|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
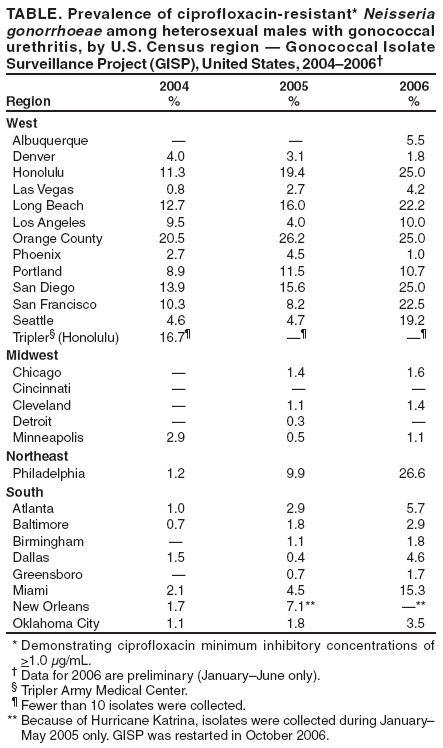
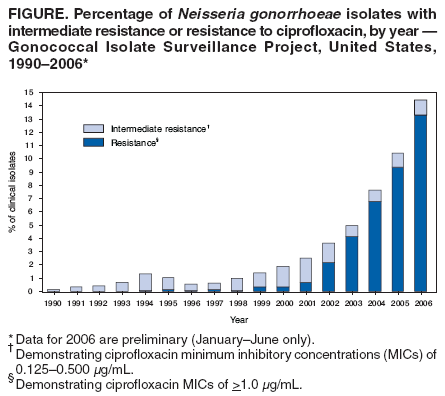
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update to CDC's Sexually Transmitted Diseases Treatment Guidelines, 2006: Fluoroquinolones No Longer Recommended for Treatment of Gonococcal InfectionsIn the United States, gonorrhea is the second most commonly reported notifiable disease, with 339,593 cases documented in 2005 (1). Since 1993, fluoroquinolones (i.e., ciprofloxacin, ofloxacin, or levofloxacin) have been used frequently in the treatment of gonorrhea because of their high efficacy, ready availability, and convenience as a single-dose, oral therapy. However, prevalence of fluoroquinolone resistance in Neisseria gonorrhoeae has been increasing and is becoming widespread in the United States, necessitating changes in treatment regimens. Beginning in 2000, fluoroquinolones were no longer recommended for gonorrhea treatment in persons who acquired their infections in Asia or the Pacific Islands (including Hawaii); in 2002, this recommendation was extended to California (2). In 2004, CDC recommended that fluoroquinolones not be used in the United States to treat gonorrhea in men who have sex with men (MSM) (3). This report, based on data from the Gonococcal Isolate Surveillance Project (GISP), summarizes data on fluoroquinolone-resistant N. gonorrhoeae (QRNG) in heterosexual males and in MSM throughout the United States. This report also updates CDC's Sexually Transmitted Diseases Treatment Guidelines, 2006 (4) regarding the treatment of infections caused by N. gonorrhoeae. On the basis of the most recent evidence, CDC no longer recommends the use of fluoroquinolones for the treatment of gonococcal infections and associated conditions such as pelvic inflammatory disease (PID). Consequently, only one class of drugs, the cephalosporins, is still recommended and available for the treatment of gonorrhea. GISP is a CDC-sponsored sentinel surveillance system that has been monitoring antimicrobial susceptibilities of N. gonorrhoeae in the United States since 1986. Annually, GISP collects approximately 6,000 urethral gonococcal isolates from males attending 26 to 30 sexually transmitted disease (STD) clinics throughout the country and provides national data to guide treatment. QRNG isolates demonstrate ciprofloxacin minimum inhibitory concentrations (MICs) of >1.0 µg/mL; isolates with intermediate resistance to fluoroquinolones demonstrate ciprofloxacin MICs of 0.125--0.500 µg/mL. GISP began susceptibility testing for ciprofloxacin in 1990. Overall, QRNG prevalence remained <1% during 1990--2001 but increased to 2.2% in 2002, to 4.1% in 2003, and to 6.8% in 2004. In 2005, of 6,199 isolates collected by GISP, 9.4% were resistant to ciprofloxacin, and during January--June 2006, 13.3% of 3,005 isolates collected were resistant (Figure) (5). Excluding isolates from Hawaii and California (areas that discontinued fluoroquinolone treatment in 2000 and 2002, respectively), 6.1% and 8.6% of isolates were QRNG in 2005 and 2006, respectively. Intermediate resistance to ciprofloxacin has remained stable, ranging from 0.4% to 1.1% from 1990 to 2006 (5). In addition, since 2001, GISP has observed QRNG increases among isolates from MSM, and more recently, from heterosexual males. In 2001, QRNG prevalence was 1.6% and 0.6% among MSM and heterosexual males, respectively. The QRNG prevalence among isolates from MSM increased to 7.2% in 2002, to 15% in 2003, to 23.8% in 2004, and to 29% in 2005 (5). Among heterosexual males, the prevalence increased more slowly, from 0.9% in 2002 to 1.5% in 2003, to 2.9% in 2004, and to 3.8% in 2005 (5). Preliminary data from January--June 2006 indicate that QRNG prevalence increased to 38.3% among MSM and 6.7% among heterosexual males. For isolates from sites outside of California and Hawaii, QRNG prevalence was 24.3% in MSM and 2.7% in heterosexual males in 2005; in the first 6 months of 2006, it was 30.7% and 5.1%, respectively. Available data from GISP for 2005 and preliminary data from 2006 have demonstrated that QRNG has continued to increase among heterosexual males and is present in all regions of the country (Table) (5). Several cities outside California and Hawaii have seen substantial increases in QRNG prevalence among heterosexual males from 2004 to 2006; for example, in Philadelphia, QRNG prevalence increased from 1.2% in 2004 to 9.9% in 2005 and to 26.6% in 2006, and in Miami, prevalence increased from 2.1% in 2004 to 4.5% in 2005 and to 15.3% in 2006. Reported by: C del Rio, MD, Emory Univ, Atlanta, Georgia. G Hall, PhD, The Cleveland Clinic Foundation, Cleveland, Ohio. EW Hook III, MD, Univ of Alabama at Birmingham, Birmingham, Alabama. KK Holmes, MD, PhD, WLH Whittington, PhD, Univ of Washington, Seattle, Washington. FN Judson, MD, Univ of Colorado Health Sciences Center, Denver, Colorado. EL Yee, MD, AB Harvey, KP Kramer, MPH, DL Trees, PhD, R Ballard, PhD, KA Workowski, MD, LM Newman, MD, S Berman, MD, HS Weinstock, MD, Div of Sexually Transmitted Diseases Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC. Editorial Note:GISP is the only national, sentinel surveillance system that monitors emerging resistance in N. gonorrhoeae in the United States; with the decreasing use of culture to diagnose gonorrhea, GISP has become an increasingly important source of information on N. gonorrhoeae that are resistant to antimicrobials. Findings from GISP, which is conducted in publicly funded clinics and includes only male urethral isolates, might not be representative of the entire U.S. population infected with gonorrhea. During January--June 2006, QRNG was identified in 25 out of 26 GISP sites, and increases in the prevalence of QRNG were observed among isolates from heterosexual males and MSM in most regions of the country. As a result, CDC no longer recommends fluoroquinolones for treatment of gonorrhea in the United States; similarly, CDC no longer recommends fluoroquinolones for treatment of other conditions that might be caused by N. gonorrhoeae, such as PID. CDC has recommended single-dose fluoroquinolone regimens for the treatment of gonococcal infections since 1993. Although QRNG was identified as a problem in Asia in 1991 and was first identified in Hawaii in the same year, only sporadic occurrences were noted in the continental United States during the 1990s. However, since 1999, increasing resistance of N. gonorrhoeae to the fluoroquinolones has been observed, first in Hawaii, then in California and other Western states, then among MSM, and now in other populations and regions. CDC has changed treatment recommendations when QRNG prevalence has reached >5% in defined groups and locations, with consideration given to other factors such as the prevalence of gonorrhea, the availability of antimicrobial susceptibility data, and the costs of diagnostic and treatment options (4,6). This >5% threshold has been used by CDC and the World Health Organization so that all recommended treatments for gonorrhea can be expected to cure >95% of infections. Because fluoroquinolones are no longer recommended, the options for treating gonococcal infections in the United States are limited (4) (Box). For the treatment of uncomplicated urogenital and anorectal gonorrhea, CDC now recommends a single intramuscular dose of ceftriaxone 125 mg or a single oral dose of cefixime 400 mg. However, 400-mg tablets of cefixime are not available; cefixime is only available in a suspension formulation. Some evidence suggests that a single oral dose of cefpodoxime 400 mg or cefuroxime axetil 1 g might be additional oral alternatives for the treatment of urogenital and anorectal gonorrhea (4). Alternative parenteral single-dose regimens for urogenital and anorectal gonorrhea include ceftizoxime 500 mg, cefoxitin 2 g with probenecid 1 g orally, or cefotaxime 500 mg. However, these cephalosporin regimens do not offer any advantage over ceftriaxone. For persons with penicillin or cephalosporin allergies, a single intramuscular dose of spectinomycin 2 g is a recommended alternative. However spectinomycin is not available in the United States. Updated information from CDC regarding the availability of cefixime and spectinomycin will be available at http://www.cdc.gov/std/gonorrhea/arg. For pharyngeal gonorrhea, CDC now recommends a single intramuscular dose of ceftriaxone 125 mg (Box); pharyngeal gonococcal infections often are asymptomatic and more difficult to eradicate than urogenital and anorectal infections (4). Spectinomycin, cefixime, cefpodoxime, and cefuroxime axetil do not appear adequate for treating pharyngeal gonococcal infections. A single oral dose of azithromycin 2 g is effective against uncomplicated gonococcal infections, but CDC does not recommend widespread use of azithromycin because of concerns regarding rapid emergence of resistance, as evidenced by the increase in azithromycin MICs documented since 1999 in the United States and internationally (4,5,7--9). However, azithromycin might be an option for treatment of uncomplicated gonococcal infections from any site (i.e., urogenital, anorectal, and pharyngeal) in persons with documented severe allergic reactions to penicillins or cephalosporins. Persons in whom gonococcal infection is diagnosed should be treated for possible coinfection with Chlamydia trachomatis with a single dose of azithromycin 1 g by mouth or with doxycycline 100 mg twice a day, by mouth for 7 days, if chlamydial infection has not been ruled out (4). Test of cure is not recommended routinely for patients with uncomplicated gonorrhea who have been treated with recommended or alternative regimens. Persons with persistent symptoms of gonococcal infection or whose symptoms recur shortly after treatment with a recommended or alternative regimen should be reevaluated by culture for N. gonorrhoeae; positive isolates should undergo antimicrobial-susceptibility testing. Clinicians and laboratories should report treatment failures or resistant gonococcal isolates to CDC at 404-639-8373 through state and local public health authorities. With fluoroquinolones no longer recommended for the treatment of gonococcal infections, only one class of drug, cephalosporins, is still recommended and available. Therefore, state and local health departments must remain vigilant for the emergence of cephalosporin resistance. With use of nonculture tests to diagnose N. gonorrhoeae increasing and with local data on antimicrobial susceptibility less available, CDC strongly recommends that all state and local health department laboratories maintain or develop the capacity to perform culture (10). CDC also encourages all state and local health department laboratories to maintain the capacity to perform antimicrobial-susceptibility testing or form partnerships with experienced laboratories that can perform such testing. At a minimum, antimicrobial-susceptibility testing should be performed for ceftriaxone, spectinomycin, azithromycin, and any other regimens that are used locally for gonorrhea treatment. Acknowledgments This report is based, in part, on contributions by J Thomas, T Sullivan, Emory Univ, Atlanta, Georgia; LJ Doyle, The Cleveland Clinic Foundation, Cleveland, Ohio; CJ Lenderman, P Dixon, Univ of Alabama at Birmingham, Birmingham, Alabama; K Winterscheid, Univ of Washington, Seattle, Washington; JM Ehret, Univ of Colorado Health Sciences Center, Denver, Colorado; and M Grabenstein, S Bowers, K Pettus, M Parekh, J Knapp, Laboratory Reference and Research Br, Div of Sexually Transmitted Diseases Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 4/12/2007
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|