|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
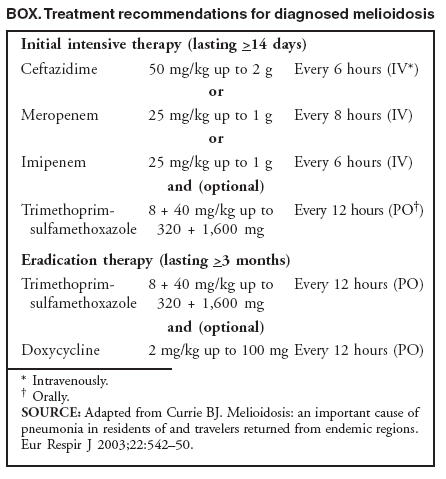
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Imported Melioidosis --- South Florida, 2005In 2005, two cases of melioidosis (one in August, one in October) were reported to the Florida Department of Health, the first cases since reporting the disease became mandatory in Florida in 2003. In one case, Burkholderia pseudomallei was not recognized as the bacterium that causes the disease melioidosis, which led to a delay in reporting the case to the local health department. In both cases, delayed recognition and unsafe laboratory practices resulted in laboratory workers being exposed to B. pseudomallei. This report summarizes the clinical and laboratory aspects of the cases and the epidemiologic study conducted by the Florida Department of Health. The findings emphasize the need for improved laboratory recognition and reporting of B. pseudomallei, safe laboratory handling of B. pseudomallei, and close adherence to antibiotic regimens for treating and preventing recurrence of melioidosis. Melioidosis is a potentially serious illness caused by the gram-negative, saprophytic bacterium B. pseudomallei (formerly Pseudomonas pseudomallei). Most commonly, the disease manifests as pneumonia, with or without septicemia, but melioidosis also can cause abscesses, particularly of the skin and soft tissues. Abscesses of the internal organs are less common (1). Melioidosis is endemic in Southeast Asia and northern Australia but can be found sporadically in tropical areas between latitudes 20º north and south (2). In areas where melioidosis is endemic, humans become infected by inoculation and inhalation through exposure to organisms in soil and water (2); the median incubation period from exposure to illness onset is 9 days (range: 1--21 days). Persons with type 2 diabetes are especially susceptible to symptomatic infection; additional risk factors include thalassemia, renal disease, chronic alcoholism, and liver disease (2). Human immunodeficiency virus has not been determined to be a risk factor (2). Asymptomatic infections can arise, and symptomatic reactivation of the disease can occur years after exposure. Where melioidosis is endemic, the case-fatality rate for cases with septicemia and pulmonary involvement ranges from 20% to 50%. Reduced fatality rates have been associated with improved antibiotic regimens and supportive care (2). Case ReportsCase 1: Broward County. On August 22, a man aged 48 years with a history of adult-onset diabetes and Guillain-Barré syndrome was evaluated at a local hospital for back pain, fever (102.6ºF [39.2ºC]), and bilateral lower extremity weakness and numbness. He received a diagnosis of left lower lobe pneumonia, perirectal abscess, which was drained on admission, and possible recurrent Guillain-Barré syndrome. He was admitted for antibiotic treatment with ceftriaxone and azithromycin. On August 27, B. pseudomallei was identified in cultures of blood drawn on admission. On August 31, the patient was discharged with a prescribed 21-day regimen of oral levofloxacin. On September 11, he returned with severe back and left-sided pleuritic chest pain. In the emergency department, he had onset of acute bilateral leg paralysis and sensation loss. Spinal magnetic resonance imaging revealed epidural abscesses along thoracic vertebrae T6--T10. The patient underwent emergency surgery for spinal decompression. On September 16, B. pseudomallei was isolated from cultures of abscess fluid. On September 26, the patient remained paraplegic and was discharged to inpatient rehabilitation, with a prescribed regimen of 8 weeks of intravenous imipenem/cilastatin and ceftazidime followed by 20 weeks of oral antibiotics. The epidemiologic investigation determined that the patient had traveled to Honduras during July 17--August 7, where he visited the city of La Ceiba (capital of Atlántida Department) and the island of Roatán. He had not been ill while traveling and did not recall being injured. He traveled with seven family members who were not ill and had no known contact with ill persons. In addition, the patient reported that before his trip to Honduras, he had never traveled out of the country. Case 2: Miami-Dade County. On September 22, a woman aged 80 years was admitted to a local hospital with pneumonia after 4 days of fever (103ºF [39.4ºC]), headache, weakness, and muscle pain. She was treated with intravenous fluids, ceftriaxone, and azithromycin. On September 23, she experienced a myocardial infarction and respiratory complications, and on September 24, her antibiotics were changed to vancomycin and cefepime. She died on September 24. On September 26, local public health authorities were notified that B. pseudomallei had been identified in a culture of blood drawn when the patient was admitted. The isolate was sent to the Florida Department of Health reference laboratory in Miami, where the presence of B. pseudomallei organisms was corroborated by real-time polymerase chain reaction. The epidemiologic investigation indicated that the patient had been a resident of San Juan Pueblo in Atlántida Department in Honduras. She had arrived in Florida on September 18 to visit family members. Laboratory InvestigationOn October 4, more than 5 weeks after B. pseudomallei organisms had been isolated in case 1, the Broward County Health Department received the report from the hospital infection-control practitioner. No isolates had been saved for confirmation at the state public health laboratory. An investigation into the hospital's reporting procedures for this case determined that the laboratorians handling the specimens did not associate the organism B. pseudomallei with the disease melioidosis, which is a mandatory reportable disease in Florida. Laboratorians from the hospitals in Broward County and Miami-Dade County were contacted on October 12 and September 26, respectively, regarding the possibility of exposure while handling the specimens. Exposures were considered high risk if isolates had been manipulated outside of a biosafety cabinet or if isolate manipulation could have resulted in aerosol or droplet formation (e.g., sniffing an open culture plate to detect characteristic odors emitted by certain bacteria). A total of nine laboratorians (six from the Broward County hospital and three from the Miami-Dade County hospital) had high-risk exposures. All were offered prophylaxis and anti--B. pseudomallei antibody testing. The three laboratorians in the Miami hospital reportedly sniffed the culture plates, and all requested prophylaxis. None of the six laboratorians in the Broward County hospital had sniffed the plates containing B. pseudomallei, but they all had handled the cultures outside of a biosafety cabinet. On October 19, specimens for diagnostic serology were obtained from these six laboratorians; all were negative for presence of B. pseudomallei, and no prophylaxis was prescribed. None of the nine exposed laboratorians reported symptoms consistent with melioidosis. Reported by: A Kite-Powell, MS, JR Livengood, MD, J Suarez, R Hopkins, MD, Florida Dept of Health. TA Clark, MD, Div of Foodborne, Bacterial, and Mycotic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases (proposed); D Chertow, MD, EIS Officer, CDC. Editorial Note:Melioidosis is a rare disease in the United States; approximately five cases are reported annually, although it is not a nationally notifiable disease (3). The cases in this report are the first to be reported from Florida. However, melioidosis is a relatively common disease in areas where it is endemic, is likely underreported in nonendemic tropical areas (4), and can affect travelers returning from tropical regions (5). The bacteria are found in contaminated water and soil in melioidosis-endemic areas worldwide. The organisms can be aerosolized and are capable of producing severe and even fatal illness. No vaccine is available to prevent melioidosis (2,6). A current treatment recommendation for melioidosis includes an initial intensive treatment phase followed by eradication therapy (Box). Relapse rates can increase from 10% to 30% when antibiotic treatment is conducted for less than 8 weeks (1). Laboratory workers with high-risk exposures can be offered postexposure prophylaxis with doxycycline (2 mg/kg up to 100 mg orally, twice daily) or trimethoprim-sulfamethoxazole (8 + 40 mg/kg, up to 320 + 1,600 mg orally, twice daily) (7), but the optimum duration of treatment and its efficacy have not been defined clearly by human studies. Serologic assays are not readily available for B. pseudomallei and are not useful in endemic settings (because they do not differentiate between active infection and background seroprevalence) but have proven useful for previously unexposed persons who have experienced a high-risk exposure (2,5). B. pseudomallei has been classified as a category B biologic terrorism agent by CDC.* All Level A laboratories, such as private clinical laboratories and hospital laboratories, should have procedures for isolation and presumptive identification of potential biologic terrorism agents, including timely submission of isolates to a laboratory in the Laboratory Response Network (LRN)† that is capable of confirmatory testing and reporting of cases to local public health authorities. To improve the existing system and minimize human error in identifying possible biologic terrorism agents, the Broward County Health Department is exploring new methods with local hospital information technology staff. For example, a system might automatically produce a written alert and reporting-requirement instructions on laboratory printouts when particular organisms are detected. Although risk for occupational exposure to B. pseudomallei in clinical laboratories exists, laboratory-acquired infections are rare. Laboratory exposures that have resulted in the most recent cases of infection involved aerosols, alone or in combination with exposure to nonintact skin (8). In one study, three cases of asymptomatic seroconversion were reported among laboratorians in an area where melioidosis is endemic, making difficult a determination of whether infection resulted from occupational or environmental exposure (9). CDC recommends that clinical specimens suspected of containing B. pseudomallei be manipulated using biosafety level (BSL)-2 containment practices, equipment, and facilities (10). Sniffing culture plates is an unsafe laboratory procedure and should be prohibited. Manipulations of an isolate that might result in aerosol or droplet exposure or contact with nonintact skin should be conducted using BSL-3 containment practices, equipment, and facilities. In addition, improved communication between physicians and laboratorians might reduce the risks to laboratorians. Clinicians should notify laboratorians when specimens are obtained from patients with symptoms, risk factors, or history suggestive of melioidosis. References
* Category B agents (i.e., second highest priority agents) include those that are moderately easy to disseminate, result in moderate morbidity rates and low mortality rates, and require specific enhancements of CDC's diagnostic capacity and enhanced disease surveillance. Additional information available at http://www.bt.cdc.gov/agent/agentlist-category.asp. † The LRN, established by CDC in 1999, is an integrated national and international network of laboratories that are equipped to respond rapidly to acts of chemical or biologic terrorism, emerging infectious diseases, and other public health threats and emergencies. Additional information available at http://www.bt.cdc.gov/lrn.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 8/16/2006 |
|||||||||
|