Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Increasing Physical Activity
A Report on Recommendations of the Task Force
on Community Preventive Services
Task Force on Community Preventive Services*
October 1, 2001
CHAIR
Jonathan E. Fielding, M.D., M.P.H., M.B.A.
Los Angeles Department of Health Services
Los Angeles, California
VICE-CHAIR
Patricia Dolan Mullen, Dr.P.H.
University of Texas-Houston
School of Public Health
Houston, Texas
MEMBERS
Ross C. Brownson, Ph.D.
St. Louis University School of Public Health
St. Louis, Missouri
Mindy Thompson Fullilove, M.D.
New York State Psychiatric Institute and Columbia University
New York, New York
Fernando A. Guerra, M.D., M.P.H.
San Antonio Metropolitan Health District
San Antonio, Texas
Alan R. Hinman, M.D., M.P.H.
Task Force for Child Survival
and Development
Atlanta, Georgia
George J. Isham, M.D.
HealthPartners
Minneapolis, Minnesota
Garland H. Land, M.P.H.
Center for Health Information Management and Epidemiology
Missouri Department of Health
Jefferson City, Missouri
Charles S. Mahan, M.D.
College of Public Health
University of South Florida
Tampa, Florida
Patricia A. Nolan, M.D., M.P.H.
Rhode Island Department of Health
Providence, Rhode Island
Susan C. Scrimshaw, Ph.D.
School of Public Health
University of Illinois
Chicago, Illinois
Steven M. Teutsch, M.D., M.P.H.
Merck & Company, Inc.
West Point, Pennsylvania
Robert S. Thompson, M.D.
Department of Preventive Care
Group Health Cooperative of Puget Sound
Seattle, Washington
CONSULTANTS
Robert S. Lawrence, M.D.
Bloomberg School of Public Health
Johns Hopkins University
Baltimore, Maryland
J. Michael McGinnis, M.D.
Robert Wood Johnson Foundation
Princeton, New Jersey
Lloyd F. Novick, M.D., M.P.H.
Onondaga County Department of Health
Syracuse, New York
*Patricia A. Buffler, Ph.D., M.P.H., University of California, Berkeley; Mary
Jane England, M.D., Regis College, Weston, Massachusetts; Caswell A. Evans,
D.D.S., M.P.H., Office of the U.S. Surgeon General, Rockville, Maryland; and
David W. Fleming, M.D., CDC, Atlanta, Georgia, also served on the Task Force
while the recommendations were being developed.
The following CDC staff members prepared this report:
Emily B. Kahn, Ph.D., M.P.H.
Leigh Taylor Ramsey, Ph.D.
Division of Prevention Research and Analytic Methods
Epidemiology Program Office
Gregory W. Heath, D.H.Sc., M.P.H.
Elizabeth H. Howze, Sc.D.
Division of Nutrition and Physical Activity
National Center for Chronic Disease Prevention and Health Promotion
in collaboration with
Kenneth E. Powell, M.D., M.P.H.
Georgia Department of Human Resources
Atlanta, Georgia
Elaine J. Stone, Ph.D., M.P.H.
National Heart, Lung, and Blood Institute
National Institutes of Health
Bethesda, Maryland
Ross C. Brownson, Ph.D.
Task Force on Community Preventive Services and
St. Louis University School of Public Health
St. Louis, Missouri
Summary
The Task Force on Community Preventive Services (the Task Force) has
conducted systematic reviews of community interventions to increase physical activity.
The Task Force either strongly recommends or recommends six interventions:
two informational approaches (i.e., communitywide campaigns and
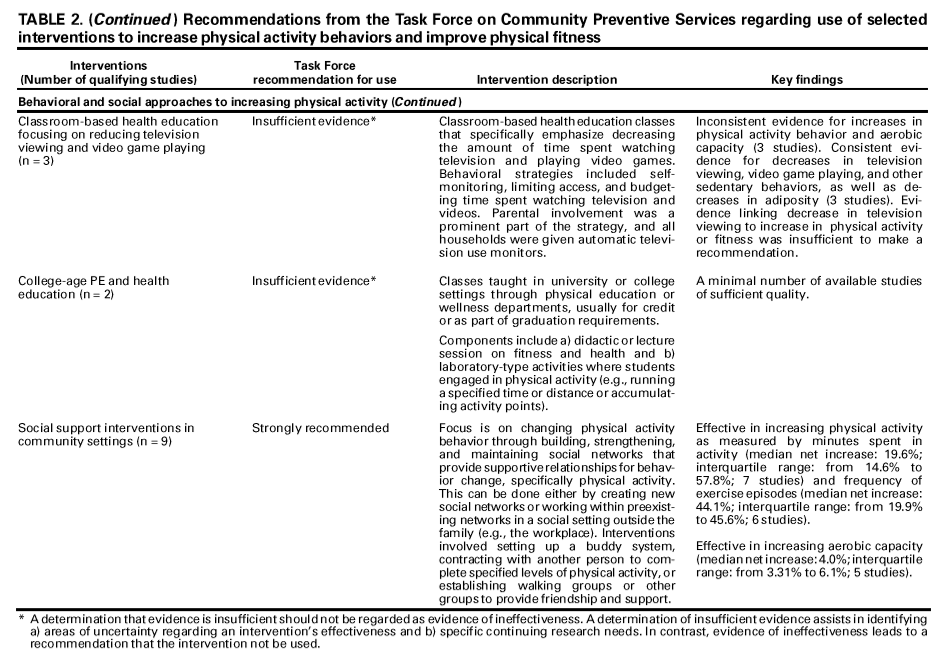
point-of-decision prompts to encourage use of stairs); three behavioral and social approaches
(i.e., school-based physical education, social support interventions in community
settings [e.g., setting up a buddy system or contracting with another person to
complete specified levels of physical activity], and individually adapted health
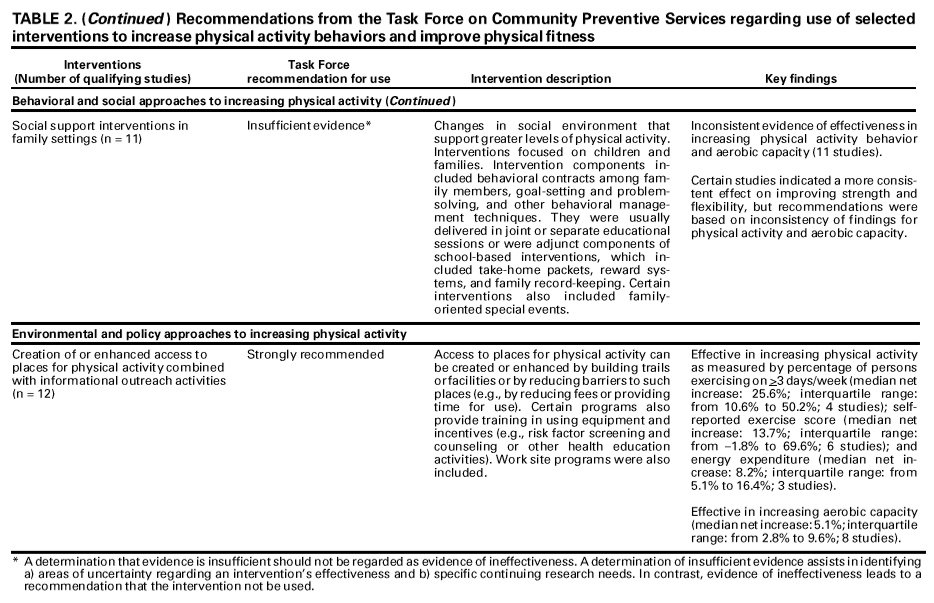
behavior change programs); and one intervention to increase physical activity by
using environmental and policy approaches (i.e., creation of or enhanced access to
places for physical activity, combined with informational outreach activities). The
Task Force found insufficient evidence on which to base recommendations
for classroom-based health education focused on information provision,
behavioral skills, and social support interventions in family settings because of
inconsistent findings; mass media campaigns, college-age physical education, and
health education because of an insufficient number of studies; and classroom-based
health education focusing on reducing television viewing and video game playing
because of the lack of a demonstrated link between reduced time spent watching
television or playing video games and increased physical activity. This report
provides additional information regarding the recommendations, briefly describes how
the reviews were conducted, and provides information that can help in applying
the interventions locally.
BACKGROUND
Regular physical activity is associated with enhanced health and reduced risk for
all-cause mortality (1--4). Beyond the effects on mortality, physical activity has
multiple health benefits, including reducing the risk for cardiovascular disease,
diabetes, obesity, selected cancers, and musculoskeletal conditions
(5). Even with all the known benefits of regular physical activity, only 25% of adults in the United
States report engaging in recommended physical activity levels (i.e., either 30 minutes
of moderate-intensity activity on >5 days/week or 20 minutes of
vigorous-intensity physical activity on
>3 days/week); 29% report no leisure-time regular
physical activity (6); and only 27% of students in grades 9--12 engage in
moderate-intensity physical activity (7).
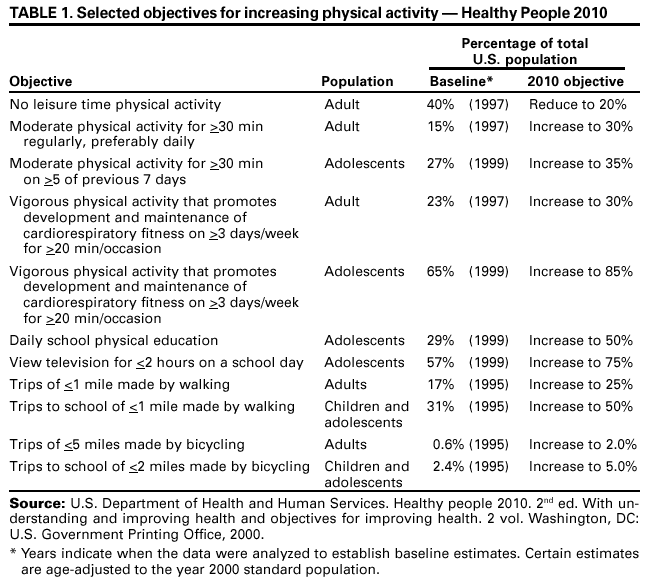
In the Healthy People 2010 national health objectives
(7), physical activity is listed as a leading health indicator. Goals have been developed to improve levels of
physical activity among adults, adolescents, and children and to reduce sedentary
behavior among adolescents (Table 1). By implementing interventions demonstrated to
be effective in increasing physical activity, policy makers and public health providers
can help their communities achieve these goals while using community
resources efficiently. This report and other related publications provide guidance from the
Task Force on Community Preventive Services (the Task Force) to personnel in state
and local health departments, education agencies, universities, community
coalitions,
organizations that fund public health programs, health-care systems, and others
who have interest in or responsibility for increasing physical activity.
INTRODUCTION
This report is one in a series of topics included in the
Guide to Community Preventive Services: Systematic Reviews and Evidence-Based
Recommendations (the Community Guide), a resource that will include multiple systematic reviews,
each focusing on a preventive health topic. This report provides an overview of
the process used by the Task Force to select and review evidence and summarize
its recommendations concerning interventions to increase physical activity. A full
report of the recommendations, additional evidence (i.e., discussions of
applicability, additional benefits, potential harms, and existing barriers to implementation),
costs, cost-benefits, and cost-effectiveness of the interventions (when available),
and remaining research questions is planned for publication in the
American Journal of Preventive Medicine in 2002.
The independent, nonfederal Task Force is developing the
Community Guide with the support of the U.S. Department of Health and Human Services (DHHS)
in collaboration with public and private partners. Although CDC provides staff
support to the Task Force for development of the
Community Guide, recommendations presented in this report were developed by the Task Force and are not necessarily
the recommendations of CDC or DHHS.
METHODS
The Community Guide's methods for conducting systematic reviews and
linking evidence to recommendations have been described elsewhere
(8). In brief, for each Community
Guide topic, a multidisciplinary team conducts a review by
developing an approach to organizing, grouping, and selecting interventions;
systematically searching for and retrieving evidence;
assessing the quality of and summarizing the strength of the body of
evidence of effectiveness;
summarizing information regarding other evidence; and
identifying and summarizing research gaps.
For physical activity, the development team focused on interventions to
increase physical activity through informational, behavioral and social, and
environmental and policy approaches.
The coordination and consultation teams* generated a comprehensive list
of interventions. From this, a priority list of interventions for review was developed
on the basis of a process of polling the coordination team, consultation team, and
other physical activity specialists. Factors for consideration included their perception of
the public health consequences (i.e., number of persons affected), the practicality
of application, and the need of those promoting physical activity for
information regarding each intervention. Time and resource constraints precluded review
of certain interventions (e.g., interventions oriented toward health-care providers
or structured exercise classes that were not part of multicomponent
community-based interventions).
Interventions reviewed were either single-component (i.e., using only one element
to achieve desired outcomes) or multicomponent (i.e., using more than one
element). Studies were grouped on the basis of similarity of the intervention being
evaluated. Certain studies provided evidence for
>2 interventions. In these cases, the
studies
were reviewed for each applicable intervention. Studies and outcome measures
were classified according to definitions developed as part of the review process.
The nomenclature used in this review might differ from that used in the original studies.
To be included in the reviews of effectiveness, studies had to a) be
primary investigations of interventions selected for evaluation rather than, for
example, guidelines or reviews; b) be published in English during 1980--2000; c) be
conducted in established market economies;** and d) compare outcomes among groups
of persons exposed to the intervention with outcomes among groups of persons
not exposed or less exposed to the intervention, whether the study design included
a concurrent or before-and-after comparison.
Searches of seven computerized databases (i.e.,
MEDLINE,® SPORTDiscus, PsychInfo, TRIS Online [Transportation Research Information Services],
Enviroline,® Sociological Abstracts, and Social
SciSearch®) were conducted. Team members also
reviewed reference lists and consulted with other physical activity specialists to
identify relevant studies.
For each intervention reviewed, the team developed an analytic framework
indicating possible causal links between the intervention under study and predefined
outcomes of interest. To make its recommendations, the Task Force required that
studies demonstrate improvements in physical activity behavior outcomes (e.g.,
increased time spent walking) or increases in selected fitness measures (e.g., increased
aerobic capacity). These outcomes were selected because they are linked to improved
health outcomes, including those that document the following principles:
Regular physical activity or improved cardiovascular fitness reduces the risk
of all-cause mortality (1--4) and increases years of healthy life.
Physical activity or improved cardiovascular fitness reduces risk for
morbidity resulting from cardiovascular and other chronic diseases
(9).
Physical activity does not need to be vigorous and sustained to achieve
health benefits. Improved health can be attained through the accumulation of shorter
bouts of moderate-intensity activity (9); however, greater levels of activity do
produce greater health benefits.
Changes in physical activity behavior precede changes in fitness levels and
can be more evident with short-term interventions; thus, behavior changes are
an appropriate outcome.
Each included study was evaluated by using a standardized abstraction form
and assessed for suitability of the study design and threats to validity
(10). Studies were characterized as having good, fair, or limited execution on the basis of the number
of threats to validity identified (8). Results for each outcome of interest were
obtained from each study that met the minimum quality criteria. Net effects were
derived when possible by calculating the difference between the changes observed in
the intervention and comparison groups relative to the respective baseline
levels.*** The median was used to summarize a typical measure of effect across the body
of evidence for each outcome of interest. For bodies of evidence consisting of
>4 studies, an interquartile range is used to represent variability; otherwise, a
simple range is reported. The strength of the body of evidence of effectiveness
was characterized as strong, sufficient, or insufficient on the basis of the number
of available studies, the suitability of study designs for evaluating effectiveness,
the
quality of execution of the studies as defined by the
Community Guide (8), the consistency of the results, and the effect size.
The Community Guide uses systematic reviews to evaluate the evidence
of intervention effectiveness, and the Task Force makes recommendations on the
basis of the findings of those reviews (8). The strength of each recommendation is
based on the evidence of effectiveness (e.g., an intervention is strongly
recommended when strong evidence of effectiveness exists and recommended when
sufficient evidence exists) (8). Other types of evidence can also affect a recommendation.
For example, harms resulting from an intervention that outweigh benefits might lead to
a recommendation that the intervention not be used even if it is effective in
improving certain outcomes. Although the option exists, the Task Force has yet to use
economic information to modify recommendations.
A finding of insufficient evidence of effectiveness should not be regarded as
evidence of ineffectiveness. Insufficient evidence might be determined for any one of
multiple reasons, alone or in combination, including an insufficient number of studies;
the available studies had too many threats to validity because of their design,
execution, or both; or the results of the studies conflict in a way that precludes a
coherent summary of effectiveness. In all of those situations, a finding of insufficient
evidence is key to identifying areas of uncertainty and continuing research needs. In
contrast, sufficient or strong evidence of ineffectiveness would lead to a recommendation
that the intervention not be used.
RESULTS
Database searches and bibliographic reviews yielded 6,238 potentially relevant
titles. After a review of the abstracts and consultation with physical activity specialists,
849 reports were retrieved. Of these, 253 were retained for full review. On the basis
of limitations in execution or design or because they provided no additional
information regarding studies that were already included, 159 of these were excluded and
were not considered further. The remaining 94 studies were considered qualifying
studies. The 11 Task Force recommendations in this report are based on the
systematic review and evaluation of these qualifying studies, all of which had good or
fair quality of execution.
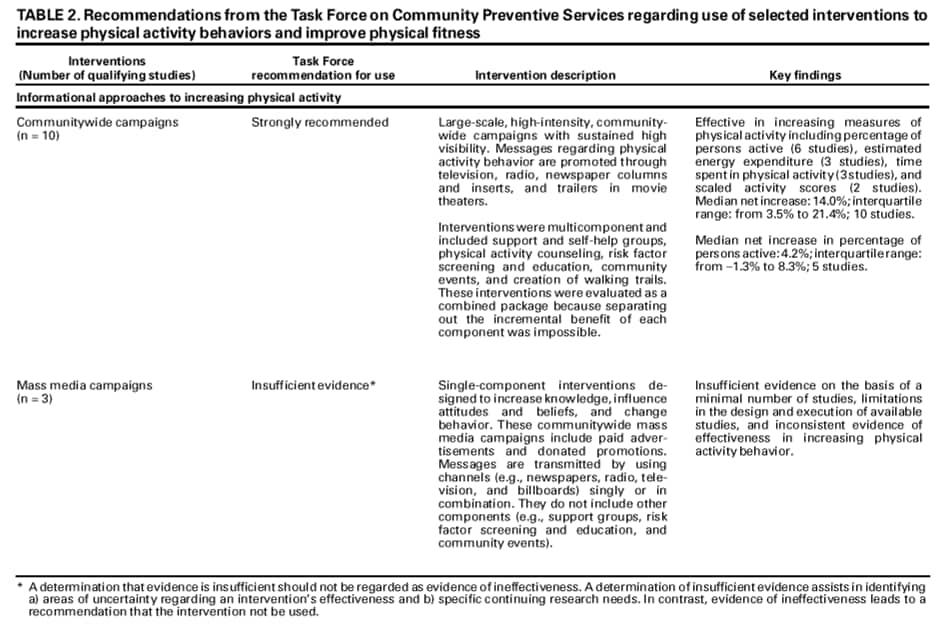
The Task Force strongly recommended or recommended six interventions (Table 2), as follows:
two informational approaches,
communitywide campaigns and
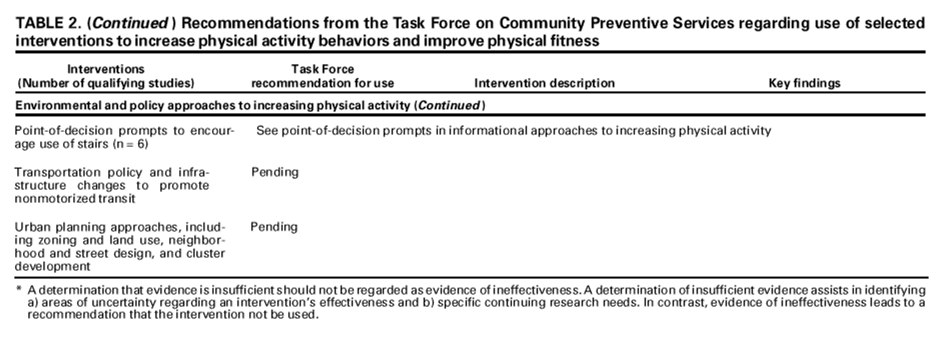
point-of-decision prompts to encourage using stairs;
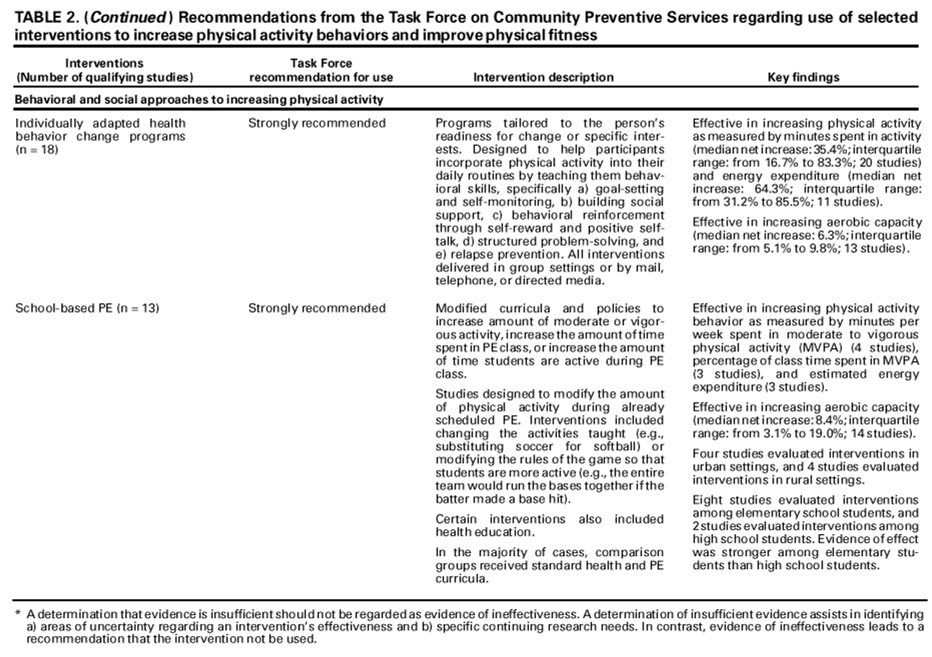
three behavioral and social approaches,
school-based physical education,
social support interventions in community settings (e.g., setting up a
buddy system or contracting with another person to complete specified limits of
physical activity), and
individually adapted health behavior change; and
one environmental and policy approach,
creation of or enhanced access to places for physical activity combined
with informational outreach activities.
The Task Force determined that evidence was insufficient to make
recommendations for or against the following interventions for the reasons provided:
classroom-based health education focusing on information
provision, behavioral skills, and social support interventions in family settings because
of inconsistent effect on physical activity behavior, aerobic fitness, or both;
mass media campaigns, college-age physical education, and health
education because of an insufficient number of studies; and
classroom-based health education focusing on reducing television viewing
and video game playing because of the lack of a demonstrated link between
reduced time spent watching television or playing video games and increased
physical activity.
In addition to these 11 interventions, reviews for 2 additional interventions
to increase physical activity by using environmental and policy approaches
(i.e., transportation policies and infrastructure changes to promote nonmotorized
transit and urban planning approaches [e.g., zoning and land use]) are under way and
will be included in a subsequent report. Summary tables of the reviews of
economic evidence are available at <http://www.thecommunityguide.org> (accessed August
13, 2001).
USING THE RECOMMENDATIONS IN COMMUNITIES
Physical inactivity and dietary patterns are second only to tobacco use as a
leading cause of preventable death in the United States
(11). Physical inactivity is also a leading contributor to morbidity and disability. In the United States, the majority
of persons do not achieve the recommended amounts of physical activity.
Communities can help increase levels of physical activity among persons of all ages and
thereby address this serious public health problem. The Task Force recommendations are
a compendium of tested interventions that promote physical activity at the
community level. They can be used for planning interventions to promote physical activity or
to evaluate existing programs.
The Task Force recommendations can be used to support
communitywide campaigns, point-of-decision prompts to encourage using stairs,
school-based physical education, social support interventions in community settings,
individually adapted health behavior change, and creation of or enhanced access to places
for physical activity combined with informational outreach activities.
Certain recommendations are multicomponent and involve different types of
interventions. For example, communitywide campaigns usually involve a combination of
mass media messages and other strategies, including community health fairs, work
site risk factor screenings, and group educational sessions. Creating or enhancing
access to places for physical activity (e.g., biking or walking trails) is also
strongly recommended. In selecting and implementing interventions, communities
are encouraged to develop comprehensive programs that include activities suitable
for their local resources, population characteristics, and settings.
Choosing interventions that are well-matched to local needs and capabilities,
and then carefully implementing those interventions, are vital steps for
increasing physical activity. In setting priorities for selecting interventions to meet
local objectives, recommendations and other evidence provided in the
Community Guide should be considered in combination with local information, including
resource availability, administrative structures, and economic and social environments
of organizations and practitioners.
Information regarding applicability can be used to assess the extent to which
the intervention might be useful in a particular setting or for a population.
Although sparse, economic information, to be provided in the full report in 2002, might
be useful in identifying intervention resource requirements and interventions that
meet public health goals more efficiently than other available options. After
considering local goals and resources, using strongly recommended or
recommended interventions should be given implementation priority.
Certain recommended or strongly recommended interventions had minimal
to moderate (although consistent) behavior change scores. Readers should
remember that the interventions were targeted at groups of persons rather than single
persons. Because the largest public health benefit in physical activity interventions
comes from having populations of sedentary persons become more active rather
than already active persons becoming more active, the interventions, if
widely implemented, could create substantial public health benefits.
ADDITIONAL INFORMATION REGARDING THE
COMMUNITY GUIDE
Community Guide topics are prepared and released as each is completed.
The findings from systematic reviews concerning vaccine-preventable diseases,
tobacco use prevention and reduction, motor-vehicle occupant injury, and diabetes
have already been published. A compilation of systematic reviews will be published
in book form. Additional information regarding the Task Force, the
Community Guide, and a list of published articles is available on the Internet at
<http://www.thecommunityguide.org> (accessed August 13, 2001).
References
Lee IM, Hsieh CC, Paffenbarger RS Jr. Exercise intensity and longevity in men: the
Harvard Alumni Health Study. JAMA 1995;273:1179--84.
Paffenbarger RS Jr, Hyde RT, Wing AL, Lee IM, Jung DL, Kampert JB. Association of
changes in physical-activity level and other lifestyle characteristics with mortality among men.
N Engl J Med 1993;328:538--45.
Paffenbarger RS Jr, Kampert JB, Lee IM, Hyde RT, Leung RW, Wing AL. Changes in
physical activity and other lifeway patterns influencing longevity. Med Sci Sports Exerc 1994;26:857--65.
Blair SN, Kohl HW 3rd, Barlow CE, Paffenbarger RS Jr, Gibbons LW, Macera CA. Changes
in physical fitness and all-cause mortality: a prospective study of healthy and unhealthy
men. JAMA 1995;273:1093--8.
Bouchard C, Shephard RJ, Stevens T, eds. Physical activity, fitness, and health:
international proceedings and consensus statement. In: Proceedings of the 1992 International
Conference on Physical Activity, Fitness, and Health. Champaign, IL: Human Kinetics Publisher, 1994.
US Department of Health and Human Services. Healthy people 2010 (conference ed in
2 vols) Washington, DC: US Department of Health and Human Services, 2000.
Briss PA, Zaza S, Pappaioanou M, et al., and the Task Force on Community Preventive
Services. Developing an evidence-based Guide to Community Preventive
Services---methods. Am J Prev Med 2000;18(1 Suppl):35--43.
US Department of Health and Human Services. Physical activity and health: a report of
the Surgeon General. Atlanta, GA: US Department of Health and Human Services, CDC,
National Center for Chronic Disease Prevention and Health Promotion, 1996.
Zaza S, Wright-De Agüero LK, Briss PA, et al. and the Task Force on Community
Preventive Services. Data collection instrument and procedure for systematic reviews in the
Guide to Community Preventive Services. Am J Prev Med 2000;18(1 Suppl):44--74.
McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA 1993;270:2207--12.
* Members of the consultation team were Terry Bazzarre, Ph.D., Robert Wood Johnson
Foundation, Princeton, New Jersey; Carl J. Caspersen, Ph.D., CDC, Atlanta, Georgia; Diana Cassady,
Dr.P.H., California Department of Health Services, Sacramento, California; Carlos J. Crespo,
Dr.P.H., State University of New York School of Medicine and Biomedical Sciences, Buffalo, New
York; Steve Hooker, Ph.D., California Department of Health Services, Sacramento, California;
Jonathan Fielding, M.D., M.P.H., M.B.A., University of California at Los Angeles School of Public
Health, Los Angeles, California; Barbara Fraser, M.S., Nebraska Department of Health and
Human Services, Lincoln, Nebraska; George J. Isham, M.D., HealthPartners, Bloomington,
Minnesota; Delle B. Kelley, CDC, Atlanta, Georgia; Abby C. King, Ph.D., Stanford University School
of Medicine, Stanford, California; I-Min Lee, M.D., Sc.D., Harvard Medical School/Brigham
and Women's Hospital, Boston, Massachusetts; Denise G. Simons-Morton, M.D., Ph.D.,
National Institutes of Health, Bethesda, Maryland; Reba A. Norman, M.L.M., CDC, Atlanta, Georgia;
Cindy Porteous, M.A., Indianapolis Park Foundation, Indianapolis, Indiana; Michael Pratt, M.D.,
M.P.H., CDC, Atlanta, Georgia; Thomas Schmid, Ph.D., CDC, Atlanta, Georgia; Christine G. Spain,
M.A., the President's Council on Physical Fitness and Sports, Washington D.C.; Wendell C.
Taylor, Ph.D., M.P.H., University of Texas Health Science Center at Houston, Houston, Texas.
** Established market economies as defined by the World Bank are Andorra, Australia,
Austria, Belgium, Bermuda, Canada, Channel Islands, Denmark, Faeroe Islands, Finland, France,
Former Federal Republic of Germany, Germany, Gibraltar, Greece, Greenland, Holy See, Iceland,
Ireland, Isle of Man, Italy, Japan, Liechtenstein, Luxembourg, Monaco, the Netherlands, New
Zealand, Norway, Portugal, San Marino, Spain, St. Pierre and Miquelon, Sweden, Switzerland, the
United Kingdom, and the United States.
*** When information for both intervention (I) and control groups (C) was provided
for times before and after the intervention, net intervention effect was calculated as
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].