|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
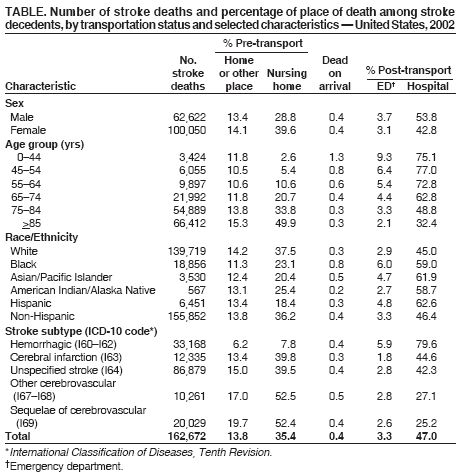
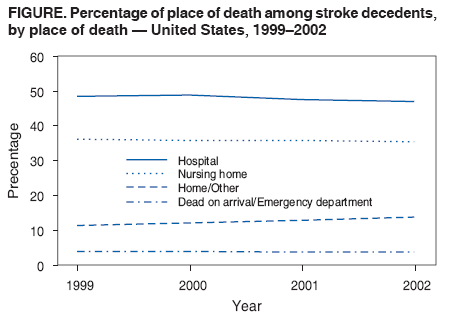
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Place of Death After Stroke --- United States, 1999--2002Stroke is the third leading cause of death in the United States (1). Successful acute stroke intervention depends on early recognition of symptoms, prompt emergency transport, and rapid in-hospital treatment. However, approximately half of stroke decedents die before admission to the hospital (2). During 1990--1998, the proportion of stroke deaths that occurred in hospitals declined, and the proportion occurring before transport to hospitals increased (3). This report summarizes trends in the place of death among all stroke decedents, the proportion of stroke deaths occurring before emergency assistance arrives, and characteristics associated with place of death. Among 162,672 persons who died of stroke in 2002, 49.2% died pre-transport, 0.4% were dead on arrival (DOA), 3.3% died in emergency departments (EDs), and 47.0% died after admission to a hospital. Early patient and bystander recognition of stroke symptoms and timely action in calling for emergency assistance might reduce the number and proportion of stroke deaths. In addition, improving timely arrival of emergency care and appropriate treatment of stroke patients can reduce the proportion of pre-transport deaths and serious sequelae that lead to severe disabilities. National mortality statistics in this report were based on death-certificate information from all 50 states and the District of Columbia (DC) that was reported to CDC. Demographic data (e.g., race/ethnicity, sex, and age) and place of death on death certificates were provided by funeral directors or family members. The death certificate item on where death was pronounced was used as a proxy source of information for place of death. Stroke-related deaths were defined as those for which the underlying cause reported on the death certificate by a physician, medical examiner, or coroner was classified according to International Classification of Diseases, Tenth Revision (ICD-10) codes I60--I69. These include hemorrhagic (I60--I62), cerebral infarction (I63), unspecified (I64), occlusion and stenosis (I65--I66), other cerebrovascular deaths (I67--I68), and deaths with cerebrovascular sequelae (I69). Place of death was defined as pre-transport death (death pronounced in a nursing home or at home or other place), post-transport death (death pronounced in the ED or hospital), DOA, or unknown. The distribution of place of death among stroke decedents in the United States was assessed during 1999--2002 and the percentage change was assessed from 1999 to 2002. In 2002, a total of 162,672 deaths from stroke occurred among U.S. residents, with an age-adjusted death rate of 56.2 per 100,000 population. Of these stroke-related deaths, 49.2% occurred pre-transport (35.4% in a nursing home and 13.8% in the decedent's home or other place), 0.4% were DOA, 50.3% occurred post-transport (3.3% in EDs and 47.0% after admission to a hospital), and information was unknown for <0.1%. The proportion of pre-transport deaths among stroke decedents in 2002 increased among successive age groups, particularly for deaths occurring in nursing homes (Table). For example, the proportion of deaths that occurred pre-transport was 14.4% among stroke decedents aged <45 years (11.8% at home or other place and 2.6% in nursing homes), compared with 65.2% among those aged >85 years (15.3% at home or other place and 49.9% in nursing homes). The proportion of pre-transport deaths was higher among females than males, among whites than other races, and among non-Hispanics than Hispanics. However, the proportion of stroke-related deaths that occurred in EDs was higher for blacks than other racial groups and higher for Hispanics than non-Hispanics. Asians/Pacific Islanders had the highest proportion of post-transport stroke deaths that occurred in a hospital compared with all racial groups. The highest proportion of pre-transport stroke deaths was observed among persons who died of sequelae of cerebrovascular diseases (72.1%) or other cerebrovascular conditions (69.5%), followed by unspecified stroke (54.5%), cerebral infarction (53.2%), and hemorrhagic stroke (14.2%). Those who died of a hemorrhagic stroke had the highest proportion of deaths in EDs (5.9%) and hospitals (79.6%) (Table). The U.S. age-adjusted stroke death rate steadily decreased from 61.6 per 100,000 population in 1999 to 56.2 per 100,000 population in 2002. However, minimal change was observed in the distribution of place of death and characteristics associated with place of death among stroke decedents from 1999 to 2002 (Figure). The place of death did not change from 1999 to 2002 for groups defined by age, sex, or race/ethnicity. The relative increase from 1999 to 2002 in the proportion of stroke decedents dying pre-transport was 3.4% for all strokes, 8.5% for hemorrhagic strokes, 7.1% for other cerebrovascular deaths, 4.9% for cerebral infarctions, 4.3% for cerebrovascular sequelae, and 3.4% for unspecified strokes. Reported by: C Harris, MPH, C Ayala, PhD, JB Croft, PhD, Div for Heart Disease and Stroke Prevention, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that overall national trends and characteristics associated with place of death among stroke decedents did not change from 1999 to 2002. In 2002, approximately half of all stroke deaths occurred pre-transport. A substantial proportion of pre-transport stroke deaths occurred in nursing homes rather than at home or another place, and a greater proportion of post-transport deaths occurred after hospital admission rather than in EDs. Pre-transport stroke deaths increased with successive age groups and occurred more frequently among females than males, whites than other racial groups, non-Hispanics than Hispanics, and those who died with sequelae of cerebrovascular diseases than other stroke subtypes. These proportions and characteristics of pre-transport stroke deaths remain consistent with previously published data, which indicated that 49.5% of all stroke deaths in 1998 occurred in hospitals, 46.1% occurred pre-transport, and 0.6% of persons were DOA (3). However, the results from this report and the 1998 report are not directly comparable because of changes in ICD coding from the ninth to the tenth revisions. Sex differences noted in pre-transport stroke deaths could be attributed in part to differences in emergency response time. One study indicated that during a stroke, women might have a longer delay time in reaching the hospital than men (4). Although delayed emergency response might partially explain the disparity between males and females, the findings in this report indicate that approximately 40% of stroke deaths in females occurred in a nursing home. In 1999, women accounted for approximately 70% of the nursing home population (5); in addition, women aged >80 years or any hospital patients admitted from a nursing home are more likely to have do-not-resuscitate orders than men aged >80 years, younger women, or hospital patients admitted from home (6). Blacks, compared with Hispanic and non-Hispanic whites, might be more likely to use emergency medical services (EMS) for transport to the hospital, thus reaching the hospital earlier (4) and supporting the finding that a smaller proportion of blacks die pre-transport than whites. In addition, one study observed that blacks and Hispanics also might be less likely to have do-not-resuscitate orders than whites, regardless of age (6). Two state program priorities for CDC's National Heart Disease and Stroke Prevention Program are to increase public awareness of signs and symptoms of a stroke and to improve emergency response for stroke. State efforts might have increased the capacity of EMS response to acute stroke. For example, Texas has adopted the Emergency Health Care Act, which mandates creation of a stroke committee, a statewide stroke emergency transport plan, and stroke facility criteria with the intent to construct an emergency treatment system in Texas so that stroke victims can be identified quickly and transported to appropriate stroke treatment facilities (7). The finding in this report indicate that hemorrhagic stroke patients were less likely to die before reaching the hospital, which supports previous findings that hemorrhagic stroke patients use EMS services more frequently (8) and are seen earlier by the neurologist than other stroke subtype patients (4). Persons dying of cerebrovascular sequelae, followed by other cerebrovascular conditions and unspecified stroke deaths, had the highest proportion of pre-transport deaths, which could indicate that they had comorbidities or do-not-resuscitate requests and might have been less likely to seek further medical attention or use EMS services (9). Further investigation is needed to clarify the impact that do-not-resuscitate requests in homes, nursing homes, and end-state disease care settings have on the high proportion of pre-transport stroke deaths. The findings in this report are subject to at least two limitations. First, death-certificate data are subject to error in the certification of the underlying cause of death (1). Second, death-certificate place of death data are based on where the decedent is pronounced dead and not necessarily where the decedent died. Therefore, the difference in reported place of death and actual place of death could result in either overestimates or underestimates in the proportion of stroke deaths that occurred in a specified location. However, the quality of place of death data has been investigated, with results indicating the consistency for reporting deaths in a hospital is 88.3% and is 92.9% for reporting deaths in either nursing homes or personal-care homes (10). Because approximately 80% of deaths in this report were classified as occurring in hospitals or nursing homes, bias likely did not affect the results of this analysis (10). The substantial proportion of pre-transport stroke deaths in the United States continues to illustrate the need for early recognition of stroke signs and symptoms followed by expeditious transport of stroke victims to hospitals, preferably hospitals recognized as stroke centers and treatment facilities. Policies and stroke emergency transport plans should be in place for all EMS systems in every state. Such plans should mandate stroke as an emergency event and should have protocols for identifying, transporting, and treating stroke patients to reduce the proportion of pre-transport stroke deaths. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 5/17/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|