|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
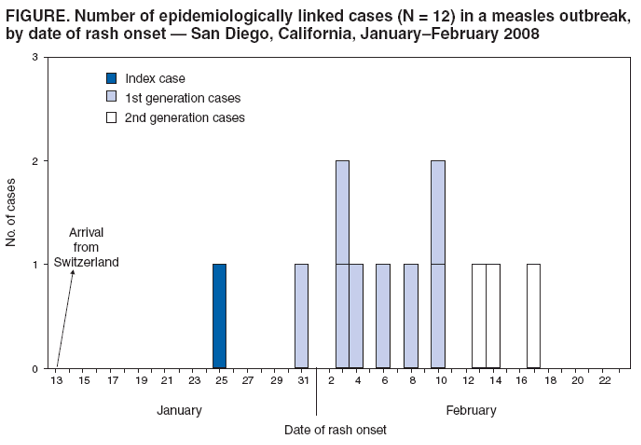
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Measles --- San Diego, California, January--February 2008On February 22, this report was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr). Measles, once a common childhood disease in the United States, can result in severe complications, including encephalitis, pneumonia, and death. Because of successful implementation of measles vaccination programs, endemic measles transmission has been eliminated in the United States and the rest of the Americas. However, measles continues to occur in other regions of the world, including Europe (1). In January 2008, measles was identified in an unvaccinated boy from San Diego, California, who had recently traveled to Europe with his family. After his case was confirmed, an outbreak investigation and response were initiated by local and state health departments in coordination with CDC, using standard measles surveillance case definitions and classifications.* This report summarizes the preliminary results of that investigation, which has identified 11 additional cases of measles in unvaccinated children† in San Diego that are linked epidemiologically to the index case and include two generations of secondary transmission. Recommendations for preventing further measles transmission from importations in this and other U.S. settings include reminding health-care providers to 1) consider a diagnosis of measles in ill persons who have traveled overseas, 2) use appropriate infection-control practices to prevent transmission in health-care settings, and 3) maintain high coverage with measles, mumps, and rubella (MMR) vaccine among children. The index patient was an unvaccinated boy aged 7 years who had visited Switzerland with his family, returning to the United States on January 13, 2008. He had fever and sore throat on January 21, followed by cough, coryza, and conjunctivitis. On January 24, he attended school. On January 25, the date of his rash onset, he visited the offices of his family physician and his pediatrician. A diagnosis of scarlet fever was ruled out on the basis of a negative rapid test for streptococcus. When the boy's condition became worse on January 26, he visited a children's hospital inpatient laboratory, where blood specimens were collected for measles antibody testing; later that day, he was taken to the same hospital's emergency department because of high fever 104°F (40°C) and generalized rash. No isolation precautions were instituted at the doctors' offices or hospital facilities. The boy's measles immunoglobulin M (IgM) positive laboratory test result was reported to the county health department on February 1, 2008. During January 31--February 19, a total of 11 additional measles cases in unvaccinated infants and children aged 10 months--9 years were identified. These 11 cases included both of the index patient's siblings (rash onset: February 3), five children in his school (rash onset: January 31--February 17), and four additional children (rash onset: February 6--10) who had been in the pediatrician's office on January 25 at the same time as the index patient. Among these latter four patients, three were infants aged <12 months. One of the three infants was hospitalized for 2 days for dehydration; another infant traveled by airplane to Hawaii on February 9 while infectious. Two generations of measles cases were identified. The first generation (eight cases) included the index patient's two siblings, two playmates from his school, and the four children from the pediatrician's office. The second generation cases included three children from the index patient's school: a sibling of a child from the first generation and two friends of one of the index patient's siblings (Figure). California allows personal beliefs exemptions (PBEs) to vaccinations required of schoolchildren§; parents can request exemptions if all or some vaccinations are contrary to their beliefs. The index patient and one of his siblings attended a school with 376 children, who ranged in age from 5 to 14 years. Thirty-six (9.6%) of the children had PBEs on file at the school. Among the nine patients aged >12 months, including the index patient, eight were unvaccinated because of PBEs. Among the 36 schoolchildren with PBEs, four had documentation of previous measles vaccination, 11 were vaccinated during the outbreak, and the remaining 21, who did not have evidence of immunity to measles, were placed under voluntary quarantine for 21 days after their last exposure. Overall, approximately 70 children exposed to children with measles in the school, a day care center, the pediatrician's office, and other community settings were placed under voluntary home quarantine because their parents either declined measles vaccination or they were too young to be vaccinated. As part of the public health response in San Diego, surveillance has been enhanced to identify additional rash illnesses, and outbreak response measures in the community are ongoing. In Hawaii, ongoing response measures include following up airplane and other contacts of the infant who traveled to Hawaii to inform them of their potential exposure and refer them to their physicians regarding their susceptibility to measles. Five exposed infants, four airplane contacts, and one personal acquaintance were administered immune globulin within 72 hours of exposure. No secondary cases have been identified in Hawaii to date. Reported by: A Hassidim, K Waters-Montijo, W Wooten, MD, M Sawyer, MD, D Sidelinger, MD, Health and Human Svcs Agency, San Diego; K Harriman, PhD, H Backer, MD, Div of Communicable Disease Control, Center for Infectious Diseases, California Dept of Public Health. P Effler, MD, Michele Nakata, Hawaii State Dept of Health. A Srinivasan, MD, M Bell, MD, Div of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases; P Kutty, MD, S Redd, S Goldstein, MD, J Seward, MBBS, Div of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:Once ubiquitous, measles now is uncommon in the United States. In the prevaccine era, 3 to 4 million measles cases occurred every year, resulting in approximately 450 deaths, 28,000 hospitalizations, and 1,000 children with chronic disabilities from measles encephalitis. Because of successful implementation of measles vaccination programs, fewer than 100 measles cases are now reported annually in the United States and virtually all of those are linked to imported cases (2,3), reflecting the incidence of measles globally and travel patterns of U.S. residents and visitors. During 2006--2007, importations were most common from India, Japan, and countries in Europe, where measles transmission remains endemic and large outbreaks have occurred in recent years (CDC, unpublished data, 2008). Since November 2006, Switzerland has experienced that country's largest measles outbreak since introduction of mandatory notification for measles in 1999 (1). The San Diego import-associated outbreak, affecting exclusively an unvaccinated population and infants too young to be vaccinated, serves as a reminder that unvaccinated persons remain at risk for measles and that measles spreads rapidly in susceptible subgroups of the population unless effective outbreak-control strategies are implemented. Although notable progress has been made globally in measles control and elimination, measles still occurs throughout the world. U.S. travelers can be exposed to measles almost anywhere they travel, including to developed countries. To prevent acquiring measles during travel, U.S. residents aged >6 months traveling overseas should have documentation of measles immunity before travel (4). Travel histories should be obtained and a diagnosis of measles should be considered by physicians evaluating patients who have febrile rash illness within 3 weeks of traveling abroad. Measles virus is highly infectious; vaccination coverage levels of >90% are needed to interrupt transmission and maintain elimination in populations. The ongoing outbreak in Switzerland, which has resulted in hospitalizations for pneumonia and encephalitis, has occurred in the context of vaccination coverage levels of 86% for 1 dose at age 2 years and 70% for the second dose for children aged <12 years. In the United States, vaccination coverage levels for at least 1 dose of MMR vaccine have been >90% among children aged 19--35 months and >95% among school-aged children during this decade. Although not measured routinely, 2-dose vaccine coverage is extremely high among U.S. schoolchildren because of school vaccination requirements. Measles transmission in schools was common in the era before interruption of endemic-disease transmission, and school requirements for vaccination have been a successful strategy for achieving high vaccination coverage levels in this age group and decreasing transmission in school settings. In the United States, all states require children to be vaccinated in accordance with Advisory Committee on Immunization Practices recommendations before attending school (4). However, medical exemptions to immunization requirements for day care and school attendance are available in all states; in addition, 48 states offer nonmedical religious exemptions, and 21 states (including California) offer nonmedical PBEs.¶ These exemptions are defined differently by each state. The PBE allowed by California requires only a parental affidavit (5). Compared with vaccinated persons, those exempt from vaccination are 22 to 224 times more likely to contract measles (5--7). The community transmission that has occurred during the San Diego outbreak is consistent with previous observations that the frequency of vaccination exemptors in a community is associated with the incidence of measles in that community; in addition, imported measles cases have demonstrated the potential for sizeable outbreaks in U.S. communities with suboptimal vaccine coverage (5,6,8). The public health response to this outbreak has included identification of cases, isolation of patients and vaccination, administration of immune globulin, and voluntary quarantine of contacts who have no evidence of measles immunity. Costs associated with control of these outbreaks can be substantial. In Iowa, the public health response to one imported measles case cost approximately $150,000 (9). This outbreak also illustrates the risk for measles transmission in health-care settings. Airborne transmission of measles has been reported in emergency departments, physician offices, and pediatric ambulatory care-settings (10). Persons exposed to measles should be instructed to inform all health-care providers of their exposure before entering a health-care facility. Health-care personnel providing care to suspected measles patients (i.e., patients with febrile illness and generalized maculopapular rash or known contacts with prodromal symptoms) should apply appropriate isolation practices, including airborne precautions, in addition to taking standard precautions for such patients.** Once a suspected measles case has been identified, prompt isolation of the potentially infectious patient and implementation of appropriate infection-control measures can help to decrease risk for transmission. Patients with suspected measles should be placed in an examination room, preferably an airborne-infection isolation room, as soon as possible and should not be permitted in patient waiting areas. Until placed in an airborne-infection isolation room, the patient should wear a surgical mask. If a surgical mask cannot be tolerated, other practical means to contain respiratory aerosols should be implemented. The door to the examination room should be kept closed, and all health-care personnel in contact with the patient should be documented as immune to measles. Health-care personnel and visitors without evidence of immunity (i.e., documentation of adequate vaccination, laboratory evidence of immunity, born before 1957, or documentation of physician-diagnosed measles) should be restricted from entering the rooms of patients known or suspected to have measles (4,10). The examination room should not be used for 2 hours after the infectious patient leaves. Suspected measles patients should not be referred to other locations for laboratory tests unless infection-control measures can be implemented at those locations. Measles morbidity and mortality can be reduced through vaccination with MMR vaccine. Vaccination of U.S. travelers can reduce measles importations. Sustained high population immunity through vaccination, effective surveillance, and robust public health preparedness and response capacity are needed to keep the United States free from indigenous measles transmission and control any outbreaks associated with importations. References
* Available at http://www.cdc.gov/ncphi/disss/nndss/casedef/measles_current.htm. † One case was identified in a girl aged 2 years whose vaccination was delayed. The girl had received a dose of single antigen measles vaccine routinely. However, investigators later determined that she had been exposed to measles 6 days before vaccination. Because postexposure vaccination is only considered effective if administered within 3 days of exposure and because immunity takes several weeks to develop, investigators considered the girl unvaccinated. § Information available at http://www.dhs.ca.gov/ps/dcdc/izgroup/pdf/imm488e.pdf. ¶ Institute for Vaccine Safety. Vaccine exemptions. Baltimore MD: Johns Hopkins Bloomberg School Public Health. Available at http://www.vaccinesafety.edu/cc-exem.htm. ** Available at http://www.cdc.gov/ncidod/dhqp/gl_isolation.html.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 2/27/2008 |
|||||||||
|