|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
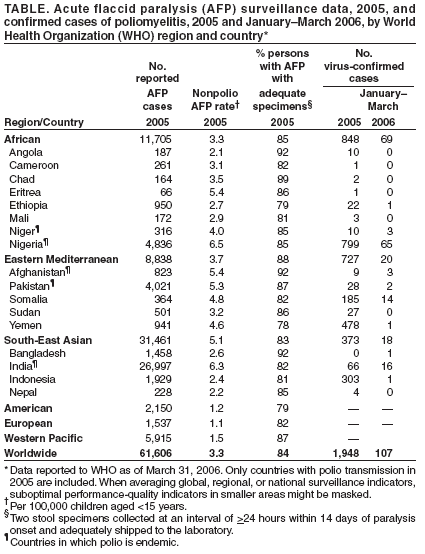
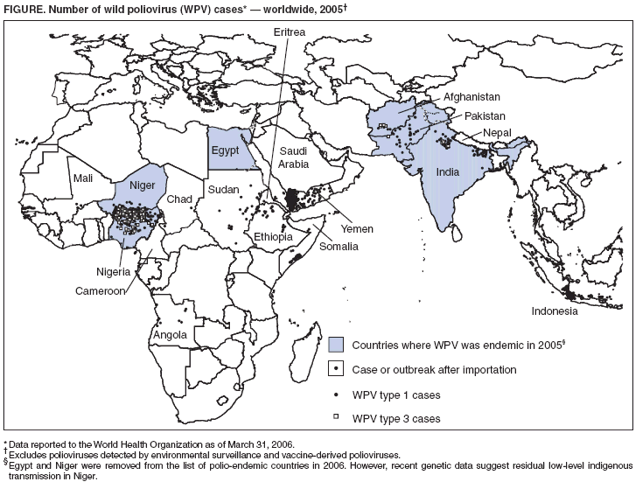
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Interruption of Wild Poliovirus Transmission --- Worldwide, January 2005--March 2006Progress toward global poliomyelitis eradication was made in 2005, despite the diversion of major financial and human resources to control outbreaks resulting from wild poliovirus (WPV) importations primarily from Nigeria. The number of countries with endemic polio has decreased to four,* compared with 125 in 1988, when the Polio Eradication Initiative was initiated by the World Health Assembly (1). In Africa and Asia, only eight of the 22 previously polio-free countries† that were reinfected since 2003 reported WPV transmission after July 2005, and transmission was curtailed substantially in all eight of these countries except Somalia (2,3). Of the three remaining polio-endemic countries in Asia (Afghanistan, India, and Pakistan), India and Pakistan also moved closer to eradication in 2005, reporting approximately half as many cases in 2005, compared with 2004. Multiple innovations were implemented during 2005, including the relicensing and use of monovalent type 1 (mOPV1) and type 3 (mOPV3) oral polio vaccines and, particularly in polio-endemic countries, increased numbers and improved quality of supplementary immunization activities (SIAs). New emphasis was placed on the systematic engagement of local leaders during SIAs and on development of SIA strategies for targeting mobile families at major train and bus transit sites. However, in certain hard-to-reach populations, SIA coverage remains inadequate to stop WPV circulation. By the end of 2005, northern Nigeria had emerged as the greatest risk for renewed international spread of WPVs; SIAs in certain areas continued to miss >40% of targeted children. This report describes global polio eradication strategies and WPV incidence during January 2005--March 2006 and outlines the greatest threats to achieving eradication. Routine OPV VaccinationGlobal routine vaccination coverage among infants with 3 doses of oral poliovirus vaccine (OPV3) was estimated at 80% in 2004,§ the most recent year with fully reported data. OPV3 coverage in 2004 varied among World Health Organization (WHO) regions, from 69% in the African Region (up from 65% in 2003) to 94% in the European Region, with considerable variation between country-level estimates within each region. OPV3 coverage in 2004 in the four countries currently on the polio-endemic list was estimated at 39% in Nigeria, 65% in Pakistan, 66% in Afghanistan, and 70% in India. These are national estimates, and areas of lower coverage within each country have been reported, especially in regions with ongoing polio transmission (e.g., Bihar and Uttar Pradesh states in India and northern Nigeria). Supplementary Immunization Activities (SIAs) with OPVIn 2005, a total of 234 SIAs with OPV (153 national immunization days [NIDs], 69 subnational immunization days [SNIDs], and 12 mop-up rounds¶) were conducted in 51 countries, administering 2.2 billion OPV doses to 371 million children aged <5 years. Of the total OPV doses used in SIAs, 473 million (22%) doses were mOPV1, and 8.4 million (4%) doses were mOPV3. Because of the substantial type-specific gains in immunity conferred by monovalent OPVs compared with trivalent OPV (4,5), mOPV1 was rapidly relicensed and administered during SIAs in 12 countries. Of the 234 SIAs, 59 were conducted in the six countries where polio was endemic during 2005: 17 SIAs in India (two NIDs and 15 SNIDs), 11 in Pakistan (eight NIDs and three SNIDs), 12 in Afghanistan (four NIDs, six SNIDs, and two mop-ups), seven in Egypt (six NIDs and one SNID), five NIDs in Niger, and seven in Nigeria (four NIDs and three SNIDs). Although use of mOPV has been effective in reducing type-specific WPV transmission in India, numerous rounds continue to ensure timely vaccination of new birth cohorts. Of the 22 previously polio-free countries reinfected since 2003, a total of 20 conducted 114 SIAs, of which 87 were NIDs, 19 were SNIDs, and eight were mop-ups. Many of these SIAs were conducted as synchronized SIAs across west and central African countries, including Sudan. Also in 2005, 25 polio-free countries conducted 61 SIAs, including 37 NIDs, to increase population immunity as a precaution to prevent the spread of possible virus importations. Acute Flaccid Paralysis (AFP) SurveillanceIn 2005, all WHO regions maintained the overall sensitivity of AFP surveillance to detect paralytic polio cases at certification-standard levels** (Table). AFP reporting continued to improve in the three regions with endemic poliovirus transmission (Africa, Eastern Mediterranean, and South-East Asia). A 43% increase in AFP reporting globally was observed, from 42,511 cases in 2004 to 61,606 cases in 2005, largely because of increased reporting from India (80% of the overall increase), Nigeria, and Pakistan. Although the certification target for AFP reporting (i.e., a nonpolio AFP rate of at least one case per 100,000 children aged <15 years) remains unchanged, in 2005 the Advisory Committee on Polio Eradication endorsed a new target of at least two cases per 100,000 children for all polio-endemic countries and countries at high risk for WPV importation (6). The intent of this recommendation was to accelerate the detection and response to circulating polioviruses. The polio laboratory network is the foundation for AFP surveillance. During 2005, WHO fully accredited 97% of the 145 global poliovirus laboratory network laboratories, which analyzed more than 120,000 stool samples that year. Compared with 2004, the laboratory network workload increased by 50% in 2005. This increase was highest in the WHO South-East Asian Region (90%), followed by the Eastern Mediterranean Region (45%) and African Region (25%). Laboratory network strategies were adjusted to meet the increased demands. Overall, 95% of virus isolation results were reported within 28 days, and >95% of intratypic differentiation results were reported within 14 days. WPV IncidenceAs of March 31, 2006, a provisional total of 1,948 polio cases had been reported globally for 2005, compared with 1,255 cases in 2004 (Figure, Table). During both 2004 and 2005, Nigeria had the largest number of cases: 782 cases in 2004 (62% of all cases globally) and 799 cases in 2005 (41%). The 55% global increase in cases in 2005 resulted from three large outbreaks after importation of Nigeria polioviruses into previously polio-free countries: Yemen (478 cases), Indonesia (303), and Somalia (185). In 2005, for the first time, more cases were reported from reinfected countries (53% of the total) than from polio-endemic countries; 94% of cases worldwide were caused by viruses that originated in northern Nigeria. After completing 12 months without evidence of indigenous poliovirus transmission, Egypt and Niger were removed from the list of polio-endemic countries in February 2006. Interruption of WPV transmission in Egypt, where the natural risk factors for intense poliovirus transmission have been high, represents a major milestone for the Polio Eradication Initiative. Polio surveillance in Egypt has been highly sensitive, combining both AFP and environmental surveillance systems. The last indigenous poliovirus in Egypt was detected in a sewage sample collected in January 2005. All 10 cases reported from Niger during 2005 were caused by WPV directly imported from Nigeria. Recent genetic data from 2006, however, suggest residual low-level transmission in Niger, although this represents a substantial decrease from previous high levels of transmission. Two large polio-endemic countries in Asia registered 50% declines in cases from 2004 to 2005. India reported 66 cases in 2005, down from 134 cases in 2004, and Pakistan reported 28 cases in 2005, down from 53 cases in 2004. Afghanistan reported nine cases in 2005, compared with four cases in 2004. The 799 cases reported by Nigeria in 2005 were eight times the total number reported by the three polio-endemic Asian countries combined. Of these 799 cases, 746 (93%) were reported from 10 northern Nigerian states (of 37 total states), where both type 1 and type 3 poliovirus continued to circulate widely. Type 3 WPV was observed only in northern Nigeria, in two small foci in northern India, in southern Afghanistan, and in Pakistan near the southern Afghanistan border. Also during 2005, the largest number of paralytic polio cases (46) known to be caused by circulating vaccine-derived poliovirus (cVDPV) occurred on a small island off East Java in Indonesia. As with other previously identified VDPV outbreaks, low OPV coverage enabled neurovirulent vaccine-derived poliovirus to emerge and circulate (6). Reported by: Polio Eradication Group, World Health Organization, Geneva, Switzerland. Div of Viral Diseases and Global Immunization, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:Despite challenges during the past 2 years, the world has moved closer to eradicating polio. Although nationwide OPV vaccination was resumed in late 2004, widespread poliovirus circulation in northern Nigeria remains the greatest threat to global polio eradication. Data on OPV coverage of nonpolio AFP cases from the six northern states that contributed 65% of all polio cases in Nigeria indicate that >40% of children aged <5 years have never received OPV. Southern Nigeria was largely polio-free by the end of 2005; however, the continued epidemic in the north indicates that critical improvements in SIA coverage are needed in northern states. On the basis of lessons learned from the 2003--2005 resurgence of polio in previously polio-free countries, and to limit the potential of further international spread of poliovirus, the Advisory Committee on Polio Eradication issued specific recommendations in October 2005 to guide the future response to any circulating poliovirus in a previously polio-free area (6), calling for rapid and large-scale responses and use of type-specific mOPV. The WHO executive board endorsed these recommendations in early 2006. With six or more large-scale SIAs each year in the remaining polio-affected countries, vaccination refusals present an ongoing challenge to achieving the high rates of OPV coverage needed. To ensure community acceptance and compliance, social mobilization, communication activities, and other interventions (e.g., administration of other vaccines and distribution of mosquito bednets) have become critical to the success of SIAs and will be a key priority in 2006. The cVDPV outbreak in Indonesia illustrates the risk for emergence of cVDPV in areas with low levels of population immunity, reinforcing the importance of ensuring uniformly high SIA coverage and the necessity to eventually stop all routine use of OPV once WPV is eradicated (5,7). Key to achievement of a polio-free world is the continued support of the international polio partnership, which is necessary to allow full implementation of the new strategic approach, including use of mOPV, to interrupt transmission in remaining polio-endemic areas. The greatest risk to global polio eradication and to the polio-free status of most countries of the world is the ongoing uncontrolled poliovirus transmission in several northern Nigerian states. Aggressive response to the challenges posed by importations and ongoing transmission characterized global polio eradication activities in 2005. Eradication efforts will ultimately require ongoing commitment by governments and health workers at all levels to ensure that all children are appropriately vaccinated. References
* The four countries currently on the polio-endemic list are Afghanistan, India, Nigeria, and Pakistan. Egypt and Niger were removed from the list in February 2006 after 12 months without indigenous WPV transmission. However, recent genetic evidence suggests residual low-level transmission in Niger. † The eight reinfected countries with transmission after July 2005 were Angola, Bangladesh, Chad, Ethiopia, Indonesia, Nepal, Somalia, and Yemen. The 14 countries reinfected since 2003 without transmission after July 2005 were Benin, Botswana, Burkina Faso, Cameroon, Central African Republic, Côte d'Ivoire, Eritrea, Ghana, Guinea, Lebanon, Mali, Saudi Arabia, Sudan, and Togo. § World Health Organization (WHO)/UNICEF estimates of OPV3 coverage, according to the 2005 summary of the WHO vaccine-preventable diseases monitoring system. ¶ Subnational immunization days can vary in size and location within a given country, but most commonly target a region consisting of several states. Mop-up campaigns target children living in specific high-risk districts known to have experienced recent WPV circulation. ** Criteria for certification are as follows: 1) a nonpolio AFP rate of at least one case per 100,000 children aged <15 years, 2) 80% of AFP cases with adequate stool specimens, and 3) 100% of stool specimens processed in a laboratory accredited by WHO.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 4/27/2006 |
|||||||||
|