusively support or refute whether simultaneous
infection with >2 subtypes of HIV is likely to occur or, if it does, whether it is
associated with more aggressive or resistant disease
(112). Researchers are divided on the value of recommending consistent condom use to prevent HIV sequelae
for mutually monogamous, HIV-infected partners.
Health-care workers after an occupational
exposure. After an occupational exposure, health-care workers should use measures to prevent
transmission during the follow-up period
(54). HIV-exposed health-care workers should
be advised that, although HIV is infrequently transmitted through an
occupational exposure, they should abstain from sex or use condoms and avoid
pregnancy until they receive a negative follow-up test result. In addition, they should
not donate blood, plasma, organs, tissue, or semen; if a woman is
breast-feeding, she should consider discontinuing (54). Health-care workers should also
be advised of the rationale for postexposure prophylaxis, the risk for
occupationally acquired HIV infection from the exposure, the limitations of current knowledge
of the efficacy of antiretroviral therapy when used as postexposure
prophylaxis, the toxicity of the drugs involved, and the need for postexposure
follow-up (including HIV testing), regardless of whether antiretroviral therapy is
taken. Further guidance on occupational HIV exposure is available
(54).
Participants in HIV vaccine
trials. HIV-vaccine--induced antibodies may be detected by current HIV tests and may cause a false-positive result.
Trial participants should be advised that HIV CTR is best provided at the vaccine
trial sites, the vaccine is of unknown efficacy, and HIV risk behavior can result in
their becoming HIV-infected (see Positive Test Results).
Addressing Barriers to HIV Prevention Counseling
Several factors can prevent provision of high-quality HIV prevention
counseling, including unavailability of trained prevention counselors at the setting in which the
HIV test was conducted, client reluctance, and low rates of client return for test
results. Recommended strategies for addressing these common barriers include a)
providing counseling on-site, b) enhancing client acceptance of counseling by examining
and improving the counseling provided, and c) considering alternate counseling methods.
Provide On-Site Counseling
Cost, lack, or turnover of trained staff members and space constraints are
barriers to providing HIV prevention counseling
(113). However, given the proven efficacy
of prevention counseling models, in settings where HIV prevalence is high or
the population served is at increased risk, the ability to provide such counseling on-site is
a high priority, and efforts should be made to address and remove barriers to
providing HIV prevention counseling on-site. Health educators or other auxiliary staff
members trained to discuss preventive activities such as healthy eating, prenatal education,
or smoking cessation could, if adequately trained, be effective HIV prevention
counselors. In the interim, alternative resources should be identified, and clearly defined
referrals should be made to settings that can provide high-quality prevention counseling
for clients at increased HIV risk. Systems to ensure that referrals are completed should
be established (see HIV Referral).
Enhance Client Acceptance of HIV Prevention Counseling
Clients who agree to HIV testing but decline HIV prevention counseling often
report they lack time or already are aware of HIV transmission modes.
However, experienced counselors report that clients mainly refuse counseling because they
do not perceive the service to be personally beneficial (Technical Expert Panel Review
of CDC HIV Counseling, Testing, and Referral Guidelines; February 18--19, 1999;
Atlanta, Georgia). These counselors believe that most of these clients are concerned about
a specific risk, which they would be willing to explore if the counseling seemed
useful. Three of the most commonly reported barriers to the perceived usefulness
of
counseling are the type of counseling provided, how it is recommended, and
the setting of the counseling. In settings where many clients are declining
counseling, these barriers and others should be examined. The counseling might be
providing information only rather than addressing personal risks. Counselors might not
be offering counseling in ways appropriate to the client's culture, language, sex,
sexual orientation, age, or developmental level. The setting might inhibit open discussion
of risk (e.g., some outreach settings are not private). Counseling skills (e.g.,
attentive listening, use of open-ended questions) that allow clients to participate might
have been overlooked. Even when clients at increased risk refuse counseling, use of
1--2 open-ended questions that urge clients to examine their personal situations
could prompt personal exploration of risk (e.g, "What were your concerns that led you
to decide to get tested today?").
Consider Alternative Methods for HIV Prevention Counseling
HIV prevention counseling models proven effective have all used
face-to-face (individual or group) encounters between counselor and client and involved
>2 brief sessions. Thus, face-to-face prevention counseling is preferred for clients at
increased HIV risk. Most HIV test sites use an enzyme immunoassay (EIA) and confirmatory
test algorithm that requires several days for final results. The return visit for test
result offers an opportunity to continue prevention counseling in a second,
face-to-face meeting. However, in some settings (e.g., STD clinics, managed care
organizations, and other private settings), many clients do not return for their results
(50,114--116). In such settings, providers can adopt strategies that increase clients' receipt of
test results, and counseling strategies might need to be adapted
(117).
Telephone Counseling. Limited studies among STD clinic clients at lower
risk indicated that substantially more clients learned their HIV infection status
when negative test results were provided by telephone rather than in person
(12,117,118). Although home sample collection provides a precedent for providing counseling
by telephone to persons with either negative or positive HIV test results, the efficacy
of telephone counseling in reducing HIV risk behaviors or the number of new
HIV infections has not been studied. One study indicated that telephone notification
of positive results was associated with delay in linkage to care
(119). However, not learning positive test results at all guarantees a delay in linkage to care.
Many specialists recommend that provision of HIV test results and prevention counseling
by telephone be limited to clients whose results are negative (Technical Expert
Panel Review of CDC HIV Counseling, Testing, and Referral Guidelines; February
18--19, 1999; Atlanta, Georgia). Also, given the known risk-reduction benefits of
face-to-face counseling, lack of efficacy data on telephone counseling, and concerns
regarding disinhibition (e.g., "since my test result is negative, whatever risks I am taking
now may be okay"), telephone counseling should be limited to clients without
known ongoing HIV risk behaviors (e.g., unprotected sex or needle-sharing with an
HIV-infected [or status unknown] partner).
Single-Session Prevention Counseling with Rapid
Testing. Rapid tests allow clients to receive their HIV test results the same day. This process could reduce the number
of clients receiving two prevention counseling sessions. Studies of the efficacy of
single HIV prevention counseling sessions for use with a rapid test are under way.
Although some single-session counseling protocols have been successfully implemented in
busy
clinics and are well-accepted by most clients, how well a single counseling
session reduces risk behaviors or the number of new HIV infections is unknown. A
counseling protocol for use with a rapid test is being studied; information is available at
<http://www.cdc.gov/hiv/projects/respect-2>. For clients with identified risk behaviors,
referral or rescheduling for ongoing counseling should be considered.
Ensuring High-Quality HIV Prevention Counseling
All CTR providers should conduct routine, periodic assessments for
quality assurance to ensure that the counseling being provided includes the
recommended, essential counseling elements.
Supervisors must be aware of HIV prevention counseling goals and
necessary counselor skills. Supervisor and administrator support of HIV counseling models
that focus on personal risk reduction (distinct from provision of information) is critical
to effective counseling. Quality assurance for counseling should contain the
following elements:
Training and continuing
education. Basic training in the use of
>1 of the interactive HIV prevention counseling models aimed at personal risk reduction
is recommended for counselors and supervisors. Counselors should know
the communities they serve and the available referral opportunities. They also
might benefit from formal training on a) transmission and prevention of HIV and
other sexually transmitted and bloodborne diseases, b) the natural history of HIV,
c) recognition and treatment of opportunistic infections, d) new therapeutic
agents used to treat HIV and AIDS, e) PCRS, f) prevention case management, and
g) other HIV prevention and support services available in the community
(e.g., services related to substance abuse assessment, cultural
competence, adolescent concerns, domestic abuse, and health concerns for gay or
lesbian clients). Additional training in specific counseling skills is also warranted
(e.g., training on how to facilitate groups for counselors conducting group
sessions). For training opportunities, providers or supervisors can contact their state
health department's HIV/AIDS program office.
Supervisor observation and immediate feedback to
counselors. Direct observation of counseling sessions can help ensure that objectives are being
met (80). Supervisors can perform this task periodically (with client
consent). Sessions might also be audiotaped (with client consent), or counseling can
be demonstrated through role-play scenarios between the counselor
and supervisor. Observation and feedback should be structured, and the
outcome should be constructive, not punitive. Supervisors should support
positive elements of the prevention counseling session and provide specific,
constructive comments regarding content areas needing improvement. Observation
and feedback should be conducted regularly for routine counseling. Staff
discomfort with observation typically wanes over time; many counselors report that
the sessions are useful in enhancing skills. When observation is offered
routinely, clients seldom refuse to participate. A suggested time frame for routine,
direct observation of an HIV prevention counselor by the supervisor is twice
monthly for the first 6 months, monthly for the second 6 months, and quarterly
for counselors with >1 year of experience. After observation, supervisors
should provide feedback to counselors quickly, preferably the same week.
Observation and feedback forms used in research studies of client-centered HIV
prevention counseling are available at
<http://www.cdc.gov/hiv/projects/RESPECT/default.htm>.
Periodic evaluation of physical space, client flow, and time
concerns. Counseling sessions should be conducted in a private space where discussion cannot
be overheard. Clients should not wait for long periods between testing
and counseling, and information could be provided during waiting times (e.g.,
through videos). Periodic time-flow analyses or client surveys can be used to
evaluate adequacy of space, client flow, and length of waiting period.
Periodic counselor or client satisfaction
evaluations. Evaluations of client satisfaction can ensure that counseling meets client needs. These
evaluations also can provide important feedback to counselors who otherwise might not
see the benefits of what they do. Evaluations can be brief. Surveys should
address whether specific counseling goals were met, the type of interaction
(e.g.,"who talked more, the counselor or the client?"), and, when applicable, specifics
of development of the risk-reduction plan (e.g, "what was the behavior change
step that you agreed to work on?"). Linking client and counselor descriptions of
a particular session might be useful. Conducting such evaluations only
occasionally (e.g., for 1--2 weeks once or twice a year) decreases the programmatic
burden and is probably sufficient to identify problems. For more information, see
Quality Assurance and Evaluation of HIV CTR Services.
Case conferences. Regularly scheduled meetings of counselors
allow supervisors to understand counselors' skills and areas that need
improvement and can help counselors learn techniques from their colleagues.
Case conferences are an opportunity for counselors to discuss specific or
problematic questions asked by clients, allowing providers to better understand the
concerns facing clients who are HIV-infected or at increased risk for HIV. Case
conferences can help offset counselor fatigue and "burn out" by providing a positive
outlet for dealing with difficult situations. Discussion might focus on a
hard-to-address client or specific elements (e.g., developing acceptable and practical
risk-reduction plans with clients who deny the magnitude of their HIV risk).
Frequency of case conferences should be balanced with client volume, with efforts made
to meet at least monthly.
HIV TESTING
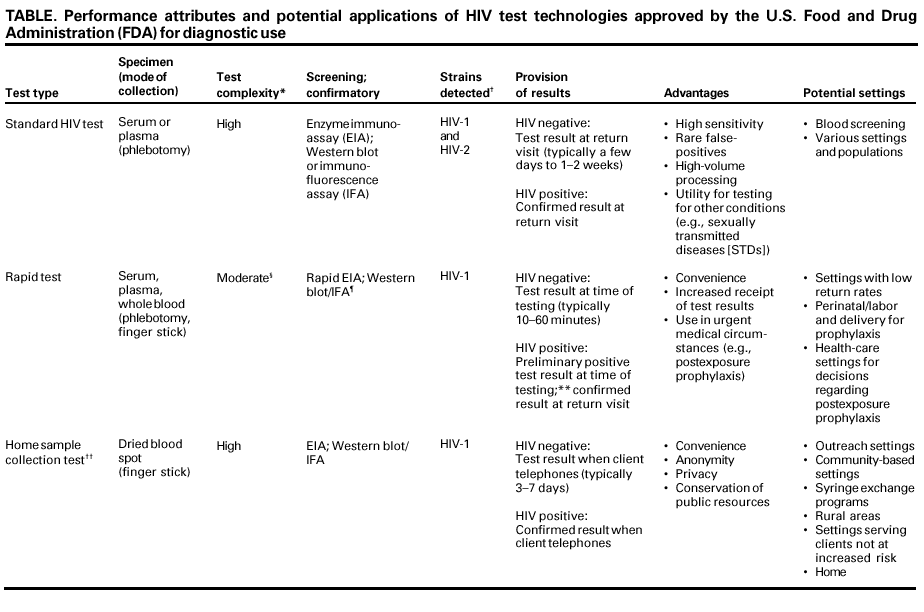
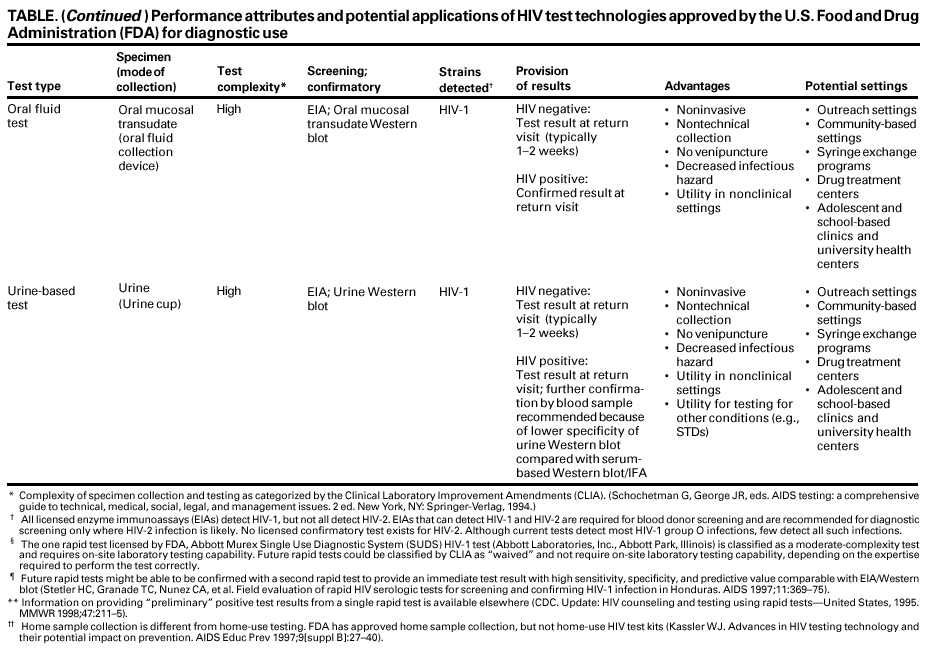
Characteristics and Applications of HIV Test Technologies
Only FDA-approved HIV tests should be used for diagnostic purposes.
Routine screening in the United States for HIV-2 and HIV-1 group O infections is not
generally recommended unless geographic, behavioral, or clinical information indicates
that infection with these strains might be present. Several HIV test technologies have
been
approved by FDA for diagnostic use in the United States. These tests enable testing
of different fluids (i.e., whole blood, serum, plasma, oral fluid, and urine) (Table).
The available technologies
enable specimen collection procedures that are less invasive and
more acceptable than venipuncture, thus helping expand HIV testing
into nontraditional settings (with home sample collection tests, oral fluid tests,
and urine-based tests) (25);
enable provision of HIV test results during a single visit at the time of
testing (with rapid tests) (120); and
increase the convenience of HIV testing (with home sample collection tests)
(52).
The decision to adopt a particular test technology in a clinical or
nontraditional setting should be based on several factors, including
accuracy of the test,
client preferences and acceptability,
likelihood of client returning for results,
cost and mechanism for provider reimbursement,
ease of sample collection,
complexity of laboratory services required for the test,
availability of trained personnel, and
FDA approval of the test.
Home Testing Versus Home Sample Collection
FDA has not approved home-use HIV test kits, which allow consumers to
purchase a test kit, collect a sample in private, and interpret their own HIV test results in a
few minutes. The Federal Trade Commission has warned that some home-use HIV test
kits, many of which are available on the Internet and in the "gray" market
(i.e., unauthorized imports), supply inaccurate results
(121). These tests are different from FDA-approved home sample collection kits
(52), which allow consumers to purchase test kits, collect a sample in private, send the sample to a laboratory for testing,
and telephone for their HIV test result, counseling, and referral.
HIV-2 and HIV-1 Group O Infections
Although most HIV infections in the United States are of HIV-1 group B
subtype, current EIAs can accurately identify infections with nearly all non-B subtypes
and many infections with group O HIV subtypes
(122). Infections with HIV-2 and HIV-1 group O are rare in the United States
(123,124), and routine screening for these subtypes is not generally recommended as part of diagnostic testing except in
areas where several such infections have been identified. Routine screening for HIV-2
might be appropriate in certain populations where potential risk for HIV-2 infection is
higher (e.g., in areas where West African immigrants have settled)
(125). Since June 1992, FDA has recommended routine screening for antibody to HIV-2 (in addition to
HIV-1)
for all blood and plasma donations (125). Clients with clinical, epidemiologic,
or laboratory history that suggests HIV infection and negative or indeterminate
HIV-1 screening tests should receive further diagnostic testing to rule out HIV
infection, potentially including testing for HIV-1 non-B subtypes
(122) and HIV-2 (125).
Other Test Uses
Viral load and HIV-1 p24 antigen assays are not intended for routine diagnosis
but could be used in clinical management of HIV-infected persons in conjunction
with clinical signs and symptoms and other laboratory markers of disease
progression. Although HIV-1 p24 antigen assays are used for routine screening in blood and
plasma centers, routine use for diagnosing HIV infection has been discouraged because
the estimated average time from detection of p24 antigen to detection of HIV antibody
by standard EIA is 6 days, and not all recently infected persons have detectable levels
of p24 antigen (126).
Interpreting HIV Test Results
Standard Testing Algorithm
HIV-1 testing consists of initial screening with an EIA to detect antibodies to
HIV-1. Specimens with a nonreactive result from the initial EIA are considered
HIV-negative unless new exposure to an infected partner or partner of unknown HIV status
has occurred. Specimens with a reactive EIA result are retested in duplicate. If the result
of either duplicate test is reactive, the specimen is reported as repeatedly reactive
and undergoes confirmatory testing with a more specific supplemental test (e.g.,
Western blot or, less commonly, an immunofluorescence assay [IFA]). Only specimens that
are repeatedly reactive by EIA and positive by IFA or reactive by Western blot
are considered HIV-positive and indicative of HIV infection. Specimens that are
repeatedly EIA-reactive occasionally provide an indeterminate Western blot result, which
might represent either an incomplete antibody response to HIV in specimens from
infected persons or nonspecific reactions in specimens from uninfected persons
(127). Although IFA can be used to resolve an indeterminate Western blot sample, this
assay is not widely used. Generally, a second specimen should be collected
>1 month later and retested for persons with indeterminate Western blot results. Although much
less commonly available, nucleic acid testing (e.g., viral RNA or proviral DNA
amplification method) could also help resolve an initial indeterminate Western blot in
certain situations. A small number of tested specimens might provide inconclusive
results because of insufficient quantity of specimen for the screening or confirmatory tests.
In these situations, a second specimen should be collected and tested for HIV infection.
Modified Testing Algorithms
FDA has licensed only one rapid test, but modified testing algorithms
are anticipated when additional rapid HIV tests are approved. If
>2 sensitive and specific rapid HIV tests became available, one positive rapid test could be confirmed with
a different rapid test. This combination has provided positive predictive value
compared with the EIA/Western blot or IFA algorithm
(128). However, no such algorithms have been adequately assessed or approved for diagnostic use in the United States.
Positive HIV Test Results
An HIV test should be considered positive only after screening and
confirmatory tests are reactive. A confirmed positive test result indicates that a person has
been infected with HIV. False-positive results when both screening and confirmatory
tests are reactive are rare. However, the possibility of a mislabeled sample or
laboratory error must be considered, especially for a client with no identifiable risk for
HIV infection. HIV-vaccine--induced antibodies may be detected by current tests and
may cause a false-positive result. Persons whose test results are HIV-positive and who
are identified as vaccine trial participants should be encouraged to contact or return
to their trial site or an associated trial site for HIV CTR services.
Negative HIV Test Results
Because a negative test result likely indicates absence of HIV infection (i.e.,
high negative predictive value), a negative test need not be repeated in clients with no
new exposure in settings with low HIV prevalence. For clients with a recent history
of known or possible exposure to HIV who are tested before they could
develop detectable antibodies (129,130), the possibility of HIV infection cannot be
excluded without follow-up testing (29). A false negative result also should be considered
in persons with a negative HIV-1 test who have clinical symptoms suggesting
HIV-1 infection or AIDS. Additional testing for HIV-2 and HIV-1 group O infection might
be appropriate for these persons.
Indeterminate HIV Test Results
Most persons with an initial indeterminate Western blot result who are
infected with HIV-1 will develop detectable HIV antibody within 1 month
(127,131,132). Thus, clients with an initial indeterminate Western blot result should be retested for
HIV-1 infection >1 month later.****** Persons with continued indeterminate Western blot
results after 1 month are unlikely to be HIV-infected and should be counseled as though
they are not infected unless recent HIV exposure is suspected.
Nucleic acid tests for HIV DNA or RNA exist, but are not approved by FDA
for diagnostic purposes and are not generally recommended for resolving
indeterminate Western blot results. However, in consultation with clinical and laboratory
specialists, nucleic acid testing (if available) might also be useful for determining infection
status among persons with an initial indeterminate Western blot result.
Informing Clients of Test Results
Because low rates of return for test results occur in many settings offering HIV
CTR (133), providers should work to ensure that clients tested for HIV infection receive
their test results, particularly HIV-infected clients who might benefit from earlier entry
into care and initiation of antiretroviral therapy. Reducing barriers to testing can
maximize the number and proportion of persons tested for HIV who receive their test results in
a timely manner (see Addressing Barriers to HIV Testing). Adoption of new HIV
test technologies and alternative methods of providing HIV-negative test results should
be considered when face-to-face rates of return for test results are low.
Strict confidentiality of the receipt of the HIV test and the HIV test result must be
maintained,
regardless of the method used. Providers unable to locate clients who do not return
for test results should seek support from their local or state health department.
Because knowledge of HIV status is a critical HIV prevention strategy and
essential for entry into care, providers should stress to clients the importance of returning
to receive their test results and establish a plan for doing so with the client.
Reminder systems might be useful. Using alternate HIV test technologies might increase
the percentage of tested persons who learn their HIV status.
Providing Test Results by Telephone
Many clinicians routinely notify clients of negative test results for various
diseases and conditions by means other than face-to-face (e.g., by telephone). They also
ask clients to return to discuss positive test results that might indicate potential
life-threatening illnesses. This strategy can also be applied, under limited
circumstances, to notifying clients of their HIV test results. Face-to-face provision of HIV test results
is strongly encouraged for HIV-infected clients and HIV-uninfected clients at
increased risk who might benefit from HIV prevention counseling and referral to
medical, preventive, and support services. Providing uninfected clients who are not
at increased risk the option of receiving HIV test results and counseling by telephone
--- with the understanding that provider assurance of client confidentiality is
of paramount importance --- might be appropriate. Limited research indicates
that offering clients the option of contacting the provider by telephone to receive
negative HIV results might increase rates of receipt of results, satisfy client preferences
for options, and preserve setting resources without apparent adverse
consequences (52,117,118). Although no published research exists regarding use of telephones
for providing positive HIV test results with most HIV test technologies, limited
experience exists on using this method to provide HIV-positive test results for home
sample collection testing (52).
Providing Test Results During the Initial Visit Through Rapid Tests
More clients receive their HIV test results with rapid tests because results can
be provided at the testing visit (120). Rapid test technology could be useful in
urgent medical circumstances (e.g., when decisions must be made regarding
postexposure prophylaxis) and in nontraditional settings with low return rates (e.g.,
community-based or outreach settings).
During the initial visit, the provider can definitively tell clients who have had
a single rapid HIV test with negative results that they are not infected
(120), except when retesting might be indicated because of recent known or possible exposure
to HIV. A reactive rapid HIV test result should be considered preliminary until
the completion of confirmatory testing, and results should be carefully communicated
to the client because of the possibility of a false-positive result.
The likelihood that a positive screening test truly indicates the presence of
HIV infection decreases as HIV prevalence in the tested population becomes
lower. Therefore, false-positive HIV test results are more likely in settings where the
tested
population prevalence is lower than in settings where the tested
population prevalence is higher. When a preliminary, positive rapid test is explained to
clients, phrases like "a good chance of being infected" or "very likely infected" can be used
to indicate the likelihood of HIV infection and qualified based on the HIV prevalence in
the setting and the client's individual risk
(120). Further testing is always required
to confirm a reactive screening test result.
Follow-up Testing in Clients with Negative HIV Test Results
A negative HIV test usually indicates the absence of HIV infection
(29). Because recent infection cannot be excluded without follow-up testing (see Negative HIV
Test Results), the appropriate timing and frequency for follow-up testing among clients
with negative HIV test results has not been firmly established. Providers should
consider the following factors related to individual client needs when recommending the
timing and frequency for follow-up HIV testing:
Timing of the last potential exposure.
Probability of HIV infection given type of exposure.
Presence or likelihood of ongoing risk behavior.
Likelihood of returning for follow-up HIV testing, prevention counseling,
and referral.
Client anxiety.
Provider and client relationship.
Resource constraints.
Recent Exposure
Follow-up testing might be appropriate for clients who have negative test
results but who have not had time to develop detectable antibody after a recent
documented occupational (54) or nonoccupational (sexual or needle-sharing)
(55) exposure to HIV-infected persons or persons at increased risk for HIV with unknown HIV status.
The timing of follow-up testing should provide assurance that the exposure did not lead
to infection. Follow-up testing should be conducted in a timely manner so
clients identified as HIV-infected can receive appropriate antiretroviral treatment
and prevention and support services as soon as possible.
Single Possible or Known Exposure
Most infected persons will develop detectable HIV antibody within 3 months
of exposure (126). If the initial negative HIV test was conducted within the first 3
months after exposure, repeat testing should be considered
>3 months after the exposure occurred to account for the possibility of a false-negative result. If the follow-up test
is nonreactive, the client is likely not HIV-infected. However, if the client was exposed to
a known HIV-infected person or if provider or client concern remains, a second
repeat test might be considered >6 months from the exposure. Rare cases of
seroconversion 6--12 months after known exposure have been reported
(134). Extended follow-up testing beyond 6 months after exposure to account for possible
delayed
seroconversion is not generally recommended and should be based on
clinical judgment and individual clients needs
(54).
Ongoing Exposure
Persons with continued HIV risk behavior pose a special challenge for
follow-up testing. In some settings, clients with ongoing risk represent a substantial proportion
of those receiving HIV CTR. In most circumstances, follow-up HIV testing should
be recommended periodically for clients with ongoing risk behavior. Follow-up
testing would monitor the client's HIV status, but also promote continued client
contact, opportunities for HIV prevention counseling (see Additional Counseling
Considerations for Special Situations), and referral to additional preventive and support services.
No Identifiable Risk
In general, persons with no recent identifiable risk for HIV infection should
receive additional HIV prevention counseling and follow-up testing when requested.
Efforts should be made to understand why these clients repeatedly seek follow-up
testing. These clients should be considered for in-depth prevention counseling and referral
to support services, where appropriate.
Special Considerations
General recommendations for follow-up testing might not be applicable in
all circumstances. In certain circumstances (e.g., when persons are
simultaneously exposed to hepatitis C virus and HIV
[54] and when persons have received HIV vaccines), guidance should be provided only after consultation with specialists.
Addressing Barriers to HIV Testing
Knowledge of HIV infection status can benefit the health of individual persons
and the community. Thus, HIV testing should be as convenient as possible to promote
client knowledge of HIV infection status. Efforts should be made to remove or lower
barriers to HIV testing by ensuring that
testing is accessible, available, and responsive to client and community
needs and priorities;
anonymous and confidential HIV testing are available;
the testing process considers the client's culture, language, sex,
sexual orientation, age, and developmental level; and
confidentiality is maintained (see Principles of HIV Counseling, Testing,
and Referral).
Acceptance of HIV testing is reportedly lower when clients have been
tested previously and are fearful of their ability to cope with their test results
(112,113). Testing is more likely to be accepted when
clients perceive their own HIV risk and acknowledge behaviors placing them
at increased risk (135);
testing is voluntary and routinely offered to clients rather than clients having
to request it (113,136);
protections for client confidentiality are in place
(113,137);
anonymous testing is available
(113,138);
alternate HIV test technologies are offered to clients
(26);
providers recommend testing as part of appropriate medical care
(139,140); and
providers (141) and clients
(113) perceive HIV counseling and testing to
be beneficial for early diagnosis and prevention purposes.
Ensuring High-Quality Testing
Testing activities should be coordinated with state and local laboratories to
ensure high-quality HIV testing through proper specimen collection, storage, and
transport. Laboratory errors most often occur in the preanalytic (i.e., specimen
collection, labeling, transporting, processing, and storing) and postanalytic steps of testing
(i.e., results validation and reporting)
(142--144) rather than during the test
itself. Laboratories performing HIV testing must be enrolled in proficiency testing
programs and conduct activities in accordance with regulatory standards outlined by the
Clinical Laboratory Improvement Amendments (CLIA) of 1988
(145). Many states have additional licensing requirements for laboratories conducting diagnostic HIV testing.
HIV REFERRAL
Definition of Referral
In the context of HIV prevention counseling and testing, referral is the process
by which immediate client needs for care and supportive services are assessed
and prioritized and clients are provided with assistance (e.g., setting up
appointments, providing transportation) in accessing services. Referral should also include
follow-up efforts necessary to facilitate initial contact with care and support service providers.
In this context, referral does not include ongoing support or management of
the referral or case management. Case management is generally characterized by
an ongoing relationship with a client that includes comprehensive assessment of
medical and psychosocial support needs, development of a formal plan to address
needs, substantial assistance in accessing referral services, and monitoring of
service delivery.
Typical Referral Needs
Clients should be referred to services that are responsive to their priority
needs and appropriate to their culture, language, sex, sexual orientation, age,
and developmental level. Examples of these services include
Prevention case
management. Clients with multiple and complex needs
that affect their ability to adopt and sustain behaviors to reduce their risk
for transmitting or acquiring HIV should receive or be referred for prevention
case management services, including ongoing prevention counseling
(28). Prevention case management can help coordinate diverse referral and follow-up concerns.
Medical evaluation, care, and
treatment. HIV-infected clients should receive
or be referred to medical services that address their HIV infection
(including evaluation of immune system function and screening, treatment, and
prevention of opportunistic infections)
(23,29--32,53). Screening and prophylaxis
for opportunistic infections and related HIV-conditions (e.g., cervical cancer)
are important for HIV-infected persons. In addition, coinfection with HIV
and communicable diseases (e.g., TB, STDs, and hepatitis) can, if untreated, pose
a risk to susceptible community members. Thus, providers of HIV testing should
be familiar with appropriate screening tests (e.g., TB), vaccines (e.g., hepatitis A
and B), STD and prophylactic TB treatment, and clinical evaluation for active
TB disease to ensure that these communicable diseases are identified early
and appropriate clinical referrals are made, even if clients forego outpatient
HIV treatment.
Partner counseling and referral
services. Persons with HIV-positive test
results should receive or be referred to services to help them notify their sex
or injection-drug-equipment--sharing partners or spouses regarding their
exposure to HIV and how to access CTR. Guidelines for PCRS are available
(27).
Reproductive health
services. Female clients who are pregnant or
of childbearing age should receive or be referred to reproductive health
services. HIV-infected pregnant women should be referred to providers who can
provide prevention counseling and education, initiate medical therapy to
prevent perinatal transmission, and provide appropriate care based on
established treatment guidelines (see Revised Recommendations for HIV Screening
of Pregnant Women).
Drug or alcohol prevention and
treatment. Clients who abuse drugs or alcohol should receive or be referred to substance or alcohol abuse prevention
and treatment services.
Mental health services. Clients who have mental illness,
developmental disability, or difficulty coping with HIV diagnosis or HIV-related conditions
should receive or be referred to appropriate mental health services.
Legal services. Clients who test positive should be referred to legal services
as soon as possible after learning their test result for counseling on how to
prevent discrimination in employment, housing, and public accommodation by
only disclosing their status to those who have a legal need to know.
STD screening and care. Clients who are HIV-infected or at increased risk for
HIV are at risk for other STDs and should receive or be referred for STD
screening and treatment (146).
Screening and treatment for viral
hepatitis. Many clients who are HIV-infected or at increased risk for HIV are at increased risk for acquiring viral hepatitis (A,
B, and C). Men who have sex with men and IDUs should be vaccinated for
hepatitis A. All clients without a history of hepatitis B infection or vaccination should
be tested for hepatitis B, and if not infected, should receive or be referred
for hepatitis B vaccination. In addition, clients who inject drugs should be
routinely recommended testing for hepatitis C. All clients who are infected with
hepatitis viruses should be referred for appropriate treatment. Further guidance
is available (30,32).
Other services. Clients might have multiple needs that can be addressed
through other HIV prevention and support services (e.g., assistance with housing,
food, employment, transportation, child care, domestic violence, and legal
services). Addressing these needs can help clients access and accept medical services
and adopt and maintain behaviors to reduce risk for HIV transmission and
acquisition. Clients should receive referrals as appropriate for identified needs.
Implement and Manage Referral Services
Clients should receive help accessing and completing referrals, and completion
of referrals should be verified. In the context of HIV prevention counseling and
testing, the following elements should be considered essential to the development
and delivery of referral services (99).
Assess Client Referral Needs
Providers should consult with the client to identify essential factors that a) are
likely to influence the client's ability to adopt or sustain behaviors to reduce risk for
HIV transmission or acquisition or b) promote health and prevent disease
progression. Assessment should include examination of the client's willingness and ability to
accept and complete a referral. Service referrals that match the client's self-identified
priority needs are more likely to be successfully completed than those that do not
(147). Priority should be placed on ensuring that HIV-infected clients are assessed for
referral needs related to medical care, PCRS, and prevention and support services aimed
at reducing the risk for further transmission of HIV. When a provider cannot
make appropriate referrals or when client needs are complex, clients should be referred to
a case management system.
Plan the Referral
Referral services should be responsive to clients' needs and priorities
and appropriate to their culture, language, sex, sexual orientation, age, and
developmental level. In consultation with clients, providers should assess and address any factors
that make completing the referral difficult (e.g., lack of transportation or child care,
work schedule, cost). Research has indicated that referrals are more likely to be
completed if services are easily accessible to clients
(147).
Help Clients Access Referral Services
Clients should receive information necessary to successfully access the
referral service (e.g., contact name, eligibility requirements, location, hours of
operation, telephone number). Research has indicated that providing assistance (e.g., setting
an appointment, addressing transportation needs) for some clients promotes
completion of referrals (148). Clients must give consent before identifying information to
help complete the referral can be shared. Outreach workers and peer
counselors/educators can be an important and effective resource to help clients identify needs and
plan successful referrals (149). Referrals are more likely to be completed after
multiple contacts with outreach workers
(147).
Document Referral and Follow-Up
Providers should assess and document whether the client accessed the
referral services. If the client did not, the provider should determine why; if the client did,
the provider should determine the client's degree of satisfaction. If the services
were unsatisfactory, the provider should offer additional or different
referrals. Documentation of referrals made, the status of those referrals, and client
satisfaction with referrals should help providers better meet the needs of clients.
Information obtained through follow-up of referrals can identify barriers to completing the
referral, responsiveness of referral services in addressing client needs, and gaps in the
referral system.
Ensure High-Quality Referral Services
Providers of referral services should know and understand the service needs
of their clients, be aware of available community resources, and be able to
provide services in a manner appropriate to the clients' culture, language, sex,
sexual orientation, age, and developmental level, given local service system limitations.
Education and Support of Staff Members
Staff members providing referral services must understand client needs,
have skills and resources to address these needs, have authority to help the client
procure services, and be able to advocate for clients.
Training and Education. Providers should ensure that staff members
receive adequate training and continuing education to implement and manage
referrals. Training and education should address resources available and methods for
managing referrals, as well as promote understanding of factors likely to influence the
client's ability and willingness to use a referral service (e.g., readiness to accept the
service, competing priorities, financial resources). Referrals are more likely to be
completed when a provider is able to correctly evaluate a client's readiness to adopt
risk-reducing behaviors (147). Research has indicated that cross-training increases knowledge
and understanding of community resources among providers and can indicate gaps
in services (148).
Authority. Staff members providing referrals must have the authority necessary
to accomplish a referral. Supervisors must ensure that staff members
understand referral policy and protocol and have the necessary support to provide referrals.
This requires the authority of one provider to refer to another (e.g., through memoranda
of
agreement) or to obtain client consent for release of medical or other
personal information.
Advocacy. Staff members who negotiate referrals must possess knowledge
and skills to advocate for clients. Such advocacy can help clients obtain services
by mediating barriers to access to services and promoting an environment in
which providers are better informed regarding the needs and priorities of their clients.
Provider Coordination and Collaboration
Providers should develop and maintain strong working relationships with
other providers and agencies that might be able to provide needed services. Providers
who offer HIV prevention counseling and testing but not a full range of medical
and psychosocial support services should develop direct, clearly delineated
arrangements with other providers who can offer needed services. Coordination and
collaboration promotes a shared understanding of the specific medical and psychosocial needs
of clients requiring services, current resources available to address these needs,
and gaps in resources.
Memoranda of agreement or other forms of formal agreement are useful
in outlining provider/agency relationships and delineating roles and responsibilities
of collaborating providers in managing referrals. When confidential client information
is shared between coordinating providers, such formal agreements are essential.
These agreements should be reviewed periodically and modified as appropriate.
Referral Resources
Knowledge of available support services is essential for successful referrals.
When referral resources are not available locally, providers should identify
appropriate resources and link clients with them. A resource guide should be developed
and maintained to help staff members make appropriate referrals (Box 7).
Information regarding community resources can be obtained from local health planning
councils, consortia, and community planning groups. Local, state, and national
HIV/AIDS information hotlines or websites (e.g., NPIN), community-based health and
human service providers, and state and local public health departments can also
provide information.
HIV CTR SERVICES IN NONTRADITIONAL SETTINGS
CTR should be provided in community-based and outreach settings as well
as clinical settings. Data from publicly supported CTR programs have indicated that
doing so could promote use of these services by persons at increased risk for HIV. When
HIV CTR are not readily available, accessible, or acceptable, persons at increased
risk might not take advantage of them. Expanding CTR into nontraditional settings can
be accomplished through partnership with community-based service providers and use
of new, FDA-approved HIV test technologies that offer portability, less-invasive
sample collection, less-complex sample collection and processing, and reduced biohazard.
To ensure effective CTR that is responsive to client needs, providers should develop
and implement written quality assurance protocols and procedures specifically for
services provided in nontraditional settings.
Privacy and Confidentiality
Ensuring clients' privacy and confidentiality during CTR is essential, but
could present unique challenges in some nontraditional settings. Confidentiality can
more easily be breached in settings where clients and providers can be seen or heard
by others. Suggested strategies for maintaining privacy and confidentiality
in nontraditional settings include the following:
Use a separated area in a mobile van.
Use rooms with locking doors.
Mark a specific room with a "do not disturb" or "occupied" sign.
Designate an area in the setting that provides physical privacy.
In parks and similar locations, seek areas with as much privacy as possible.
Provide counseling and testing services in the client's home or other
secure setting.
Have clients return to the setting to receive test results and counseling
and referral.
Informed Consent
Staff members providing CTR services should be sensitive to barriers that
can interfere with obtaining true informed consent, including alcohol and drug use,
mental illness, and peer pressure in venues where persons congregate or
socialize. Suggested strategies for obtaining informed consent in nontraditional settings
include the following:
Schedule an appointment to test at a later date/time.
Follow up at a later time with the client if contact information is available.
Read the informed consent form to the client.
Use verbal prompts to ensure that the client understands information in
the informed consent form.
Counseling
Staff members working in community-based and other nontraditional
settings should know and use risk-screening strategies to determine whether HIV
prevention counseling should be recommended. Staff members should be trained in
HIV prevention counseling or other approaches aimed at personal HIV risk
reduction. When appropriate (e.g., among IDUs), information regarding other STDs
and bloodborne diseases should be incorporated into the counseling sessions
(29,30).
Testing
The decision to offer HIV testing in nontraditional settings should be based
on several factors, including availability of resources and feasibility of providing
test
results and follow-up. In some cases, referral to other providers is appropriate.
The selection of a specific HIV test technology should be based on logistical issues
(e.g., field conditions related to collection, transport, and storage of specimens;
worker safety; and the likelihood that clients will receive HIV test results). Providers
must understand the extent to which field conditions can affect specimens (e.g.,
extreme temperatures or time lapse from collection to processing). Test specimens should
be collected, stored, and transported according to manufacturer instructions.
Provision of Test Results
Clear protocols for provision of test results and prevention counseling should
be developed. The following strategies might be useful in ensuring the provision of
results in nontraditional settings:
Provide a telephone number that clients can call to receive test results.
Make an appointment with the client at the time of testing to receive results.
Provide incentives (e.g., food certificates, hygiene kits, food).
Return to a site on a regularly scheduled basis.
Provide reminders when contact information is available.
Referral
Staff members working in community-based and outreach settings should
be trained to implement and manage referrals. Providers should establish
appropriate collaborative relationships for referrals. Arranging for PCRS staff members or
case managers to be available to clients at the time test results are provided might
help promote referral.
Record Keeping
Maintaining the confidentiality of client records is critical. Providers should
develop written protocols for record keeping that address transport of client records to
and from outreach venues. Strategies to maintain confidentiality of client records
in nontraditional settings include the following:
Return all client records to the office immediately after the CTR session.
Use codes or unique identifiers rather than client names.
Store all records in a secured area (e.g., locked file drawers).
Provide option of anonymous counseling and testing as well as
confidential counseling and testing.
Verify identity of client (e.g., match client signature with that provided
for informed consent or check identification card) when providing test results.
Store paperwork in a lockbox while in outreach settings.
Password protect and encrypt electronically stored client records.
Where allowed by state/local statute, clients can choose anonymous HIV
testing. Procedures to ensure client anonymity (i.e., no indication of testing in the
client's record and no recording of personal identifying information on laboratory
requests) should be developed. Even when staff members providing CTR services know
the client (including name and locating information) from other activities, the client's
right to be tested anonymously should be protected.
Staff Safety
Providing services in outreach settings (e.g., bars, parks) might compromise
staff safety, which must be considered in development of outreach protocols.
Appropriate training and precautions (e.g., working in teams) should be developed in
planning services in nontraditional settings.
QUALITY ASSURANCE AND EVALUATION OF HIV CTR SERVICES
Quality Assurance
Written quality assurance protocols should be developed, made available to
all staff members providing CTR services, and routinely implemented. All staff
members should receive training and orientation regarding quality assurance. For
information specific to ensuring high-quality CTR services, see Ensuring High-Quality
HIV Prevention Counseling, Ensuring High-Quality Testing, and Ensuring
High-Quality Referral Services. Quality assurance activities should address the following:
Accessibility of services (e.g., hours of operation, location, availability of
supplies and materials such as brochures, posters, test kits, safe injection
materials, condoms, or lubricant).
Compliance with written protocols for provision of service to an individual
client (e.g., appropriate counseling protocols, timely return of HIV test results,
referral for services responsive to client's priority needs).
Services and materials appropriate to the client's culture, language, sex,
sexual orientation, age, and developmental level.
Staff performance/proficiency (e.g., competence, skills, credentials, and training).
Supervision of staff members, including routine, timely feedback.
Compliance with program guidelines and performance standards.
Appropriateness of services to client needs, measured with client
satisfaction tools (e.g., surveys or suggestion boxes).
Record-keeping procedures, including confidentiality and security.
Community resources (availability and collaborative arrangements).
Collection, handling, and storage of specimens.
Assurance of adequate funding and institutional support for CTR services.
Evaluation
CTR services should be continually evaluated to improve services to clients
and provide accountability to stakeholders
(150,151). Evaluation should be
interactive, involving individual persons and organizations affected by the services
(150). In public health settings, the community goals outlined in community health planning
processes and other relevant local planning processes could be incorporated.
Providers should identify the key, relevant program goals and objectives
that reflect services to the program, community, and client, and then determine what
data are needed to evaluate those goals and objectives. Information obtained from
the evaluation should be used to plan and prioritize provision of CTR services within
a setting. For example, information from the HIV Counseling and Testing System
(133) or locally available sources could be used during local community planning (e.g.,
HIV prevention community planning) to help develop or revise an HIV/AIDS
prevention plan or describe who needs services. If resources for evaluation are
limited, comprehensive evaluations (e.g., examining outcome or impact) might not be
possible. However, even with limited resources, providers can conduct meaningful
evaluations by focusing on relevant local outcomes
(82).
Data
Data collected should have a clear, anticipated use and should not be the focus
of or interfere with provision of CTR services. Data should be used to evaluate the
extent to which the goals of CTR and locally defined service outcomes (e.g., targeted
return rates, knowledge of HIV infection status, proportion of successful referrals) are
met. Although sound data are essential for evaluation of services, the primary purpose
of each visit should be to provide the best possible service to the client. Data should
be recorded outside the time reserved for CTR discussions between the provider and
the client. Clients could complete a questionnaire or intake information form on
admission, providers could complete the forms immediately after meeting with a client, or
a combination of the two approaches could be used.
Data collection methods should be compatible with the evaluation needs
and priorities of the CTR setting and locally defined service outcomes. Data should
be collected with a standard collection instrument throughout the program. Simple
data collection instruments (e.g., intake forms, medical record reviews) should
be developed so data can be collected unobtrusively as part of the provision of services.
Publicly funded CTR sites collect data on client demographic characteristics,
risk behavior/exposure category, test acceptance, and type of site where service
is provided (133). Most sites record the date of visit, anonymous or confidential
test status, previous test result, current test result, and return for current test result
for each client encounter. Additional data can be useful for evaluation of
services, including date of previous test, type of current test (e.g., standard, rapid, oral
fluid), risk-reduction plan summary, information relevant to any referrals made
(e.g., provider and service description, information and materials provided, whether
an appointment was made), whether the referral was received, type of service
provided,
dates when services were provided, and other relevant information (e.g.,
follow-up required, additional service needs).
Confidentiality
Any data collected or recorded must be collected or recorded in a manner
that ensures the confidentiality of the client. Clear procedures and protocol manuals
must be developed and used.
Ensuring High-Quality Evaluation
The system used to collect the information must be monitored periodically
to ensure data quality, which depends on the cooperative efforts of all
persons providing CTR services. Periodically, data collection systems should
check records at each level of the data-collection process to ensure that information
is recorded consistently and completely.
Adequate training in the use of data collection instruments should be provided
to all staff members to ensure that the evaluation process is not interfering with
the provision of high-quality CTR services.
The information assembled during the evaluation process should be
analyzed and reported in a timely manner to individual persons and organizations
affected by the service.
Information and feedback gained during the evaluation process should be
used to improve the services offered by the site to the client.
CONCLUSION
Advances in HIV prevention and medical treatment increase the importance of
HIV CTR services. Prevention counseling and knowledge of HIV status can help
persons who are HIV-infected or at increased risk for HIV infection reduce their risk
for transmitting or acquiring HIV infection. Referral can help persons access
relevant medical, preventive, and psychosocial support services to reduce their risk
for transmitting or acquiring HIV infection. These guidelines recommend how CTR can
be provided to clients who could most benefit from these services across various
settings and client populations.
ADDITIONAL RESOURCES
Additional information on HIV CTR can be obtained from the following sources:
We are grateful for the contributions of health professionals within CDC and
elsewhere (e.g., Health Resources and Services Administration, National Alliance of State
and Territorial AIDS Directors, academic institutions, health departments,
health-care organizations). We also thank graduate students/research assistants Jennifer
Chapman, M.P.H., Steven J. Connor, M.P.H., and Parag R. Sanghvi, M.S.P.H., National Center for
HIV, STD, and TB Prevention, CDC.
CDC. HIV counseling, testing and referral standards and guidelines. Atlanta, GA:
US Department of Health and Human Services, Public Health Service, CDC, 1994.
Kamb ML, Fishbein M, Douglas JM Jr, et al. Efficacy of risk-reduction counseling
to prevent human immunodeficiency virus and sexually transmitted diseases:
a randomized controlled trial. JAMA 1998;280:1161--7.
The National Institutes of Mental Health (NIMH) Multisite HIV Prevention Trial
Group. The NIMH multisite HIV prevention trial: reducing HIV sexual risk behavior.
Science 1998;280:1889--94.
Boyer CB, Barrett DC, Peterman TA, Bolan G. Sexually transmitted disease (STD)
and HIV risk in heterosexual adults attending a public STD clinic: evaluation of
a randomized controlled behavioral risk-reduction intervention trial. AIDS
1997;11:359--67.
St. Lawrence JS, Brasfield TL, Jefferson KW, Alleyne E, O'Bannon RE, III, Shirley
A. Cognitive-behavioral intervention to reduce African American adolescents' risk for
HIV infection. J Consult Clin Psychol 1995;63:221--37.
McCusker J, Willis G, McDonald M, Sereti SM, Lewis BF, Sullivan JL.
Community-wide HIV counselling and testing in central Massachusetts: who is retested and does
their behavior change? J Community Health 1996;21:11--22.
Kelly JA, Murphy DA, Washington CD, et al. The effects of HIV/AIDS
intervention groups for high-risk women in urban clinics. Am J Pub Health 1994;84:1918--22.
Tudiver F, Myers T, Kurtz RG, et al. The talking sex project: results of a
randomized controlled trial of small-group AIDS education for 612 gay and bisexual
men. Evaluation and the Health Professions 1992;15:26--42.
Wenger NS, Linn LS, Epstein M, Shapiro MF. Reduction of high-risk sexual
behavior among heterosexuals undergoing HIV antibody testing: a randomized clinical trial.
Am J Pub Health 1991;81:1580--5.
Orr DP, Langefeld CD, Katz BP, Caine VA. Behavioral intervention to increase
condom use among high-risk female adolescents. J Pediatr 1996;128:288--95.
Hobfoll SE, Jackson AP, Lavin J, Britton PJ, Shepherd JB. Reducing inner-city
women's AIDS risk activities: a study of single, pregnant women. Health Psychol
1994;13:397--403.
Kelly JA, St. Lawrence JS, Hood HV, Brasfield TL. Behavioral intervention to
reduce AIDS risk activities. J Consult Clin Psychol 1989;57:60--7.
Valdiserri RO, Lyter DW, Leviton LC, Callahan CM, Kingsley LA, Rinaldo CR.
AIDS prevention in homosexual and bisexual men: results of a randomized trial
evaluating two risk reduction interventions. AIDS 1989;3:21--6.
Jemmott JB, III, Jemmott LS, Fong GT. Reductions in HIV risk-associated
sexual behaviors among black male adolescents: effects of an AIDS prevention
intervention. Am J Pub Health 1992;82:372--7.
Shain RN, Piper JM, Newton ER, et al. A randomized, controlled trial of a
behavioral intervention to prevent sexually transmitted disease among minority women. N Eng
J Med 1999;340:93--100.
O'Donnell C, O'Donnell L, San Doval A, Duran R, Labes K. Reductions in STD
infections subsequent to an STD clinic visit: using video-based patient education to
supplement provider interactions. Sex Transm Dis 1998;25:161--7.
Cohen DA, MacKinnon DP, Dent C, Mason HRC, Sullivan E. Group counseling at
STD clinics to promote use of condoms. Public Health Rep 1992;107:727--31.
Cohen D, Dent C, MacKinnon D. Condom skills education and sexually
transmitted disease reinfection. J Sex Research 1991;28:139--44.
Palella FJ Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality
among patients with advanced human immunodeficiency virus infection. N Eng J
Med 1998;338:853--60.
Connor EM, Sperling RS, Gelber R, et al. Reduction of maternal-infant transmission
of human immunodeficiency virus type 1 with zidovudine treatment. N Eng J
Med 1994;331:1173--80.
Kassler WJ. Advances in HIV testing technology and their potential impact
on prevention. AIDS Educ Prev 1997;9(suppl B):27--40.
Spielberg B, Goldbaum G, Branson B, Wood B. Acceptance of alternate HIV
counseling and testing strategies [Abstract]. Presented in the 1999 National HIV
Prevention Conference, Atlanta, GA, 1999.
CDC. HIV partner counseling and referral services: guidance. Atlanta, GA:
US Department of Health and Human Services, Public Health Service, CDC, 1998.
CDC. HIV prevention case management: guidance. Atlanta, GA: US Department
of Health and Human Services, CDC, 1997.
Collis TK, Celum CL. The clinical manifestations and treatment of sexually
transmitted diseases in human immunodeficiency virus-positive men. Clin Infect Dis
2001;32:611--22.
Valdiserri RO, Holtgrave DR, West GR. Promoting early HIV diagnosis and entry
into care. AIDS 1999;13:2317--30.
Rietmeijer CA, Kane MS, Simons PZ, et al. Increasing the use of bleach and
condoms among injecting drug users in Denver: outcomes of a targeted, community-level
HIV prevention program. AIDS 1996;10:291--8.
Rhodes F, Malotte CK. HIV risk interventions for active drug users. In:
S.Oskamp, S.Thompson, eds. Understanding HIV risk behavior: safer sex and drug
use. Thousand Oaks, CA: Sage Publications, 1996:297--36.
Gibson DR, Lovelle-Drache J, Young M, Hudes ES, Sorensen JL. Effectiveness of
brief counseling in reducing HIV risk behavior in injecting drug users: final results
of randomized trials of counseling with and without HIV testing. AIDS and
Behavior 1999;3:3--12.
Doll LS, O'Malley PM, Pershing AL, Darrow WW, Hessol NA, Lifson AR.
High-risk sexual behavior and knowledge of HIV antibody status in the San Francisco City
Clinic Cohort. Health Psychol 1990;9:253--65.
Cleary PD, Van Devanter N, Rogers TF, et al. Behavior changes after notification of
HIV infection. Am J Pub Health 1991;81:1586--90.
Fox R, Odaka NJ, Brookmeyer R, Polk BF. Effect of HIV antibody disclosure
on subsequent sexual activity in homosexual men. AIDS 1987;1:241--6.
van Griensven GJP, de Vroome EMM, Tielman RAP, et al. Effect of
human immunodeficiency virus (HIV) antibody knowledge on high-risk sexual behavior
with steady and nonsteady sexual partners among homosexual men. Am J
Epidemiol 1989;129:596--603.
Coates TJ, Morin SF, McKusick L. Behavioral consequences of AIDS antibody
testing among gay men [Letter]. JAMA 1987;258:1889.
Wenger NS, Kusseling FS, Beck K, Shapiro MF. Sexual behavior of individuals
infected with the human immunodeficiency virus: the need for intervention. Arch Intern
Med 1994;154:1849--54.
Desenclos J-C, Papaevangelou G, Ancelle-Park R, for the European Community
Study Group on HIV in Injecting Drug Users. Knowledge of HIV serostatus and
preventive behaviour among European injecting drug users. AIDS 1993;7:1371--7.
Dawson J, Fitzpatrick R, McLean J, Hart G, Boulton M. The HIV test and
sexual behavior in a sample of homosexually active men. Soc Sci Med 1991;32:683--8.
Otten MW Jr, Zaidi AA, Wroten JE, Witte J, Peterman TA. Changes in
sexually transmitted disease rates after HIV testing and posttest counseling, Miami, 1988
to 1989. Am J Pub Health 1993;83:529--33.
Quinn TC, Wawer MJ, Sewankambo N, et al. Viral load and heterosexual
transmission of human immunodeficiency virus type 1. N Eng J Med 2000;342:921--9.
Branson BM. Home sample collection tests for HIV infection. JAMA
1998;280:1699--701.
Tiara DA, Safran DG, Seto TB, Rogers WH, Tarlov AR. The relationship between
patient income and physician discussion of health risk behaviors. JAMA 1997;278:1412--7.
Schwartz JS, Lewis CE, Clancy C, Kinosian MS, Radany MH, Koplan JP.
Internists' practices in health promotion and disease prevention. Ann Intern Med 1991;114:46--53.
Bindman AB, Osmond D, Hecht FM, et al. Multistate Evaluation of anonymous
HIV testing and access to medical care. JAMA 1998;280:1416--20.
Chen Z, Branson B, Ballenger A, Peterman TA. Risk assessment to improve targeting
of HIV counseling and testing services of STD clinic patients. Sex Transm Dis
1998;25:539--43.
Quinn TC, Glasser D, Cannon RO, et al. Human immunodeficiency virus
infection among patients attending clinics for sexually transmitted diseases. N Eng J
Med 1988;318: 197--203.
Erickson B, Wasserheit JN, Rompalo AM, Brathwaite W, Glasser D, Hook EW
III. Routine voluntary HIV screening in STD clinic clients: characterization of
infected clients. Sex Transm Dis 1990;17:194--9.
Groseclose S, Erickson B, Quinn T, Glasser D, Campbell C, Hook E. Characteristics
of patients accepting and refusing routine, voluntary HIV antibody testing in
public sexually transmitted disease clinics. Sex Transm Dis 1994;21:31--5.
Kassler WJ, Zenilman JM, Erickson B, Fox R, Peterman TA, Hook EW
III. Seroconversion in patients attending sexually transmitted disease clinics.
AIDS 1994;8:351--5.
Asch SM, London AS, Barnes PF, Gelberg L. Testing for human
immunodeficiency virus infection among tuberculosis patients in Los Angeles. Am J Respir Crit Care
Med 1997;155:378--81.
Pitchenik AE, Burr J, Suarez M, Fertel D, Gonzalez G, Moas C. Human
T-cell lymphotropic virus-III (HTLV-III) seropositivity and related disease among
71 consecutive patients in whom tuberculosis was diagnosed. Am Rev Respir
Dis 1987;135:875--9.
Shafer RW, Chirgwin KD, Glatt AE, Dahdouh MA, Landesman SH, Suster B.
HIV prevalence, immunosuppression, and drug resistance in patients with tuberculosis
in an area endemic for AIDS. AIDS 1991;5:399--405.
Theuer CP, Hopewell PC, Elias D, Schecter GF, Rutherford GW, Chaisson RE.
Human immunodeficiency virus infection in tuberculosis patients. J Infect Dis 1990;162:8--12.
Peterman TA, Todd KA, Mupanduki I. Opportunities for targeting publicly
funded human immunodeficiency virus counseling and testing. J Acquir Immune Defic
Syndr 1996;12:69--74.
Janssen RS, St. Louis ME, Satten GA, et al. HIV infection among patients in U.S.
acute care hospitals: strategies for the counseling and testing of hospital patients. New
Eng J Med 1992;327:445--52.
CDC. HIV prevalence trends in selected populations in the United States: results
from national serosurveillance, 1993--1997. Atlanta, GA: US Department of Health
and Human Services, CDC, 2001.
Kelly JA, St. Lawrence JS. The prevention of AIDS: roles for behavioral
intervention. Scand J Behav Therapy 1987;16:5--19.
Cohen DA, Dent C, MacKinnon D, Hahn G. Condoms for men, not women: results
of brief promotion programs. Sex Transm Dis 1992;19:245--51.
Sikkema KJ, Bissett RT. Concepts, goals, and techniques of counseling: review
and implications for HIV counseling and testing. AIDS Educ Prev 1997;9(suppl B):14--26.
Roffman RA, Kalichman SC, Kelly JA, et al. HIV antibody testing of gay men in
smaller US cities. AIDS Care 1995;7:405--13.
DiClemente RJ, Wingood GM. A randomized controlled trial of an HIV sexual
risk-reduction intervention for young African-American women. JAMA 1995;274:1271--6.
Kelly JA, St. Lawrence JS, Diaz YE, et al. HIV risk behavior reduction
following intervention with key opinion leaders of population: an experimental analysis. Am
J Pub Health 1991;81:168--71.
Kelly JA, St. Lawrence JS. Behavioral intervention and AIDS. The Behavioral
Therapist 1986;6:121--5.
Kamb ML, Dillon BA, Fishbein M, Willis KL, and the Project RESPECT Study
Group. Quality assurance of HIV prevention counseling in a multi-center
randomized controlled trial. Public Health Rep 1996;111(suppl 1):99--107.
Holtgrave DR, Valdiserri RO, Gerber AR, Hinman AR. Human immunodeficiency
virus counseling, testing, referral, and partner notification services: a cost-benefit
analysis. Arch Intern Med 1993;153:1225--30.
Holtgrave DR, Reiser WJ, DiFranceisco W. The evaluation of HIV
counseling-and-testing services: making the most of limited resources. AIDS Educ Prev
1997;9(3 suppl):105--18.
Kamb ML, Kassler W, Peterman TA, and the Project RESPECT Study Group. Cost
of preventing HIV via counseling: results from a randomized trial (Project
RESPECT) [Abstract 33263]. Presented at the XII International Conference on AIDS,
Geneva, Switzerland, 1998:644.
Booth RE, Kwiatkowski CF, Stephens RC. Effectiveness of HIV/AIDS interventions
on drug use and needle risk behaviors for out-of-treatment injection drug users.
J Psychoactive Drugs 1998;30:269--78.
Castrucci BC, Kamb ML, Hunt K. Assessing use of the 1994 HIV counseling,
testing, and referral standards and guidelines---how closely does practice conform to
existing recommendations? [Abstract P125]. Presented at the 2000 National STD
Prevention Conference, December 4--7, Milwaukee, WI, 2000.
Kelly JA, Murphy DA, Sikkema KJ, Kalichman SC. Psychological interventions
to prevent HIV infection are urgently needed: new priorities for behavioral research in
the second decade of AIDS. Am Psychol 1993;48:1023--34.
McCusker J, Stoddard AM, Zapka JG, Zorn M, Mayer KH. Predictors of
AIDS-preventive behavior among homosexually active men: a longitudinal study. AIDS 1989;3:443--8.
Kelly JA, Murphy DA. Some lessons learned about risk reduction after ten years of
the HIV/AIDS epidemic. AIDS Care 1991;3:251--7.
Kelly JA, Murphy DA. Psychological interventions with AIDS and HIV: prevention
and treatment. J Consult Clin Psychol 1992;60:576--85.
American Public Health Association. AIDS prevention in the community: lessons
from the first decade. Washington, DC: American Public Health Association, 1995.
Wiktor SZ, Biggar RJ, Melbye M, et al. Effect of knowledge of
human immunodeficiency virus infection status on sexual activity among homosexual men.
J Acquir Immune Defic Syndr 1990;3:62--8.
Kelly JA, St. Lawrence JS, Betts R, Brasfield TL, Hood HV. A skills-training
group intervention model to assist persons in reducing risk behaviors for HIV infection.
AIDS Educ Prev 1990;2:24--35.
Sikkema KJ, Winett RA, Lombard DN. Development and evaluation of an
HIV-risk reduction program for female college students. AIDS Educ Prev 1995;7:145--59.
Kelly JA, Kalichman SC. Increased attention to human sexuality can improve
HIV-AIDS prevention efforts: key research issues and directions. J Consult Clin Psychol
1995;63:907--18.
CDC. Compendium of HIV prevention interventions with evidence of
effectiveness. Atlanta, GA: US Department of Health and Human Services, CDC, 1999.
Higgins DL, Galavotti C, O'Reilly KR, et al. Evidence for the effects of HIV
antibody counseling and testing on risk behaviors. JAMA 1991;266:2419--29.
Wolitski RJ, MacGowan RJ, Higgins DL, Jorgenson CM. The effects of HIV
counseling and testing on risk-related practices and help-seeking behavior. AIDS Educ
Prev 1997;9(suppl B):52--67.
Flaskerud JH. Matching client and therapist ethnicity, language, and gender: a
review of research. Issues in Mental Health Nursing 1990;11:321--36.
Kilmarx PH, Hamers FF, Peterman TA. Living with HIV: experiences and perspectives
of HIV-infected sexually transmitted disease clinic patients after posttest counseling.
Sex Transm Dis 1998;25:28--37.
Cates W, Handsfield HH. HIV counseling and testing: does it work? Am J Public
Health 1988;78:1533--4.
Calsyn DA, Saxon AJ, Freeman G, Whittaker S. Ineffectiveness of AIDS education
and HIV antibody testing in reducing high risk behaviors among injection drug users.
Am J Public Health 1992;82:573--5.
Edlin BR, Irwin KL, Faruque S, et al. Intersecting epidemics---crack cocaine use and
HIV infection among inner-city young adults. N Eng J Med 1994;331:1422--7.
Cottler LB, Leukefeld C, Hoffman J, et al. Effectiveness of HIV risk reduction
initiatives among out-of-treatment non-injection drug users. J Psychoactive Drugs
1998;30:279--90.
Nicolosi A, Molinari S, Musicco M, Saracco A, Ziliani N, Lazzarin A.
Positive modification of injecting behavior among intravenous heroin users from Milan
and Northern Italy 1987--1989. Brit J Addiction 1991;86:91--102.
Neaigus A, Sufian M, Friedman S, et al. Effects of outreach intervention on
risk reduction among intravenous drug users. AIDS Educ Prev 1990;2:253--71.
Obermeyer TE, Streeter A. Street outreach HIV education to intravenous drug
users and other substance abusers. AIDS Patient Care 1991;5:312--4.
Hagan H, Jarlais DC, Friedman SR, Purchase D, Alter MJ. Reduced risk of hepatitis
B and hepatitis C among injection drug users in the Tacoma Syringe Exchange
Program. Am J Public Health 1995;85:1531--7.
Jones TS, Vlahov D. Use of sterile syringes and aseptic drug preparation are
important components of HIV prevention among injection drug users. J Acquir Immune
Defic Syndr 1998;18(suppl 1):S1--S5.
Padian NS, O'Brien TR, Chang Y, Glass S, Francis DP. Prevention of
heterosexual transmission of human immunodeficiency virus through couple counseling. J
Acquir Immune Defic Syndr 1993;6:1043--8.
Kamenga M, Ryder RW, Jingu M, et al. Evidence of marked sexual behavior
change associated with low HIV-1 seroconversion in 149 married couples with discordant
HIV-1 serostatus: experience at an HIV counselling center in Zaire. AIDS 1991;5:61--7.
De Vincenzi I. A longitudinal study of human immunodeficiency virus transmission
by heterosexual partners. N Eng J Med 1994;331:341--6.
Levy J, Fox S, Valle M. What you don't know can hurt you: the influence of prior
HIV testing on serostatus results at repeat testing [Abstract 43113]. Presented at the
12th World AIDS Conference, Geneva, Switzerland, 1998:869.
Irwin KL, Valdiserri RO, Holmberg SD. The acceptability of voluntary HIV
antibody testing in the United States: a decade of lessons learned. AIDS 1996;10:1707--17.
Valdiserri RO, Moore M, Gerber AR, Campbell CH Jr, Dillon BA, West GR. A study
of clients returning for counseling after HIV testing: implications for improving rates
of return. Public Health Rep 1993;108:12--8.
Catania JA, Gibson DR, Marin B, Coates TJ, Greenblatt RM. Response bias
in assessing sexual behaviors relevant to HIV transmission. Evaluation and
Program Planning 1990;13:19--29.
Weber JT, Frey R Jr, Horsley R, Gwinn ML. Publicly funded HIV counseling and
testing in the United States, 1992--1995. AIDS Educ Prev 1997;9(suppl B):79--91.
Branson B, Ballenger A, Olthoff G. HIV test results and post-test counseling
by telephone [Abstract PC0535]. Presented at the Tenth International Conference
on AIDS, 1994.
Schluter WW, Judson FN, Baron AE, McGill WL, Marine WM, Douglas JM
Jr. Usefulness of human immunodeficiency virus post-test counseling by telephone
for low-risk clients of an urban sexually transmitted diseases clinic. Sex Transm
Dis 1996;23:190--7.
Samet JH, Freedberg KA, Stein MD, et al. Trillion virion delay: time from
testing positive for HIV to prevention for primary care. Arch Intern Med 1998;158:734--40.
Sullivan PS, Do AN, Robbins K, et al. Surveillance for variant strains of HIV: subtype
G and group O HIV-1 [Letter]. JAMA 1997;278:292.
CDC. Human immunodeficiency virus type 2. Atlanta, GA: US Department of
Health and Human Services, CDC, 1998. Available at
<http://www.cdc.gov/hiv/pubs/facts/hiv2.htm>. Accessed July 4, 2001.
Celum CL, Coombs RW, Lafferty W, et al. Indeterminate human
immunodeficiency virus type 1 Western blots: seroconversion risk, specificity of supplemental tests,
and an algorithm for evaluation. J Infect Dis 1991;164:656--64.
Stetler HC, Granade TC, Nunez CA, et al. Field evaluation of rapid HIV serologic
tests for screening and confirming HIV-1 infection in Honduras. AIDS 1997;11:369--75.
Horsburgh CR Jr, Jason J, Longini I, et al. Duration of human immunodeficiency
virus infection before detection of antibody. Lancet 1989;2:637--40.
Busch MP, Lee LLJ, Satten GA, et al. Time course of detection viral and
serologic markers preceding human immunodeficiency virus type 1
seroconversion: implications for screening of blood and tissue donors. Transfusion 1995;35:91--7.
Jackson JB, MacDonald KL, Cadwell J, et al. Absence of HIV infection in blood
donors with indeterminate Western blot tests for antibody to HIV-1. N Eng J Med
1990;322:217--22.
Dock NL, Kleinman SH, Rayfield MA, Schable CA, Williams AE, Dodd RY.
Human immunodeficiency virus infection and indeterminate Western blot
patterns: prospective studies in a low prevalence population. Arch Intern Med 1991;151:525--30.
CDC. HIV counseling and testing in publicly funded sites: annual report, 1997
and 1998. Atlanta, GA: US Department of Health and Human Services, CDC, 2001.
Ciesielski CA, Metler RP. Duration of time between exposure and seroconversion
in healthcare workers with occupationally acquired infection with
human immunodeficiency virus. Am J Med 1997;102:115--6.
Wykoff RF, Jones JL, Longshore ST, et al. Notification of the sex and
needle-sharing partners of individuals with human immunodeficiency virus in rural South Carolina:
30 month experience. Sex Transm Dis 1991;18:217--22.
Exner TM, Ehrhardt A, Loeb I, Zawadzki R. HIV counseling and testing:
women's experiences and the role of testing as a prevention strategy [Abstract We.C.3529].
In: Proceedings of the XI International Conference on AIDS, 1996;11(2):150.
Kassler WJ, Meriwether RA, Klimko TB, Peterman TA, Zaidi A. Eliminating access
to anonymous HIV antibody testing in North Carolina: effects on HIV testing and
partner notification. J Acquir Immune Defic Syndr 1997;14:281--9.
Simpson WM, Johnstone FD, Goldberg DJ, Gormley SM, Hart GJ. Antenatal
HIV testing: assessment of a routine voluntary approach. BMJ 1999;318:1660--1.
Lee JH, Mitchell B, Nolt B, Robbins B, Thomas MC, Branson BM. Targeted opt-in
vs. routine opt-out HIV testing in an STD clinic [Abstract 153]. Presented at the
1999 National HIV Prevention Conference, August 29--September 1, Atlanta, GA, 1999.
Rahimian A, Driscoll M, Taylor D, Cohen M. Barriers to building a
comprehensive system of HIV counseling and testing by consent to women of reproductive age
in Chicago, Illinois [Abstract Tu.D. 2772]. In: Proceedings of the XI
International Conference on AIDS, 1996;1:396.
Nutting PA, Main DS, Fischer PM, et al. Problems in laboratory testing in primary
care. JAMA 1996;275:635--9.
Boone DJ, Steindel SD, Herron R, et al. Transfusion medicine monitoring practices:
a study of the College of American Pathologists/CDC Outcomes Working Group.
Arch Path Lab Med 1995;119:999--1006.
Witte DL, VanNess SA, Angstandt DS, Pennell BJ. Errors, mistakes, blunders,
outliers, or unacceptable results: how many. Clin Chem 1997;43:1352--6.
Schochetman G, George JR, eds. AIDS testing: a comprehensive guide to
technical, medical, social, legal, and management issues. 2 ed. New York, NY:
Springer-Verlag, 1994.
Institute of Medicine. Eng TR, Butler WT, eds. The hidden epidemic:
confronting sexually transmitted diseases. Washington, DC: National Academy Press, 1997.
Greenberg JB, MacGowan R, Neumann M, et al. Linking injection drug users
to medical services: role of street outreach referrals. Health Soc Work 1998;23:298--309.
Marx R, Hirozawa AM, Chu PL, Bolan GA, Katz M. Linking clients for HIV
antibody counseling and testing to prevention services. J Community Health 1999;24:201--14.
Hymel MS, Greenberg BL. The Walden House Young Adult HIV Project: meeting
the needs of multidiagnosed youth. J Adolesc Health 1998;23S:122--31.
CDC. Evaluating CDC-funded health department HIV prevention programs. Volume
1: guidance. Atlanta, GA: US Department of Health and Human Services, CDC, 1999.
* Delivered according to recommended protocols (for counseling, referral, and
evaluation) or regulatory standards (for testing).
** Risk screening differs from risk assessment, which is a part of HIV prevention
counseling (see HIV Prevention Counseling).
*** For example, "A negative test means no HIV was found. But if you were exposed to
HIV recently --- in the last 1--2 months --- this test may not be able to pick that up."
See Negative HIV Test Results.
**** Client-centered is used here to mean that the counseling sessions focus on the
client's own risk circumstances, risk behaviors, and prevention needs. This term should not
be confused with the more intensive, client-centered approach advocated by
psychologist Carl R. Rogers, although some skills and strategies that involve the client in
the prevention counseling process might be similar (Rogers CR. Client-centered therapy:
its current practice, implications, and theory. Boston, MA: Houghton Mifflin, 1951).
***** Personal risk assessment is an essential element of HIV prevention counseling in
which the client and counselor work to understand and acknowledge the client's personal
risk for HIV. Risk assessment is not synonymous with risk screening (see
Determining Individual Client Risk Through Risk Screening and Box 2), which helps determine
which clients should be recommended HIV CTR.
Acquired immunodeficiency syndrome. AIDS can affect the immune and
central nervous systems and can result in neurological problems, infections, or cancers.
It is caused by human immunodeficiency virus (HIV).
Anal sex:
A type of sexual intercourse in which a man inserts his penis in his
partner's anus. Anal sex can be insertive or receptive.
Anonymous:
In anonymous testing, client identifying information is not linked to
testing information, including the request for tests or test results.
Antiretroviral therapy:
Treatment with drugs designed to prevent HIV from
replicating in HIV-infected persons. Highly active antiretroviral therapy (HAART) is
an antiretroviral regimen that includes multiple classifications of antiretroviral drugs.
Client-centered HIV prevention
counseling:
An interactive risk-reduction
counseling model usually conducted with HIV testing, in which the counselor helps the
client identify and acknowledge personal HIV risk behaviors and commit to a
single, achievable behavior change step that could reduce the client's HIV risk.
Confidentiality:
Pertains to the disclosure of personal information in a relationship
of trust and with the expectation that it will not be divulged to others in ways that
are inconsistent with the original disclosure. Confidentiality must be maintained
for persons who are recommended and/or who receive HIV counseling, testing,
and referral (CTR) services.
Confidential HIV test:
An HIV test for which a record of the test and the test results
are recorded in the client's chart.
Confirmatory test:
A highly specific test designed to confirm the results of an
earlier (screening) test. For HIV testing, a Western blot or, less commonly,
an immunofluorescence assay (IFA) is used as a confirmatory test.
EIA:
Enzyme immunoassay. Sometimes referred to as ELISA (see next definition).
A commonly used screening test to detect antibodies to HIV.
ELISA:
Enzyme-linked immunosorbent assay. A type of EIA (see previous definition).
A commonly used screening test to detect antibodies to HIV.
Evaluation:
A process for determining how well health systems, either public
or private, deliver or improve services and for demonstrating the results of
resource investments.
False negative:
A negative test result for a person who is actually infected.
False positive:
A positive test result for a person who is actually not infected.
Freestanding HIV test site:
A site that provides only HIV services. Sometimes
referred to as alternate test site or anonymous test site.
HIV:
Human immunodeficiency virus, which causes AIDS. Several types of HIV
exist, with HIV-1 being the most common in the United States.
HIV test:
More correctly referred to as an HIV antibody test, the HIV test is
a laboratory procedure that detects antibodies to HIV, rather than the virus itself.
HIV prevention counseling:
An interactive process between client and
counselor aimed at reducing risky sex and needle-sharing behaviors related to
HIV acquisition (for HIV-uninfected clients) or transmission (for HIV-infected
clients). See also client-centered HIV prevention counseling.
Home sample collection test:
A test that a consumer purchases and uses to
collect blood (or other bodily fluid) and then send it out for testing. Counseling and
test results are typically provided by telephone using user-generated codes to
ensure confidentiality and anonymity.
Incidence:
In epidemiology, the number of new cases of infection or disease that
occur in a defined population within a specified time.
Indeterminate test result:
A possible result of a Western blot, which might represent
a recent HIV infection or a false-positive.
Information:
In the context of HIV counseling, information encompasses the topics
HIV transmission and prevention and the meaning of HIV test results.
Informed consent:
The legally effective permission of a client or legally
authorized representative (e.g., parent or legal guardian of a minor child) to undergo
a medical test or procedure.
Negative predictive value:
A negative predictive value estimates the probability that
a person with a negative diagnostic test result will actually not be infected.
Nonoccupational HIV exposure:
A reported sexual, injection-drug--use, or other
non-occupational HIV exposure that might put a patient at high risk for acquiring
HIV infection.
Nucleic acid amplification testing:
A type of testing that identifies viral genes
(e.g., specific sequences of nucleic acids) using gene amplification technologies such
as polymerase chain reaction (PCR).
Occupational HIV exposure:
An occupational exposure to HIV that occurs during
the performance of job duties. Defined as a percutaneous injury (e.g., a needlestick
or cut with a sharp object), contact of mucous membranes, or contact of
skin (especially when the exposed skin is chapped, abraded, or afflicted with
dermatitis or the contact is prolonged or involving an extensive area) with blood, tissues,
or other body fluids to which universal precautions apply.
Oral fluid test:
A test using oral mucosal transudate, a serous fluid. To differentiate
this fluid from saliva, an absorbent material is left in the mouth for several minutes.
In an HIV-infected person, oral mucosal transudate is likely to contain HIV antibodies.
Oral sex:
A type of sexual intercourse in which the partner's genitals are stimulated
by mouth and tongue.
Partner counseling and referral services
(PCRS):
A prevention activity that aims to a) provide services to HIV-infected persons and their sex and
needle-sharing partners so they can reduce their risk for infection or, if already infected,
can prevent transmission to others and b) help partners gain earlier access
to individualized counseling, HIV testing, medical evaluation, treatment, and
other prevention and support services.
Perinatal HIV transmission:
Transmission of HIV from the mother to the fetus or
infant during pregnancy, delivery, or breast-feeding.
Positive predictive value:
A positive predictive value estimates the probability that
a person with a positive diagnostic test result will actually be infected.
Positive test:
For HIV, a specimen sample that is reactive on an initial ELISA
test, repeatedly reactive on a second ELISA run on the same specimen, and
confirmed positive on Western blot or other supplemental test indicates that the client
is infected.
Prevalence:
The number or percentage of persons in a given population with a
disease or condition at a given point in time.
Prevention case management (PCM):
A client-centered HIV prevention activity
that promotes adoption of HIV risk-reduction behaviors by clients with
multiple, complex problems and risk-reduction needs. PCM is a hybrid of HIV
prevention counseling and traditional case management that provides intensive,
on-going, individualized prevention counseling, support, and referral to other
needed services.
Prevention counseling:
An interactive process between client and counselor aimed
at reducing risky sex and needle-sharing behaviors related to HIV acquisition
(for HIV-uninfected clients) or transmission (for HIV-infected clients). See also
client-centered HIV prevention counseling and HIV prevention counseling.
Quality assurance:
An ongoing process for ensuring that the CTR program
effectively delivers a consistently high level of service to the clients.
Rapid HIV test:
A test to detect antibodies to HIV that can be collected and
processed within a short interval of time (e.g., approximately 10--60 minutes).
Referral:
The process through which a client is connected with services to
address prevention needs (medical, prevention, and psychosocial support).
Risk assessment:
Risk assessment is a fundamental part of a client-centered
HIV prevention counseling session in which the client is encouraged to
identify, acknowledge, and discuss in detail his or her personal risk for acquiring
or transmitting HIV.
Risk screening:
A brief evaluation of HIV risk factors, both behavioral and clinical,
used for decisions about who should be recommended HIV counseling and testing.
Risk screening is different from risk assessment.
Screening test:
An initial test, usually designed to be sensitive, to identify all
persons with a given condition or infection (e.g., enzyme immunoassay [EIA] or
enzyme-linked immunosorbent assay [ELISA]).
Sensitivity:
The probability that a test will be positive when infection or condition
is present.
Seroconversion:
Initial development of detectable antibodies specific to a
particular antigen; the change of a serologic test result from negative to positive as a
result of antibodies induced by the introduction of antigens or microorganisms into
the host.
Specificity:
The probability that a test will be negative when the infection or condition
is not present.
Tuberculosis (TB) disease:
Active disease caused by
Mycobacterium tuberculosis, as evidenced by a confirmatory culture, or, in the absence of culture,
suggestive clinical symptoms, including productive cough lasting
>3 weeks, chest pain, hemoptysis, fever, night sweats, weight loss, and easy fatigability. Active TB is
a communicable disease that is treatable, curable, and preventable, and
persons with active TB disease should be under the care of a health-care provider.
Active TB disease could indicate immune deficiency. For HIV-infected persons, active
TB disease is considered an opportunistic infection and a qualifying condition
for AIDS.
Tuberculosis (TB) infection:
Infection with the bacteria
M. tuberculosis, as evidenced by a positive tuberculin skin test (TST) that screens for infection with this
organism. Sometimes, TST is called a purified protein derivative (PPD) or Mantoux test.
A positive skin test might or might not indicate active TB disease (see
tuberculosis disease). Thus, any person with a positive TST should be screened for active
TB and, once active TB is excluded, evaluated for treatment to prevent
the development of TB disease. TB infection alone is not considered an
opportunistic infection indicating possible immune deficiency.
Vaginal sex:
A type of sexual intercourse in which the man's penis enters the
woman's vagina.
Voluntary HIV testing:
HIV testing that is offered free of coercion. With voluntary
HIV testing, participants have the opportunity to accept or refuse HIV testing.
Western blot:
A laboratory test that detects specific antibodies to components of
a virus. Chiefly used to confirm HIV antibodies in specimens found
repeatedly reactive using ELISA.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].