|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
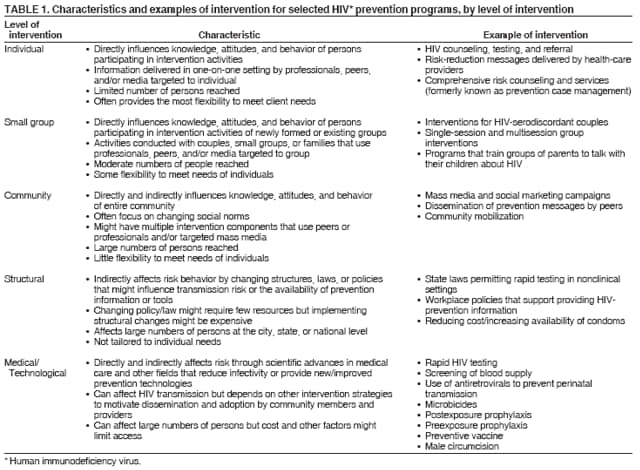
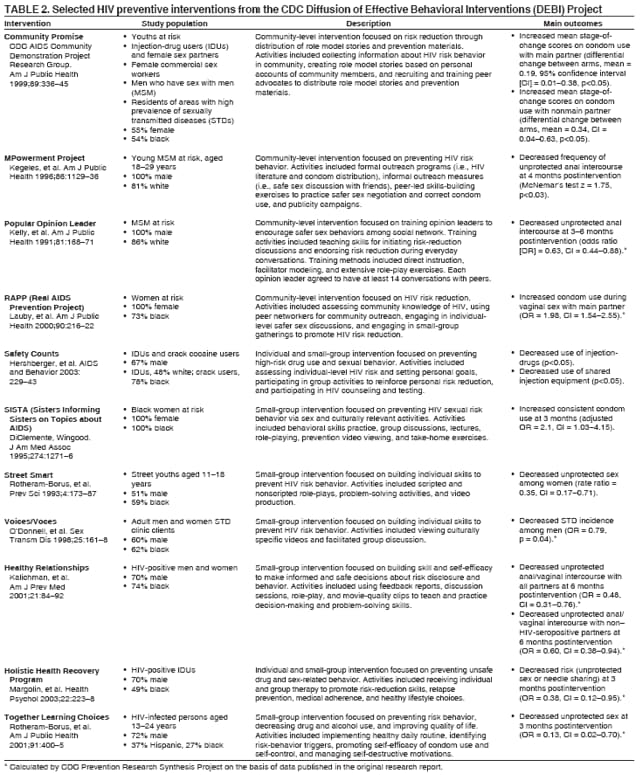
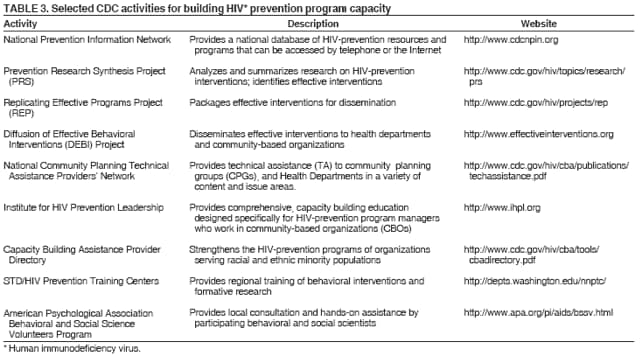
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Evolution of HIV/AIDS Prevention Programs --- United States, 1981--2006When the first cases of what would become known as acquired immunodeficiency syndrome (AIDS) were reported in 1981, the magnitude of the epidemic and the numbers of deaths were unimaginable. During the next 25 years, an unprecedented mobilization of individual, community, and government resources was directed at stopping the epidemic. CDC currently supports a wide range of human immunodeficiency virus (HIV) prevention activities in the United States, including 1) collection of behavioral and HIV/AIDS case surveillance data that document trends in the epidemic and risk behaviors; 2) programs conducted by state, territorial, and local health departments, community-based and national organizations, and education agencies; 3) capacity building to improve HIV-prevention programs; 4) program evaluation to monitor the delivery and outcomes of prevention services; and 5) research leading to new strategies for preventing transmission of HIV/AIDS. Since 1994, local and state health departments have allocated resources to specific programs and populations through local community planning processes that involve health department staff, prevention providers, and members of affected communities (1). A three-pronged approach has been developed, consisting of 1) prevention activities directed at persons at high risk for contracting HIV; 2) HIV counseling, testing, and referral services; and 3) prevention activities directed at improving the health of persons living with HIV and preventing further transmission. Persons at High Risk for Contracting HIVThe first HIV-prevention programs in the United States were grassroots measures initiated in 1982 predominantly by homosexual men in San Francisco, California, and New York City (2). These and other early HIV-prevention activities primarily were designed to increase AIDS awareness, reduce unfounded fears about transmission, and provide basic information regarding symptoms, likely transmission routes, and risk-reduction strategies. Early CDC activities included establishment of the National AIDS Information Line (1983) and National AIDS Clearinghouse (1987), institution of the nationwide America Responds to AIDS public information campaign (1987), and distribution of Understanding AIDS (1988), a brochure prepared in consultation with U.S. Surgeon General C. Everett Koop; this was the first mailing regarding a major public health problem that was delivered to every residential mailing address in the United States (3). CDC programs during the mid- to late 1980s addressed high-school and college-aged populations, persons at increased risk for HIV, racial and ethnic minority populations, perinatal transmission, and health-care workers (3). These programs increased basic knowledge about HIV transmission and prevention, reduced risk behavior within populations at high risk for infection, and decreased negative attitudes toward persons living with HIV/AIDS (4). However, as important as these gains were, they were not sufficient to motivate behavior change among some persons at high risk for HIV infection. More intensive, targeted interventions were developed, including the five-city CDC AIDS Community Demonstration Projects (1989), which produced effective, community-level interventions for difficult-to-reach populations that led to increased condom use with main and nonmain sex partners (5). A wide range of behavioral intervention strategies, operated at individual, small-group, and community levels, and complemented by structural interventions and medical/technological advances, has been implemented for persons at high risk for HIV infection (Table 1) (4). Behavioral interventions were observed to substantially reduce HIV risk while remaining cost effective or cost saving for a wide range of populations at high risk (4). The CDC HIV Prevention Research Synthesis Project has conducted meta-analyses of data from scientifically rigorous intervention trials since 1996. These analyses have determined that behavioral interventions substantially reduce sexual risk among young adults, men who have sex with men (MSM), heterosexual men and women, and drug users (6--9). More than 50 interventions for populations at high risk have been identified that meet stringent criteria for efficacy and scientific rigor (10--12). A growing number of these evidence-based interventions have been packaged for use in local HIV-prevention programs (13,14). These packages, or kits, and training on how to use them are available through the CDC Diffusion of Effective Behavioral Interventions (DEBI) project (Table 2) (15). In addition, CDC supports a wide range of other activities designed to build the capacity of local HIV-prevention providers and their organizational infrastructures (Table 3). HIV Counseling, Testing, and Referral ServicesIn 1983, identification of HIV as the cause of AIDS (16,17) made possible the development of tests to detect the virus. In January 1985, the U.S. Public Health Service (PHS) issued provisional recommendations for screening donated blood and plasma in anticipation of a commercial HIV-antibody test (18). The first test for HIV antibody was licensed by the Food and Drug Administration in March 1985 and was widely implemented in blood banks, plasma collection centers, health departments, and clinical-care settings. Concurrent with licensing of the new test, PHS announced availability of funding for health departments to establish test sites that would provide an HIV-test alternative to blood donation for persons at high risk to enable them to learn their HIV-antibody status. By the end of 1985, a total of 874 alternate test sites had been established, and 79,100 persons had been tested (19). In 1986, new recommendations published by CDC substantially expanded use of HIV-antibody testing (20). These recommendations encouraged confidential and anonymous HIV-antibody testing of persons at high risk in combination with risk-reduction counseling and, for HIV-seropositive persons, referral of sex and needle-sharing partners for medical evaluation and testing. Since then, the number of CDC-supported test sites has increased to approximately 11,000, providing approximately 2.2 million HIV-antibody tests in 2004 (CDC, unpublished data, 2006). For most of the epidemic, HIV-antibody testing has required two visits. The first visit consisted of a pretest counseling session and a blood draw, but test results and posttest counseling were not provided until the second visit (usually 2 weeks after the blood draw), after completion of the laboratory test. The need for a second visit posed a major barrier; depending on the setting and population, 10% to >50% of persons tested failed to return for their results (21,22). Counseling was initially based on standard messages about the test, the meaning of positive and negative test results, and risk reduction. Early studies of HIV counseling and testing observed considerable reductions in risk among persons who learned that they were HIV seropositive but found little change among those who were HIV seronegative (23). On the basis of these findings, CDC recommended a shift to client-centered counseling that emphasized increasing the client's perception of risk and developing a personalized risk-reduction plan (24). This approach substantially increased condom use and decreased new sexually transmitted diseases (STDs) among HIV-seronegative patients at STD clinics (25). In recent years, CDC has issued new guidelines and supported new initiatives to make HIV-antibody testing more accessible, incorporate advances in testing technologies, better integrate testing into routine medical care, recognize resource and provider constraints, and accommodate the diverse needs and preferences of persons seeking testing (26,27). The availability of oral fluid, urine, and finger-prick testing, along with rapid tests, has made it easier to provide HIV testing in a wide range of clinical and nontraditional settings and has led to new strategies for reaching more persons with undiagnosed HIV infection (26). Rapid tests produce results in 20 minutes and make it possible to give HIV-seronegative and provisional HIV-seropositive test results in a single visit, increasing the percentage of persons who receive their test results in a single visit to more than 95% in many testing programs (28,29). CDC also is developing recommendations to make HIV screening a routine part of medical care, remove barriers that hamper early HIV diagnosis and treatment, and demonstrate and disseminate effective models for testing in clinical and nontraditional settings. Persons Living with HIVThe availability of highly active antiretroviral therapy (HAART) in the mid-1990s led to a dramatic decline in AIDS-related deaths and a new era in which many persons newly diagnosed with HIV can expect to lead active and productive lives that extend for decades. This treatment breakthrough underscored the need for additional prevention services for the estimated 1.0--1.2 million persons living with HIV in the United States (30). Although most persons who have HIV infection diagnosed reduce or eliminate behaviors that place themselves at risk for STDs and transmitting HIV to others, some do not eliminate risk behaviors, and others resume risk behaviors later in life (23,31). Historically, most prevention programs were designed to address the needs of persons who were at risk for contracting HIV. During the first decade of the epidemic, fewer prevention programs focused on persons living with HIV with the following notable exceptions: 1) measures to prevent perinatal transmission; 2) HIV counseling, testing, and referral programs to identify undiagnosed HIV infections and to provide HIV-seropositive persons with risk-reduction counseling, partner-referral services, and referrals to medical care and other supportive services around the time of diagnosis; 3) prevention case management for HIV-seropositive and other persons with multiple needs; and 4) pioneering community and health department-based programs that integrate prevention with medical or social services for persons living with HIV (22). In 2001, CDC introduced the Serostatus Approach to Fighting the HIV Epidemic (SAFE), which defined a framework for improving the health of persons living with HIV and preventing transmission to others (32). In 2003, CDC implemented the Advancing HIV Prevention (AHP) initiative (26), which formally adopted prevention with persons living with HIV as a core element of a comprehensive approach to HIV prevention. AHP funded large-scale demonstration projects to evaluate public health strategies for identifying undiagnosed HIV infections and preventing transmission by persons living with HIV (26). Recommendations were made to incorporate HIV prevention into the medical care of HIV-seropositive patients (33). A meta-analytic study of 12 HIV trials published during 1988--2004 determined that behavioral interventions for persons living with HIV led to a 43% relative reduction in unprotected sex and also reduced acquisition of STDs (34); CDC is disseminating effective behavioral interventions for persons living with HIV to state and local programs through capacity-building activities (Tables 2 and 3). Successes and Current ChallengesConsiderable success in the prevention of HIV infection in the United States has been achieved. HIV testing and donor deferral have markedly increased the safety of the nation's blood supply. Perinatal transmission of HIV has been greatly reduced (35). Reductions in needle sharing have resulted in a substantial decrease in HIV transmissions associated with injection-drug use (36,37). These and other prevention successes have reduced incidence of HIV infection from more than 150,000 cases per year in the mid-1980s to approximately 40,000 cases per year since the late 1990s. Despite this success, considerable prevention challenges remain. Racial/ethnic disparities have increased during the past 25 years, especially among black men and black women (38). HIV prevalence remains high among MSM overall, new cases of HIV increased substantially among MSM from 2003 to 2004 (37), and prevalence among black MSM was reported as high as 46% in a study in five U.S. cities during 2004--2005 (39). The growing number of persons living with HIV means that more persons are potentially capable of transmitting the virus to others, and existing resources might not be adequate to ensure that all HIV-seropositive persons have access to appropriate care, treatment, and prevention services. Despite the substantial progress, an estimated one quarter of persons living with HIV do not know they are infected and are at considerable risk for developing AIDS and unknowingly transmitting HIV (30). Changes in beliefs regarding the severity of HIV infection, prevention fatigue, and increases in methamphetamine abuse and STDs also present new challenges to HIV prevention. These challenges are compounded by deep-rooted social problems and inequities. Poverty, homelessness, racism, homophobia, and gender inequality all affect HIV risk and can limit the effective delivery of prevention programs and medical services (40). Other social factors might also be associated with increased risk behaviors. HIV stigma and discrimination remain pervasive, causing some persons to avoid HIV testing and others living with HIV to delay medical care, be less adherent to care, and fear disclosing their HIV status to others (41). HIV-prevention programs must continue to evolve to address these challenges, incorporating biomedical advances and findings (e.g., preexposure and postexposure prophylaxis, microbicides, male circumcision [42], vaccine development, and effects of antiretroviral treatment on infectivity) and innovations in HIV-testing technologies, and other breakthroughs. New interventions are needed for underserved populations at high risk, to improve effectiveness of existing interventions, and to further develop the capacity of health departments and community-based organizations to implement effective behavioral and public health interventions. In addition, the need continues for CDC and its local, state, and national prevention partners and affected communities to work together to improve the quality and efficiency of HIV-prevention programs to best serve the prevention needs of persons who are at risk for or living with HIV infection. Reported by: RJ Wolitski, PhD, KD Henny, PhD, CM Lyles, PhD, DW Purcell, JD, PhD, JW Carey, PhD, N Crepaz, PhD, A O'Leary, PhD, TD Mastro, MD, JC Cleveland, MS, AK Nakashima, MD, RS Janssen, MD, Div of HIV and AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed). References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/1/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|