|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
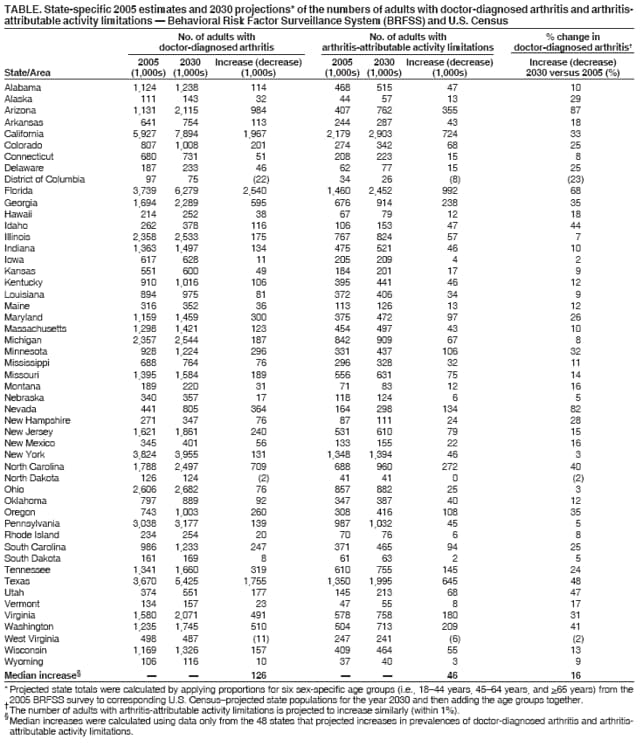
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Projected State-Specific Increases in Self-Reported Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitations --- United States, 2005--2030Please note: An erratum has been published for this article. To view the erratum, please click here. Arthritis and other rheumatic conditions (e.g., gout, lupus, and fibromyalgia) affect approximately 46 million adults in the United States, resulting in substantial disability and costs of $128 billion annually (1--3). Because U.S. adults are living longer and the number of persons in older age groups is growing, the number of U.S. adults living with chronic conditions such as arthritis likely will increase. The number of U.S. adults with doctor-diagnosed arthritis has been projected to reach nearly 67 million adults by the year 2030, including 25 million adults who are expected to have arthritis-attributable activity limitations (4). This report supplements those estimates by projecting the number of adults aged >18 years in each state who will have doctor-diagnosed arthritis and arthritis-attributable activity limitations in 2030.* The results indicate that, among 48 states, the median projected increase in doctor-diagnosed arthritis from 2005 to 2030 will be 16%; a total of 14 states are projected to have increases of 30% to 87%. Greater use of existing evidence-based interventions and development of new interventions aimed at decreasing pain, improving function, and delaying disability associated with arthritis are needed to reduce the impact of these projected increases, particularly in those states that will be most heavily affected. To estimate the number of adults who will have doctor-diagnosed arthritis and arthritis-attributable activity limitations in 2030, CDC applied state arthritis prevalence proportion estimates from the 2005 Behavioral Risk Factor Surveillance System (BRFSS) survey to U.S. Census--projected state population data for the year 2030. BRFSS is a state-based, random-digit--dialed telephone survey of the U.S. civilian, noninstitutionalized population aged >18 years. BRFSS is administered in all 50 states, the District of Columbia, and three U.S. territories (Guam, Puerto Rico, and the U.S. Virgin Islands). In 2005, the median response rate (i.e., the percentage of persons who completed interviews among all eligible persons, including those who were not successfully contacted) among states was 51.1% (range: 34.6% [New Jersey] to 67.4% [Alaska]). The median cooperation rate (i.e., the percentage of persons who completed interviews among all eligible persons contacted) was 75.1% (range: 58.7% [California] to 85.3% [Minnesota]). Self-reported doctor-diagnosed arthritis was defined as a "yes" response to the question, "Have you ever been told by a doctor or other health-care professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?" Arthritis-attributable activity limitations were defined as a "yes" response by a respondent with doctor-diagnosed arthritis to the question, "Are you now limited in any way in any of your usual activities because of your arthritis or joint symptoms?" Projected state totals for doctor-diagnosed arthritis were calculated by applying prevalence proportion estimates for six sex-specific and age-specific (18--44 years, 45--64 years, and >65 years) groups from the 2005 BRFSS survey to corresponding U.S. Census--projected state populations for the year 2030 (6) and then adding the six results. The same method was used to calculate projected state totals for arthritis-attributable activity limitations. Projections were not calculated for the three U.S. territories because U.S. Census--projected territory populations for the year 2030 were not available. From 2005 to 2030, the number of adults with doctor-diagnosed arthritis is projected to increase by a median of 16%† in 48 states (range: 2% [Iowa] to 87% [Arizona]); in 14 states, the projected increase ranges from 30% to 87% (Table). The median projected increase in the absolute number of persons with doctor-diagnosed arthritis in these same states is 126,000 (range: 8,000 [South Dakota] to 2,539,000 [Florida]); the comparable median increase in those with arthritis-attributable activity limitations is 46,000 (range: 3,000 [South Dakota] to 991,000 [Florida]) (Table). Primarily because of expected population declines, two states (North Dakota and West Virginia) and the District of Columbia are projected to have decreases in the numbers of adults with doctor-diagnosed arthritis and arthritis-attributable activity limitations. Reported by: M Freedman, DVM, JM Hootman, PhD, CG Helmick, MD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report confirm previous findings that arthritis and other rheumatic conditions will be increasing in nearly all U.S. states in the years ahead. On the basis of U.S. Census--projected increases in state populations overall and their older age distributions, 48 states are expected to have an increase in the number of adults reporting doctor-diagnosed arthritis and arthritis-attributable activity limitations by the year 2030, including 14 states with increases of >30%. States can use these projections to plan programs and resource allocations that will be needed to address the needs of their growing populations with arthritis. The findings in this report are subject to at least five limitations. First, doctor-diagnosed arthritis is self-reported and not confirmed by a health-care provider; however, such self-reports have been validated previously for surveillance purposes (5). Second, BRFSS is a telephone survey that excludes certain populations (e.g., military personnel residing on bases, institutionalized populations, and persons without landline telephones). Third, the median response rate for BRFSS is low; however, BRFSS data have consistently been determined to provide valid and reliable estimates when compared with national household surveys in the United States (7). Fourth, projections in this report assume consistent age/sex prevalence proportions of doctor-diagnosed arthritis and arthritis-attributable activity limitations to the year 2030; these projections do not take into account emerging health risks (e.g., obesity) that might increase the proportions of doctor-diagnosed arthritis or emerging interventions (e.g., earlier diagnosis of and continued improvements in medications for rheumatoid arthritis) that might decrease the proportions of arthritis-attributable activity limitations. Finally, less than 2% (five of 306) of the sex- and age-specific cells used to calculate the projected prevalence of arthritis-attributable activity limitation in each state had fewer than 50 respondents before weighting and, therefore, might not be reliable estimates. However, any effect on the final state projection likely was overshadowed when the data in these five cells were summed with the other 301 cells. CDC's Arthritis Program funds 36 state health departments, who collaborate with local chapters of the Arthritis Foundation to expand the reach of evidence-based public health interventions for arthritis. These include physical activity programs (Arthritis Foundation Exercise Program, Arthritis Foundation Aquatics Program, and Enhance Fitness) and self-management education programs (Arthritis Foundation Self-Help Program and Chronic Disease Self-Management Program), both of which are delivered by trained instructors in community settings. These interventions decrease the impact of arthritis by reducing pain and health-care utilization and by improving the ability to function and mental health of persons with arthritis (8). In addition, the CDC Arthritis Program also has developed two communication campaigns to promote physical activity among persons with arthritis.§ Healthy People 2010 midcourse review objectives¶ for arthritis include increasing the proportion of adults with doctor-diagnosed arthritis who have had effective, evidence-based arthritis education as an integral part of the management of their condition (objective 2-8). Only 11% of adults with arthritis have taken a class to help manage their arthritis (9). In addition to expanding the reach of arthritis education and other existing interventions, new interventions that specifically target persons with arthritis at highest risk for disability (e.g., persons who are overweight, obese, or physically inactive) also should be developed, evaluated, and disseminated. CDC is funding a project to develop a new arthritis-specific exercise program that emphasizes joint-protection strategies and components designed to improve physical function. The impact of the projected increases in doctor-diagnosed arthritis and arthritis-attributable activity limitations can be reduced by greater participation in such programs and other healthful activities. References
* This report uses the most current surveillance case definition of arthritis, which excludes adults who report only chronic joint symptoms because only a small percentage of these persons have arthritis (5). † The number of adults with arthritis-attributable activity limitations is projected to increase similarly (within 1%). § Available at http://www.cdc.gov/arthritis/campaigns. ¶ Available at http://www.healthypeople.gov/data/midcourse/pdf/fa02.pdf.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 5/2/2007 |
|||||||||
|