Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Diagnosis and Management of Tickborne Rickettsial
Diseases: Rocky Mountain Spotted Fever, Ehrlichioses, and Anaplasmosis
--- United States
A Practical Guide for Physicians and Other Health-Care and Public
Health Professionals
Prepared by
Alice S. Chapman, DVM1
in collaboration with the
Tickborne Rickettsial Diseases Working Group Johan S. Bakken, MD, PhD2 Scott M. Folk,
MD6 Christopher D. Paddock, MD1 Karen C. Bloch, MD3 Allan Krusell,
MD7 Daniel J. Sexton,
MD10
Steven C. Buckingham, MD4 Gary S. Marshall,
MD8 Gregory A. Storch, MD11 Gregory A. Dasch, PhD1 Jennifer H. McQuiston,
DVM1 David L. Swerdlow,
MD1
J. Stephen Dumler, MD5 William L. Nicholson,
PhD1 David H. Walker, MD12 Marina E. Eremeeva, MD, PhD, ScD1 Christopher A. Ohl,
MD9
1National Center for Infectious Diseases, CDC;
2St. Luke's Infectious Disease Associates, Duluth, Minnesota;
3Vanderbilt University Medical School, Nashville, Tennessee;
4University of Tennessee Health Science Center, Memphis, Tennessee;
5Johns Hopkins Medical Institutions, Baltimore, Maryland;
6Heartland Regional Medical Center, St. Joseph, Missouri;
7Northeast Medical Center, Concord, North Carolina;
8University of Louisville Medical School, Louisville, Kentucky;
9Wake Forest University Medical School, Winston-Salem, North
Carolina; 10Duke University Medical School, Durham, North Carolina;
11Washington University Medical School, St. Louis, Missouri;
12University of Texas Medical Branch, Galveston, Texas
The material in this report originated in the National Center for Infectious Diseases, Rima Khabbaz, MD, Director; and the Division of Viral
and Rickettsial Diseases, Steve Monroe, PhD, Acting Director.
Corresponding preparer: David L. Swerdlow, MD, Division of Viral and Rickettsial Diseases, National Center for Infectious Diseases, 1600
Clifton Rd., NE, MS G-13, Atlanta, GA 30333. Telephone: 404-639-1329; Fax: 404-639-4436; E-mail: [email protected].
Summary
Tickborne rickettsial diseases (TBRD) continue to cause severe illness and death in otherwise healthy adults
and children, despite the availability of low cost, effective antimicrobial therapy. The greatest challenge to clinicians is
the difficult diagnostic dilemma posed by these infections early in their clinical course, when antibiotic therapy is most
effective. Early signs and symptoms of these illnesses are notoriously nonspecific or mimic benign viral illnesses, making
diagnosis difficult. In October 2004, CDC's Viral and Rickettsial Zoonoses Branch, in consultation with 11 clinical and
academic specialists of Rocky Mountain spotted fever, human granulocytotropic anaplasmosis, and human
monocytotropic ehrlichiosis, developed guidelines to address the need for a consolidated source for the diagnosis and management of
TBRD. The preparers focused on the practical aspects of epidemiology, clinical assessment, treatment, and laboratory diagnosis
of TBRD. This report will assist clinicians and other health-care and public health professionals to 1)
recognize epidemiologic features and clinical manifestations of TBRD, 2) develop a differential diagnosis that includes and
ranks TBRD, 3) understand that the recommendations for doxycycline are the treatment of choice for both adults and
children, 4) understand that early empiric antibiotic therapy can prevent severe morbidity and death, and
5) report suspect or confirmed cases of TBRD to local public health authorities to assist them with control measures and public
health education efforts.
Introduction
Tickborne rickettsial diseases (TBRD) are clinically similar, yet epidemiologically and etiologically distinct illnesses.
In the United States, these diseases include 1) Rocky Mountain spotted fever (RMSF), 2) human monocytotropic
(or monocytic) ehrlichiosis (HME), 3) human
granulocytotropic (or granulocytic) anaplasmosis (HGA, formerly known
as human granulocytotropic ehrlichiosis or HGE)
(1), 4) Ehrlichia ewingii infection, and 5) other emerging TBRD.
The reported incidence of these diseases has increased during the previous decade. Despite the availability of low-cost
and effective antibiotic therapy, which may be used empirically for suspected cases, TBRD continue to cause severe
illness and death in otherwise healthy adults and children. The greatest challenge to clinicians is diagnosing these
infections early in their clinical course, when antibiotic therapy is most effective
(2,3). The majority of patients with TBRD
seek medical care within 2--4 days of onset of illness
(4--7). In general, these patients are first evaluated by
family practitioners, pediatricians, internists, emergency department (ED) physicians, or physician
extenders. Early signs and symptoms of these illnesses are notoriously nonspecific, or they might mimic benign viral illnesses, making
diagnosis difficult. For example, even in areas where awareness of RMSF is high, approximately 60%--75% of
patients with this TBRD receive an alternate diagnosis on their first visit for medical care
(8,9). Moreover, the earlier patients seek care
in the course of their illness, the more likely an alternate diagnosis will be made
(4). The lack of a specific initial
syndrome, however, does not imply that the course of these diseases will be benign.
In October 2004, to address the need for a consolidated resource for the diagnosis and management of TBRD,
CDC's Viral and Rickettsial Zoonoses Branch collaborated with 11 clinical and academic specialists of RMSF, HGA, and
HME. These external contributors were invited by CDC subject matter specialists to participate among clinicians
and researchers in the field of TBRD, based on direct working interactions related to case consultation and
recognized expertise from peer-reviewed publications. In December 2004, the framework of this report was developed by
CDC's Viral and Rickettsial Zoonoses Branch, based on a summary of the peer-reviewed published reports on the
epidemiology and clinical aspects of TBRD. External contributors further developed recommendations for the diagnosis and
treatment of TBRD based on their clinical research and experience. All work group collaborators reviewed and provided input
and approved the final content of this report.
The primary goal of this report is to provide primary care physicians and physician extenders with
practical information to assist with the diagnosis and care of
patients with TBRD. This report provides a framework
for recognizing suggestive symptoms, considering likely alternative diagnoses, eliciting relevant history,
requesting appropriate diagnostic tests, and initiating prompt, effective treatment. Information in this guide is designed to
assist clinicians to
recognize common epidemiologic situations and clinical manifestations of TBRD;
obtain appropriate history and diagnostic tests for TBRD;
develop a differential diagnosis that includes and ranks TBRD;
make treatment decisions based on epidemiologic and clinical evidence;
recognize that doxycycline is the treatment of choice for both adults and children;
recognize that early and empiric antibiotic therapy can prevent severe morbidity or death;
identify the availability, limitations, and utility of confirmatory laboratory assays;
recognize potential severe manifestations of TBRD; and
report suspected and confirmed cases to appropriate public health authorities to assist with control measures
and public health education efforts.
This report also provides resources on TBRD for health-care and public health professionals. Clinical cases
are included for self-evaluation and to reinforce the information presented in this guide. Additional information
concerning TBRD in this report is available from medical specialists, various medical societies, CDC, and state and local
health authorities.
Epidemiology of TBRD
RMSF, HME, and HGA are tickborne zoonoses caused by
Rickettsia rickettsii, Ehrlichia
chaffeensis, and Anaplasma
phagocytophilum, respectively. These pathogens are maintained in natural cycles involving wild mammals and
hard-bodied (ixodid) ticks. The epidemiologies of these diseases reflect the geographic distribution and seasonal activities of the
vectors and reservoirs and the human behaviors that place persons at risk for tick attachment and subsequent infection.
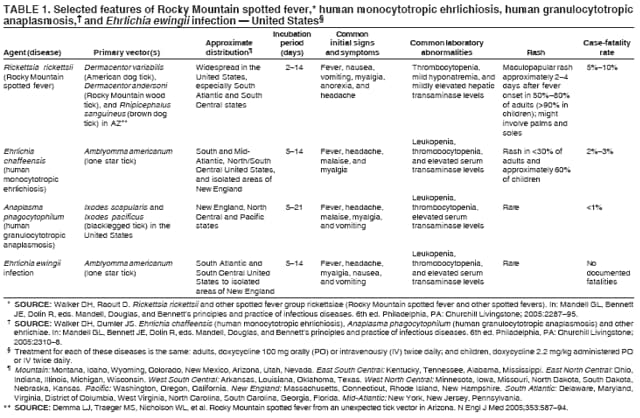
Selected epidemiologic and clinical features of TBRD have been summarized
(Table 1). RMSF, HME, and HGA are reported each month of the year in the United States,
although 90%--93% of reported cases occur during April--September
(6,10--12), coincident with peak levels of tick feeding activity on
humans. Travelers outside of the United States might also be
exposed to other tick vectors in other countries that transmit related agents that result in disease after they return to the
United States.
Males appear to be at higher risk for infection with all TBRD, possibly because of greater recreational or
occupational exposures to tick habitats. Although previous studies have indicated that the highest incidences of RMSF have
occurred in children aged <10 years, surveillance during 2003 demonstrates a higher age-specific incidence for RMSF
among persons aged 40--64 years, compared with other age groups
(13). For HME and HGA, the highest
age-specific incidences occurred among persons aged
>70 and 60--69 years, respectively
(14). The higher frequency of disease reporting in adults might reflect greater susceptibility to recognizable disease rather than higher infection rates.
Two recent cross-sectional studies in the southeastern and south central United
States* have indicated that up to 22% of children have serologic evidence of previous exposure to antigens of both
E. chaffeensis (15) and R. rickettsii
(16), suggesting that rickettsial and ehrlichial
infection might be more common than previously recognized.
RMSF
In the United States, R. rickettsii is transmitted to
humans by several tick species. However, the species that
transmit R. rickettsii most frequently include the American dog tick
(Dermacentor variabilis;Figure 1) in the eastern, central,
and Pacific coastal United States and the Rocky Mountain wood tick
(Dermacentor andersoni;Figure 2) in the western
United States. In 2005, the brown dog tick (Rhipicephalus
sanguineus;Figure 3), a vector of RMSF in Mexico
(17), was implicated as a vector of this disease in a confined geographic area in Arizona
(18). The cayenne tick (Amblyomma
cajennense;Figure 4) is a common vector for RMSF in Central and South America, and its range
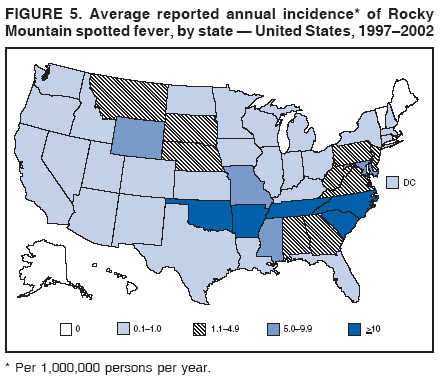
extends into the United States in Texas (19). During 1997--2002, the estimated average annual incidence of RMSF, based on
passive surveillance, was 2.2 cases per million persons. More than half (56%) of reported cases of RMSF were from only
five states: North Carolina, South Carolina, Tennessee, Oklahoma, and Arkansas (CDC, unpublished data, 2005).
However, cases have been reported from each of the contiguous 48 states, except Vermont and Maine
(10,11). Average reported annual incidence of RMSF per
1 million population, based on cases reported to CDC during 1997--2002, has
been reported (Figure 5). Incidence varies considerably by geographic area. RMSF is also
endemic throughout several countries in Central and South America, including Argentina, Brazil, Columbia, Costa Rica, Mexico, and
Panama (17,19,20). Household clusters of disease and hyperendemic foci of infected ticks have been
reported (3,21). Dogs are susceptible to RMSF, and they might frequently develop the disease concurrently with other household members in
an endemic focus (22,23).
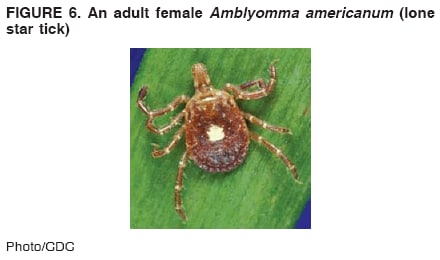
HME
E. chaffeensis is transmitted to humans by the lone star tick,
A. americanum (Figure 6), and possibly other ticks.
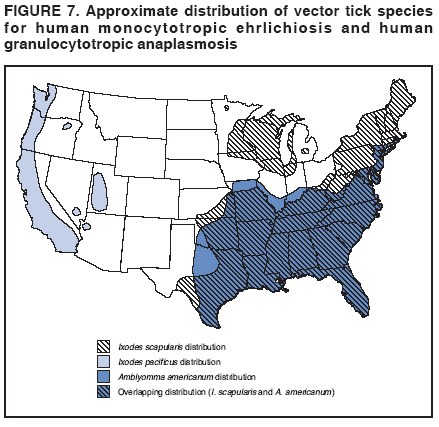
The white-tailed deer is a major host of all stages of lone star ticks and is an important natural reservoir
for E. chaffeensis. Natural infections of coyotes, dogs, and goats have been documented. The lone star tick is among the
most commonly encountered ticks in the southeastern United States, with range extensions into areas of the South
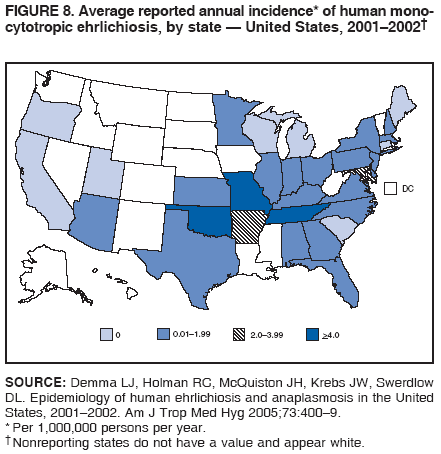
Central and New England states (Figure 7). Cases of HME are most commonly reported to CDC from Missouri,
Oklahoma, Tennessee, Arkansas, and Maryland, although the disease is found throughout the range of the lone star tick. The
average reported annual incidence of HME was 0.7 cases per million population, but incidence varied by state, based on
cases reported to CDC from 2001 to 2002 (Figure 8). In a prospective study among febrile patients with a history of a
recent tick bite in central North Carolina, the incidence of ehrlichial infection was approximately twice that of RMSF
(24). The reported incidence probably represents an underestimate of the true burden of disease in areas where
E. chaffeensis is endemic (24,25). Clusters of HME have been reported, suggesting that foci of ticks
infected with E.chaffeensis do
occur(21,26).
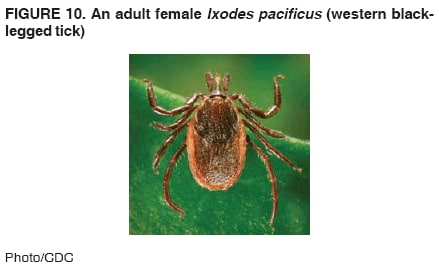
HGA
The blacklegged tick (Ixodes scapularis;
Figure 9) is the vector of A.
phagocytophilum in New England and North
Central United States, whereas the western blacklegged tick
(Ixodes pacificus; Figure 10) is the principal vector in northern
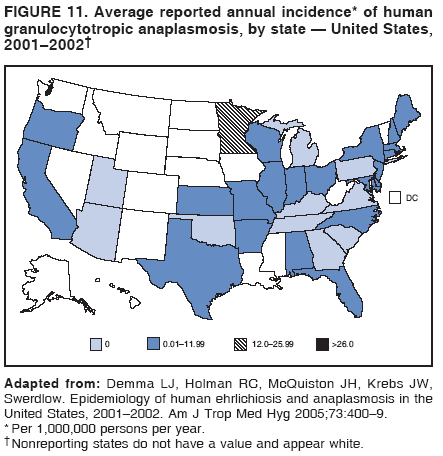
California. Deer, elk, and wild rodents are thought to be reservoirs. HGA is more frequently reported than HME, resulting in an
average reported annual incidence of 1.6 cases per million during 2001--2002. States that reported the highest
incidence during this period were Rhode Island (36.5 cases per million), Minnesota (12.3 cases per million), Connecticut (8.1 cases per
million), New York (2.3 cases per million), and Maryland (1.6 cases per million)
(Figure 11). HGA has been identified as a
substantial cause of unexplained fever during the tick season in Wisconsin
(27). Evidence suggests that the incidence of HGA
in Wisconsin might be much higher than that in Minnesota
(7). Because these Ixodes species ticks also transmit
Borrelia burgdorferi (the causative agent of Lyme disease) and various
Babesia species (agents of human babesiosis), the preponderance
of cases of HGA occur in the same states that report high incidences of Lyme disease and human babesiosis.
Simultaneous infection with A.
phagocytophilum and B. burgdorferi has been reported
(28), and discerning such a mixed infection is
vital because it might affect antimicrobial choice. For example, amoxicillin can be used to treat early stage Lyme disease, but it is
not effective for HGA.
Ehrlichia ewingii Infection
Amblyomma americanum also is the principal vector of the ehrlichial pathogen,
E. ewingii. The ecologic features of E. ewingii
are not completely known; however, dogs and deer have been naturally infected. Cases of
granulocytotropic ehrlichiosis caused by E.
ewingii have been reported primarily in immunocompromised patients from
Missouri, Oklahoma, and Tennessee (29,30).
E. ewingii infections in dogs or ticks also have been described in these states and
in Arkansas, Texas, Florida, Georgia, Mississippi, North Carolina, and Virginia, suggesting that human infections with
this pathogen might be expected to occur throughout the range of the lone star tick
(31,32).
The following is a summary of the salient epidemiologic features of TBRD:
Occurrence is seasonal, with the majority of illness onset during warmer spring and summer months, but cases
might develop throughout the year.
RMSF has been reported in all of the contiguous 48 states, except Vermont and Maine.
RMSF and HME are most commonly reported in the southeastern and south central United States.
HGA is reported most frequently in New England, the north central states, and in focal areas along the West Coast.
Pathogen Tropisms and Clinical Presentation
R. rickettsii, E. chaffeensis,
E. ewingii, and A. phagocytophilum have specific and distinct cell tropisms.
R. rickettsii infects endothelial cells and more rarely infects underlying smooth muscle cells, where rickettsiae multiply freely in
the cytoplasm. The rickettsiae cause a small-vessel vasculitis,
resulting in a maculopapular or petechial rash in the
majority of patients. Vasculitis occurring in organs (e.g., the brain or lungs) can result in life-threatening complications.
R. rickettsii does not stain with the majority of routine histopathologic stains and is not detected by blood smear evaluation
because of limited numbers of circulating bacteria. Ehrlichioses and anaplasmosis are characterized by infection of
leukocytes, where the causative agents multiply in cytoplasmic membrane-bound vacuoles as microcolonies called morulae.
E. chaffeensis most frequently infects monocytes, whereas
A. phagocytophilum and E. ewingii demonstrate
a predilection for granulocytes. Morulae may be stained with conventional Wright or
Giemsa stains and are occasionally observed in leukocytes in smears of
peripheral blood, buffy coat preparations, or cerebrospinal fluid. In this context, a routine
blood smear can provide a presumptive clue for early diagnosis; however, the visualization of morulae still requires
confirmatory testing for Ehrlichia or Anaplasma
species by serology, polymerase chain reaction (PCR), or immunostaining methods
(33). The demonstration of morulae is also not sensitive, and a case of ehrlichiosis or anaplasmosis might be missed if
the diagnosis relies solely on detection of morulae on blood smears. Although the
diagnostic sensitivity of a blood smear is greater for HGA than for HME, blood smears might only be positive in up to 60% of patients with HGA
(34).
The following is a summary of salient features of pathogen tropisms:
R. rickettsii infects endothelial cells, causing vasculitis, which leads to rash and life-threatening damage to the
brain, lungs, and other viscera.
R. rickettsii is not evident in blood smears, and these bacteria and do not stain with the majority of conventional stains.
Ehrlichia and Anaplasma species infect monocytes or granulocytes, respectively, and morulae might occasionally be
observed on peripheral blood smears by using routine stains.
Clues from the Clinical History
A thorough clinical history that elicits recent tick exposure, specific recreational or occupational exposures to
tick-infested habitats, recent travel to areas where TBRD might be endemic, or similar illnesses in family
members, coworkers, or pet dogs can provide critical information that can be used to make a presumptive diagnosis of TBRD
and help guide subsequent therapeutic actions. However, the absence of certain features does not exclude a diagnosis
of TBRD. These features include 1) history of tick bite or exposure, 2) recent travel to areas endemic for TBRD, and
3) similar illness in family members, coworkers, or pets.
History of Tick Bite or Exposure
A detailed medical history might reveal activities that suggest potential exposure to ticks. Outdoor activities
during April--September, particularly in areas with high uncut grass, weeds, and low brush can increase the risk for tick
bites (35). These activities include recreational pursuits (e.g., camping, hiking, fishing, hunting, gardening, and
walking dogs) as well as occupational activities that involve persons being in brushy or grassy areas that might be inhabited
by ticks. Vegetation that borders roads, trails, yards, or fields also are potential areas that might be inhabited by ticks.
In endemic areas (where the agents causing TBRD are present at all times), even adults or children who play in grassy
areas in their backyard are at risk. Queries concerning frequency of contact with family pets, especially dogs, and findings
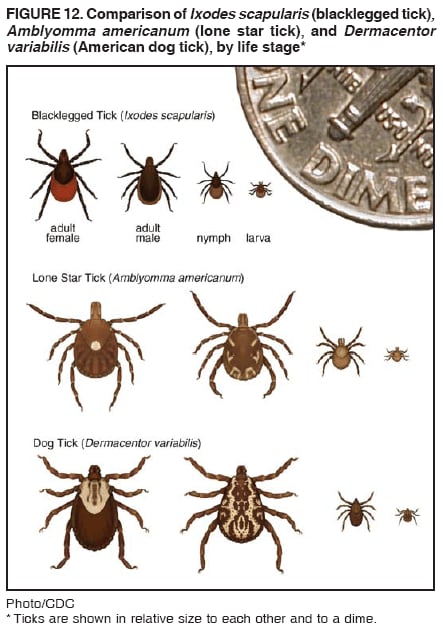
of tick attachment to animals or removal can be useful. The majority of patients will not recall or recognize an attached
tick because the location of the tick might be obscure; the bite is typically painless; and bites from smaller immature
stages of ticks (e.g., nymphs are approximately 1--2 mm
or the size of the head of a pin; Figure 12) might not be
readily detected but might still result in infection. A specific history of a tick bite within 14 days of illness onset is
typically only reported in 60% of RMSF cases
(10,11) and has been reported in only 68% of ehrlichiosis cases
(6). Therefore, the absence of definite tick attachment should never dissuade a physician from considering the
diagnosis of a TBRD.Finally, certain patients do not specifically recall tick exposure but might describe other pruritic, erythematous, or
ulcerated cutaneous lesions that they call a mosquito bite, spider bite, chigger bite, or bug bite, which can be
indistinguishable from an actual tick bite.
Recent Travel to Areas Endemic for TBRD
Clinicians in areas of the United States where the incidence of TBRD is historically low are typically at a
disadvantage in distinguishing these diseases among multiple other infectious and noninfectious syndromes that they
resemble. Because TBRD are typically sporadic, identifying these infections requires high clinical acumen, especially in
an environment in which TBRD have not previously been recognized as occurring frequently.
Knowledge of the epidemiology of these illnesses, including regions of the country with a high incidence (number
of reported cases per million persons per year) of TBRD (e.g., south Atlantic, north central, and south central and
New England states), is important. A history of recent travel from an endemic area of TBRD (e.g., within 2 weeks
preceding illness), especially if the patient had participated in an outdoor activity, might support a suspicion of tickborne
illness. Physicians should also consider the possibility that changes in tick vector range can influence the distribution of
TBRD. In addition, in 2004, a total of 13 cases of RMSF occurred in eastern Arizona, a state in which the disease was
previously rarely diagnosed (18).
Clinicians should also consider that TBRD occur worldwide and might have epidemiologic, seasonal, and
clinical features distinct from those observed in the United States. International travel to destinations (e.g.,
southern Mediterranean, Central and South America, Africa, Asia, and the Middle East) might result in tick vector
exposure, particularly if the patient participated in rural or outdoor
activities. For example, African tick-bite fever (ATBF),
an increasingly reported travel-related rickettsiosis caused by
R. africae, has an estimated incidence of 4%--5.3%
among international travelers to sub-Saharan Africa and has been identified in clusters of
infection among group travelers (e.g., game hunters, safari tourists
[36], and humanitarian workers; 37). A related rickettsial organism,
R. conorii, endemic in the Mediterranean basin, Middle East, and parts of
Africa and the Indian subcontinent causes Mediterranean
spotted fever (MSF; 38). ATBF and MSF are characterized by fever, malaise, headache, and myalgia, which are typical
symptoms for other TBRD. However, a distinguishing clinical feature of both
travel-related diseases is the development of one
or more eschars (a dark, scab-like plaque overlying a shallow ulcer with surrounding erythema or scaling) at the site of
tick attachment that is noted coincident with or shortly after the
onset of fever in 30%--50% of patients
(36,39).
Emerging TBRD
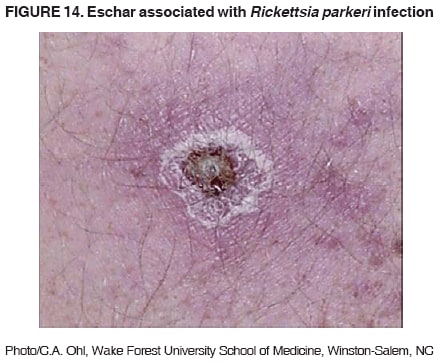
Similarly, considering TBRD as a diagnosis is essential
because of new, previously unrecognized rickettsial
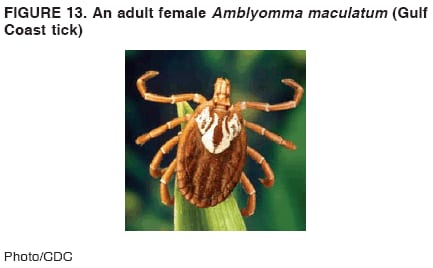
pathogens that have been observed in tick vectors in the United States. For example, in 2002,
R. parkeri was identified as a new cause of spotted fever rickettsiosis in a patient living in the southeastern coastal United States
(40). This agent is present in A.
maculatum (the Gulf Coast tick; Figure 13), which is found in the southeastern United States. A
clinical presentation, similar to ATBF and MSF (i.e., fever, headache, eschars, and
regional lymphadenopathy), was observed in a patient with no substantial travel history
(Figure 14). The diagnosis of spotted fever rickettsiosis was confirmed by
using rickettsial culture from an eschar skin biopsy and serologic and molecular methods
(40). Other spotted fever group rickettsiae might also cause mild febrile illness in certain persons exposed to ticks in highly endemic areas
(41). The common observation of antibodies to rickettsiae and ehrlichiae in persons and dogs might indicate exposure to
other rickettsial agents of varying pathogenicity
(15,16,24).
Similar Illness in Family Members, Coworkers, or Pets
Clinicians might be inclined to offer diagnoses of a communicable viral infection when more than one family
member is affected by an illness. However, clustering of certain TBRD is a well-recognized epidemiologic phenomenon
and might occur after exposure to natural foci of infected ticks. Temporally and geographically related clusters
occurring among family members, coworkers, or persons frequenting a particular common area have been observed. These
clusters include family clusters of RMSF (3), clusters of ehrlichiosis among residents of a golfing community
(26), and soldiers on field maneuvers
(21). Common exposures to tick-infested habitats or outdoor activities might place certain or
all members of a family or group, including pet dogs, at risk for TBRD. Concurrent infections with
R. rickettsii and Ehrlichia species also have been observed in humans and dogs
(22,24,29). Therefore, clinicians should query
patients concerning similar illnesses among family members, close coworkers, or community residents, and even
among household dogs.
The following is a summary of salient features of clues from the clinical history:
A detailed history of recent recreational or occupational activities might reveal potential exposure to ticks.
Exposure can occur in the patient's backyard or neighborhood.
Familiarity with TBRD epidemiology will be helpful when querying patients regarding recent travel
to endemic areas (domestic and international;
38,39).
Clustering of certain TBRD is well-recognized and has been reported among family members, coworkers, and
other defined groups.
Clinical Assessment
Signs and Symptoms
The early signs and symptoms of HME, HGA, RMSF, and
E. ewingii infection might resemble nonspecific findings
of other infectious and noninfectious diseases. The
majority of patients with TBRD visit a physician during the first
2--4 days of illness, after an incubation period of approximately 5--10 days after a tick bite
(5). Patients with HGA might seek medical care later (4--8 days after fever onset)
(7). Substantial overlap occurs in the initial clinical presentation
of the three diseases. Initial symptoms commonly include a sudden onset of fever, chills, and headache,
commonly associated with malaise and myalgia. In adults, photophobia might be observed. Headache is nearly always reported
by adults who seek medical care and can be severe. Patients also might report nausea, vomiting, and anorexia early in
the course of their illness, especially with RMSF
(35) and HME in children. Diarrhea might occasionally
occur. Other frequently observed signs and symptoms in children with either RMSF or HME are
abdominal pain, altered mental status, and conjunctival injection. Abdominal pain might be severe enough to mimic appendicitis or other causes
of acute abdominal pain (42). Certain findings described in medical textbooks are less commonly observed by
clinicians and include bilateral periorbital
edema, edema of the dorsum of hands and feet, and calf pain and tenderness.
Because the signs and symptoms that persons have when they first seek medical care are nonspecific, clinicians frequently
must incorporate clues from the clinical and epidemiologic history and consider other features (e.g., the presence of rash
or abnormalities of routine laboratory tests).
In RMSF, a rash typically appears 2--4 days after onset of fever; however, the majority of patients will seek medical
care before this period. For adults and children with RMSF, rash frequently occurs earlier in children than in adults
(43) and is eventually observed in approximately 90% of children. The exanthem typically begins as small, blanching,
pink macules on the ankles, wrists, or forearms that evolve to maculopapules
(Figure 15). In half of cases, the rash might evolve to petechiae over the next several days of illness. The classic centripetal spread of rash is typically not noticed
by the patient and might be difficult to elicit from the clinical history. The rash can expand to involve the entire
body, including the palms and soles, but its presence on the face is usually limited. Discerning the rash in
darker-skinned persons might be difficult. The classic spotted or generalized petechial rash of RMSF is usually not apparent until
the fifth or sixth day of the illness and signifies progression of the disease,
although the progression is considerably variable
(Figure 16). Patients with petechial rash are often severely ill, and
although fever and organ dysfunction might resolve quickly with treatment, complete recovery can take longer to
occur. The rash progression of RMSF includes
several critical exceptions and considerations.
A rash on the palms and soles is not pathognomonic and might occur in illnesses caused by drug
hypersensitivity reactions, infective endocarditis, and a diverse group of other agents, including
Treponema pallidum, Neisseria
meningitidis, Streptobacillus
moniliformis, E. chaffeensis, and certain enteroviruses.
The rash might be evanescent or localized to a particular region of the body.
A rash might be completely absent or atypical in up to 20% of RMSF cases
(4,43,44).
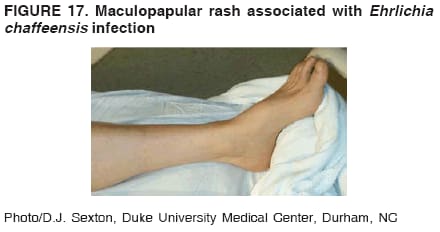
Rash is observed in approximately one third of all
patients with HME (although rash is described in up to 66%
of children) and is rare in patients with HGA or
E. ewingii infection (45,46). For children with HME and a
rash, distinguishing the condition from RMSF might be difficult. Rash patterns occasionally associated with HME vary
in character from petechial or maculopapular
(Figure 17; 47) to diffuse erythema
(48) and typically occur later in the course of disease
(median: 5 days after onset; 6).The rash patterns might involve the extremities, trunk, face or,
rarely, the palms and soles (49).
In certain cases, patients with RMSF or ehrlichiosis might seek medical attention for a febrile illness that mimics
viral meningoencephalitis. Focal neurologic deficits, including cranial or peripheral motor nerve paralysis or sudden
transient deafness, might also be observed
(50).
Differential Diagnosis of Febrile Patients with Rash
The differential diagnosis of febrile patients with rash is broad. The onset of TBRD is frequently rapid, and
the majority of patients experience high fever, shaking chills,
severe headache, and generalized myalgias, in contrast to
other tickborne diseases (e.g., Lyme disease). Tickborne viral fevers (e.g., Colorado tick fever) infrequently cause rash but
should be included in the differential diagnoses of TBRD, particularly when leukopenia and thrombocytopenia are present in
a patient who has recently traveled to the western United States. Clinically, TBRD might be essentially
indistinguishable from the majority of viral infections, particularly those in children. The dermatologic classification of the rash,
its distribution, pattern of progression and timing relative to onset of fever, and other systemic signs provide clues that
help the clinician rule out other exanthemata. Maculopapular rashes might
occur in association with multiple conditions, including human herpesvirus 6 infection (i.e., roseola), human parvovirus B19, enteroviral infection (e.g.,
coxsackievirus and echovirus), Epstein-Barr virus infection, disseminated gonococcal infection,
Mycoplasma pneumoniae infection, leptospirosis, secondary syphilis, Kawasaki disease, thrombotic thrombocytopenic purpura
(TTP), drug reactions, and immune complex-mediated illness
(51). A petechial rash can occur in association with meningococcal infection,
enteroviral infection, immune thrombocytopenic purpura, and after group A streptococcal pharyngitis.
R. rickettsii infection is noted for causing a rash on the soles and palms, although this distribution typically occurs late in RMSF and in only half of
cases, whereas in the majority of other bacterial or viral infections rash has not been
observed. Initially, clinicians might experience difficulty distinguishing
N. meningitidis infection from RMSF because both can
begin as a maculopapular rash and progress to a petechial rash, but the rash and other clinical features progress more rapidly in meningococcemia than in
RMSF.
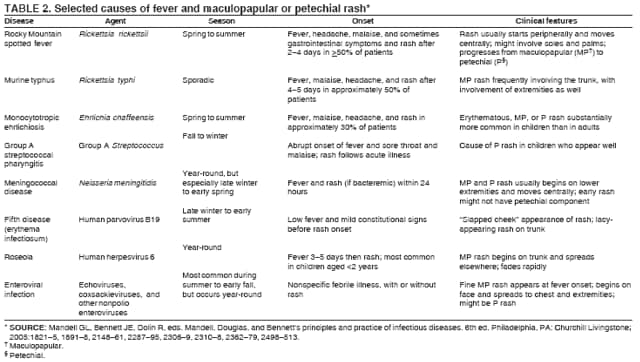
Selected infectious causes and features of maculopapular and petechial rash illnesses have been reported
(Table 2). Other exanthematous diseases that can occasionally be confused with TBRD include toxic-shock syndrome, erythema
multiforme, and Stevens-Johnson syndrome.
Laboratory Findings
Obtaining a complete blood cell count (CBC), comprehensive metabolic panel, and examination of peripheral
blood smear are essential when considering a diagnosis of TBRD. The total white blood cell (WBC) count is typically
normal in patients with RMSF, but increased numbers of immature bands are generally observed. Thrombocytopenia,
mild elevations in hepatic transaminases, and hyponatremia might be observed with RMSF
(35), whereas leukopenia (up to 53% of patients), thrombocytopenia (up to 94% of patients), and modest elevations of liver transaminase levels
are particularly suggestive of HME and HGA
(52,53). An inverse relation has been reported between the mean WBC
and platelet count and the probability that HGA is the cause of nonspecific fever
(53). Blood smears might be useful in identifying patients with HGA
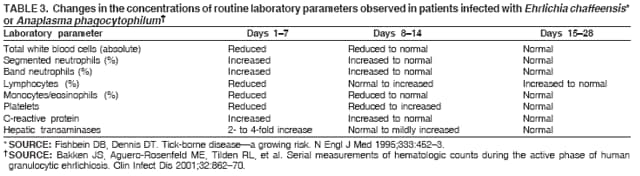
(34) or E. ewingii infection. Nonspecific changes
in the concentrations of routine laboratory parameters that have been observed for patients infected with
E. chaffeensis (52) or A.
phagocytophilum have been reported
(53;Table 3).
Cerebrospinal fluid (CSF) analysis might be a useful
adjunct to laboratory diagnosis of TBRD. When CSF is
evaluated in patients with RMSF or HME, a pleocytosis (usually <100 cells/microliter) is typically observed (with either
a polymorphonuclear or lymphocytic predominance), whereas CSF evaluated in
E. ewingii infection is characterized by a neutrophilic pleocytosis
(29). Moderately elevated protein (100--200 mg/dL) and normal glucose levels also
are commonly observed in patients with RMSF
(54,55). A Gram stain indicating gram-negative diplococci, very low
glucose (i.e., <20--30 mg/dL), or neutrophilic pleocytosis is more suggestive of meningococcal meningitis. Clinicians
should distinguish TBRD-related CNS involvement from other infections (e.g.,
N. meningitidis); however, in the majority
of patients, reliably distinguishing between RMSF, HME, and meningococcal infection based on laboratory testing is
difficult (unless a pathogen is cultured). Therefore, empiric treatment for both TBRD and meningococcemia is necessary for
ill patients with fever and rash and for patients in whom neither disease can be ruled out.
The following is a summary of salient clinical assessment features:
Early clinical presentations of HME, HGA, RMSF, and
E. ewingii infection include fever, headache, myalgia,
and malaise and are difficult to distinguish from other infectious and noninfectious diseases.
Patients with RMSF typically do not have a spotted or petechial rash when they initially seek medical care during
the first 2--4 days of illness.
A CBC, metabolic panel, and peripheral blood smear
examination are helpful in developing both a
differential diagnosis and treatment approach to TBRD.
CSF analysis might reveal neutrophilic or lymphocytic pleocytosis and elevated protein but might not
reliably distinguish TBRD and meningococcal disease,
necessitating empiric antibiotic therapy for both conditions
when indicated.
Leukopenia, thrombocytopenia, mild hyponatremia, and mildly elevated hepatic transaminase levels are common
and particularly useful clinical features of TBRD, although the absence of these features does not exclude a diagnosis
of TBRD.
Infrequent features of TBRD include severe abdominal pain and meningoencephalitis.
Rash is observed frequently in RMSF, occasionally in HME, and rarely in HGA or
E. ewingii infection.
Treatment and Management
An assessment of clinical signs and symptoms, along with laboratory diagnostic tests and a thorough clinical
history, will help guide clinicians in developing a differential diagnosis and treatment plan. At least 50% of patients with
TBRD might need to be hospitalized. Patients with evidence of organ dysfunction and severe thrombocytopenia, mental
status changes, and the need for supportive therapy should be hospitalized. Essential considerations include social factors,
the likelihood that the patient can and will take oral medications, and existing comorbidities. For
example, a patient who appears well, has acute febrile illness and an unrevealing history and physical examination, and whose laboratory
indices are within normal limits might warrant a "wait and watch" approach for 24 hours with reassessment if the
patient fails to improve. If laboratory testing of a patient with a history compatible with TBRD reveals leukopenia
or thrombocytopenia, or metabolic abnormalities, the
clinician should consider obtaining blood cultures for other
likely pathogens and specific laboratory tests and initiating empiric oral antimicrobial therapy that will
effectively treat TBRD. Certain patients with TBRD can be treated on an outpatient basis with oral medication, particularly if a
reliable caregiver is available in the home and the patient is compliant with follow-up medical care. When other diagnoses
are under consideration, empiric treatment for these conditions can be incorporated into the therapeutic plan. For
example, for a patient's condition in which meningococcal disease cannot be ruled out,
intramuscular ceftriaxone should be administered in addition to oral doxycycline to provide activity against possible meningococcal infection,
pending culture results. Inpatient observation and assessment of the blood cultures after 24 hours of incubation should
be considered for such patients. A critical step is for clinicians to keep in close contact with patients who are treated in
the outpatient setting to ensure that they are responding to therapy as
expected.
Appropriate antibiotic treatment should be initiated
immediately when a clinician suspects that the diagnosis
could be RMSF, HME, HGA, or E. ewingii infection, based on clinical, laboratory, or epidemiologic findings. Delay
in treatment can lead to severe disease and fatal outcome for TBRD
(2--4). Because each of the agents causing TBRD
is susceptible to tetracycline-class antibiotics, these drugs, particularly doxycycline, are considered the therapy of choice
in nearly all clinical situations. Fever typically subsides within 24--48 hours after treatment when the patient
receives doxycycline or another tetracycline during the first 4--5 days of illness. If a patient fails to respond to early
treatment with a tetracycline antibiotic (i.e., within 48 hours), this response might be an indication that their condition is not
a TBRD. Severely ill patients might require longer periods before clinical
improvement is noted, especially if they have multiple organ dysfunction.
Doxycycline is the drug of choice for treatment of all TBRD in children and adults. This drug is bacteriostatic in
its activity against rickettsial organisms. The recommended dose is 100 mg per dose administered twice daily (orally
or intravenously) for adults or 2.2 mg/kg body weight per dose administered twice daily (orally or intravenously)
for children weighing <100 lbs. (45.4 kg). Intravenous
therapy is frequently indicated for hospitalized patients, and
oral therapy is acceptable for patients considered to be early in the disease and who can be managed as outpatients.
Oral therapy also can be used for inpatients who are not vomiting or obtunded. The optimal duration of therapy has not
been established, but current recommendations for RMSF and HME are for treatment for at least 3 days after the
fever subsides and until evidence of clinical improvement is noted, which is typically for a minimum total course of 5--7
days. Severe or complicated disease might require longer treatment courses.
Patients with HGA should be treated with doxycycline for 10--14 days to provide appropriate length of therapy for possible incubating coinfection with
Lyme disease (45).
The use of tetracyclines to treat children with TBRD is no longer a subject of controversy
(56--58). Concerns regarding dental staining after tetracycline therapy have been based primarily on studies conducted during the
1960s that involved children receiving multiple courses of the drug for recurrent otitis media
(59,60). The propensity of tetracyclines to bind calcium can lead to darkening of the teeth if the antibiotic is ingested during the period of
tooth crown formation. More recent studies in 1971 and 1998, however, have demonstrated that although multiple
exposures to tetracycline increase the risk for tooth staining, limited use of this drug in children during the first 6--7 years of
life has a negligible effect on the color of permanent incisors
(56,57). Beyond ages 6--7 years, the risk for
tetracycline staining is of minimal consequence because visible tooth formation is complete. Moreover, a prospective study
of children treated with doxycycline for RMSF demonstrated that these children did not have substantial discoloration
of permanent teeth compared with those who had never received the drug
(56). Because TBRD can be life-threatening
and limited courses of therapy with tetracycline-class antibiotics do not pose a substantial risk for tooth staining,
the American Academy of Pediatrics Committee on Infectious Diseases revised its recommendations in 1997 and
has identified doxycycline as the drug of choice for treating presumed or confirmed RMSF and ehrlichial
infections in children of any age (61,62).
Chloramphenicol is an alternative drug that has been used to treat RMSF
(50); however, this drug is associated with various side effects and might require monitoring of blood indices. Chloramphenicol is no longer available in the oral
form in the United States. Moreover, epidemiologic studies in which CDC case report data have been used suggested
that patients with RMSF treated with
chloramphenicol have a higher risk of dying than persons who received a
tetracycline (11,63). In vitro evidence also indicates that chloramphenicol might not be an effective antibiotic for HME or
HGA (64,65). Clinicians who suspect a TBRD and are considering empiric antibiotic therapy before laboratory
confirmation should be aware that doxycycline provides therapeutic coverage for RMSF, HME, HGA, and
E. ewingii infection.
Tetracyclines are generally contraindicated for use in pregnant women because of risks associated with malformation
of teeth and bones in the fetus and hepatotoxicity and pancreatitis in the mother
(66). However, tetracycline has been used successfully to treat HME in pregnant women
(67), and the use of tetracyclines might be warranted during
pregnancy in life-threatening situations where clinical suspicion of TBRD is high. Whereas chloramphenicol is typically
the preferred treatment for RMSF during pregnancy, care must be used when administering chloramphenicol late
during the third trimester of pregnancy because of risks associated with grey baby syndrome
(66). Substantially limited clinical data exist that support the use of other antimicrobials during pregnancy, although rifampin has been used successfully
in several pregnant women with HGA (68). In vitro studies have demonstrated that rifamycins provide effective
activity against Ehrlichia and Anaplasma
species (64,65), and therapy with rifampin may be considered for patients with
HGA who are unsuited for tetracycline treatment because of pregnancy or a history of drug allergy
(45). Clinicians should use caution, however, in ensuring that RMSF can be ruled out because the clinical presentations of RMSF and
anaplasmosis are similar, and the comparative effectiveness of rifampin and doxycycline is unknown at this time.
Because certain patients with TBRD might initially
receive an alternative diagnosis, they might be empirically
treated with antibiotics inactive against rickettsiae, including penicillins, cephalosporins, aminoglycosides, erythromycin,
or sulfonamides. This situation presents both diagnostic and therapeutic challenges. In certain cases,
patients treated with beta-lactam antibiotics or
sulfa-containing drugs are mistakenly thought to have drug
eruptions when they later manifest a rash
(66), further postponing a correct diagnosis and appropriate treatment. Because the physician might conclude
that the prescribed treatment will take time to work, a delay in obtaining
critical additional laboratory or clinical
information also might be a result. In addition, sulfa-containing antimicrobials have been associated with increased severity of
TBRD, although whether disease severity is directly related to the use of
sulfa-containing drugs or the delayed administration of
more effective antimicrobials is not clear. Cases of severe ehrlichiosis complicated by acute respiratory distress syndrome have been
associated with the use of trimethoprim-sulfamethoxazole
(69,70).
In addition, clinicians should note the overlap between early symptoms of invasive meningococcal infection
and TBRD. These conditions are difficult to distinguish early in the course of illness. In patients for whom both
conditions are included in the initial differential diagnoses, after performing blood cultures and a lumbar puncture,
empirically treating for both diseases is appropriate. This treatment can be accomplished by adding an appropriate
parenteral penicillin or cephalosporin that has activity against
N. meningitidis to doxycycline therapy.
Preventive antibiotic therapy for rickettsial infection is not indicated for patients who have had recent tick bites
and are not ill. Limited numbers of ticks in areas where tickborne diseases are endemic are infected with
pathogenic rickettsiae. Approximately 1%--3% of vector ticks are
infected with spotted fever group rickettsiae
(71). However, less than 1% of these rickettsiae usually have been confirmed to be
R. rickettsii (72,73). Approximately
5%--15% of lone star ticks are infected with E. chaffeensis
(47), and 10%--50% of I.
scapularis ticks are reported to be infected
with A. phagocytophilum (74,75) in endemic areas. Therefore, the risk for such infection after a tick bite is low. Moreover, for
RMSF, preventive therapy has been demonstrated to delay but not prevent the onset of symptoms
(76).
The following is a summary of salient features of treatment and management:
Clinical history, symptoms, and physical and laboratory findings should guide the clinician's approach to
patient management and treatment.
Not all patients with TBRD will require hospitalization.
Clinicians may consider a wait and watch approach for 24--48 hours for patients early in the course of illness and
who have nonsupporting history, nonspecific clinical signs, and normal laboratory findings.
Doxycycline is the drug of choice for the treatment of presumptive or confirmed TBRD in both adults and children.
Limited courses of tetracycline-class antibiotics (e.g., doxycycline) do not pose a substantial threat of tooth staining
in children.
Tetracyclines typically are contraindicated for use
during pregnancy but might be warranted in life-threatening
situations where clinical suspicion of TBRD is high.
Delay in treatment can lead to severe disease and fatal outcome of TBRD.
In evaluating for TBRD, when early invasive meningococcal infection cannot be ruled out, providing treatment
for both conditions by adding an antimicrobial that has activity against N. meningitidis is appropriate.
Prophylactic use of antibotics after a tick bite is not
recommended.
Considerations for Management of Patients with Severe Manifestations
of TBRD
A substantial number of patients with TBRD require hospitalization
(6,7,10). Severe manifestations of TBRD
might include prolonged fever, renal failure, disseminated intravascular coagulopathy (DIC), hemophagocytic
syndrome, meningoencephalitis, and acute respiratory distress syndrome.
A notable exception is that HGA has not been
associated with meningoencephalitis.
RMSF is frequently a severe illness, and patients commonly require hospitalization. Up to 20% of untreated cases
and 5% of treated cases have fatal outcome, making RMSF the most commonly fatal rickettsial disease in the United
States (5,10). However, assessment of passive reporting of RMSF-associated death has suggested that only one third of
fatal cases of RMSF were reported to CDC during 1983--1998
(77). Therefore, the actual case-fatality rate of RMSF
might be closer to 5%--10%. Host factors associated with severe or fatal RMSF
include advanced age, male gender, black race, chronic alcohol abuse, and glucose-6-phosphate-dehydrogenase (G6PD) deficiency
(50). Deficiency of G6PD is a sex-linked genetic condition affecting approximately 12% of the U.S. black male population; deficiency of this enzyme
is associated with a high proportion of fulminant cases of RMSF
(50,78). Fulminant cases follow a clinical course that
is fatal within 5 days of onset. Long-term health effects persisting for >1 year after acute RMSF infection include
partial paralysis of the lower extremities; gangrene requiring amputation of fingers, toes, arms, or legs; hearing loss;
blindness; loss of bowel or bladder control; movement disorders; and speech disorders
(79). These complications are observed most frequently in persons
recovering from severe, life-threatening disease, often after lengthy hospitalizations. Digital
necrosis in a patient occurring late in the course of RMSF has been illustrated
(Figure 18).
Similarly, HME and HGA can cause serious or fatal disease as well, although at lower rates than are observed
for RMSF. At least 50% of patients with HGA and HME are hospitalized to rule out other potentially
life-threatening conditions and to manage the illness
(34,47). Clinical indications for admission might include
immunocompromised state, pain management (i.e., headache and myalgias), mental confusion, cough, infiltrate in chest radiograph,
abnormal spinal fluid findings, or specific acute organ failure. Approximately 3% of HME patients and less than 1% of
HGA patients with symptoms severe enough to seek medical attention will die from the infection
(25,34,47). The severity of ehrlichiosis might be related, in part, to the immune status of the patient. Persons with compromised immune
systems caused by immunosuppressive therapies (e.g., corticosteroids or cancer chemotherapy), human
immunodeficiency virus (HIV) infection, organ transplantation, or splenectomy appear to develop more severe disease from
E. chaffeenis infection, and case-fatality rates for these persons are characteristically higher than
case-fatality rates reported for the general population
(30). Although the case fatality rate for HGA (0.5%--1.0%) is lower than that for HME,
notable complications, including respiratory failure, a toxic-shock--like syndrome, rhabdomyolysis, pancreatitis, acute
renal failure, and invasive infections caused by opportunistic viral or fungal agents can occur, especially among patients
who have co-morbid illnesses or who are actively immunosuppressed
(45). In addition, advanced patient age and delay
in diagnosis and the onset of specific antibiotic therapy are predictors of a more severe course of HGA
(53).
Management of severely ill patients with TBRD should
include careful assessment of fluid and electrolyte
balance. Vasopressors and rigorous fluid management might be needed, especially when the illness is complicated by renal
failure or hypotension. Patients might have pulmonary
infiltrates because of vasculitis that are erroneously thought to be
caused by cardiac failure or pneumonia. Seizures might require
aggressive treatment, and arrhythmias (e.g., atrial fibrillation
or flutter) will frequently respond to treatment of the patient's underlying disease. Consultation with an intensivist or
an infectious disease subspecialist might be helpful in managing these complications.
The following is a summary of salient features of severe manifestations:
TBRD can be life-threatening.
Severe manifestations of TBRD include prolonged
fever, renal failure, myocarditis, meningoencephalitis,
hypotension, acute respiratory distress syndrome, and multiple organ failure.
Confirmatory Diagnostic Tests
Rickettsial infections pose difficult diagnostic challenges to both clinicians and laboratorians. Rapid
confirmatory assays are not commonly available to guide treatment decisions of acutely ill patients. However, confirmatory assays
provide the physician with vital information that retrospectively validates the accuracy of the clinical diagnosis.
Laboratory confirmation of infection is also vital to understanding the epidemiology and public health impact of TBRD.
Several laboratory methods are available to diagnose TBRD. However, they vary in the time required to obtain
results and in the type of information they provide the clinician. Therefore, treatment decisions should be based
on epidemiologic and clinical clues and should never be
delayed while waiting for laboratory confirmation of a
diagnosis. Similarly, test results should be interpreted in the context of the patient's illness and the epidemiologic setting.
Misuse of specialized tests for patients with a low probability of the disease and in areas with a low prevalence of disease
might result in confusion. A fundamental understanding of the signs, symptoms, and epidemiology of the disease is critical
in guiding requests for tests and interpretation of test results for ehrlichioses, anaplasmosis, and RMSF. Studies
have suggested that antibiotic therapy might diminish the development of convalescent
antibodies in RMSF (CDC, unpublished data, 2005). However, the degree to which doxycycline might cause this
occurrence is uncertain. If molecular or culture diagnostic methods are conducted, obtaining blood for testing before antibiotics are administered
is essential to obtain the best results.
Blood-Smear Microscopy
Microscopic examination of blood smears stained with eosin-azure type dyes (e.g., Wright-Giemsa stain) might
reveal morulae in the cytoplasm of infected circulating leukocytes (1%-- 20%) of patients with HME and 20%--80%
of patients with HGA (45,47) during the first week of
infection, which is highly suggestive of ehrlichial or
anaplasma infection. However, blood smear examination is
insensitive and should be performed by an experienced
microscopist. In addition, a negative blood smear examination should not dissuade the caregiver from initiating treatment
with doxycycline if the clinical presentation and routine laboratory findings support the diagnosis of ehrlichiosis
or anaplasmosis. Blood smear examination is not useful for diagnosis of RMSF.
Serologic Testing
Serologic assays for RMSF, HME, and HGA are commonly available through multiple commercial and state
public health laboratories. Serologic evaluations are commonly conducted by using the indirect immunofluorescence
antibody (IFA) assay. Antibodies in the serum bind to fixed antigens on a slide and are detected by a fluorescein-labeled
conjugate. Although IFA remains the principle diagnostic tool for the diagnosis of rickettsial and ehrlichial infections, no
standardized antigens, conjugates, or agreement on what constitutes a positive result among the various laboratories providing these
tests exist. Individual laboratories should be consulted regarding their test threshold levels. Enzyme-linked
immunosorbent assay (ELISA) is becoming a more frequently used assay. Similar to IFA, the accuracy of
ELISAdepends on the laboratory conducting the test, the quality and specificity of the antigen, and the threshold levels at which a positive
result is considered. Available ELISA tests are qualitative and cannot be used effectively to monitor increases or
decreases in antibody titer.
The sensitivity of the IFA assay is substantially dependent on the timing of collection of the sample. Early in
any TBRD, a majority of serologic tests will be negative. Clinical illness nearly always precedes laboratory diagnosis by
any method. As the illness progresses to 7--10 days, the sensitivity of IFA serology increases. The IFA is estimated to
be 94%--100% sensitive after 14 days, and that sensitivity is increased if paired samples are tested
(80). The IFA is considered to be the gold standard of serologic testing for rickettsial diseases, and other serologic tests have not
been developed that surpass the sensitivity and specificity of these assays. Testing two sequential serum or plasma
samples together to demonstrate a rising IgG or IgM antibody level is essential to confirm acute infection. Paired
serum specimens taken early (i.e., acute) and later (i.e., convalescent) in the disease course represent the preferred specimens
for evaluation. Typically, these specimens should be taken at least 2--3 weeks apart to examine for a four-fold or
greater increasein antibody titer
(33).
The majority of patients demonstrate increased IgM or IgG titers by the second week of the illness
(patients infected with certain imported rickettsiae might not demonstrate increased titers until 4 weeks after illness onset).
However, patients might lack diagnostic IgG and IgM antibody titers in the first 7 days of illness, a period when the majority
of patients initially seek medical care and laboratory testing is performed. The duration of time that antibodies will
persist after recovery from the infection is variable. In certain persons, high titers of antibodies against
A. phagocytophilum have been observed for 3½ years after the acute illness
(81). For RMSF, IgG and IgM titers increase
concurrently by the second week of illness, and IgM antibodies wane after 3--4 months, whereas IgG titers persist for 7--8 months
(82). The majority of commercial reference laboratories conduct testing for IgG and IgM antibodies.
Cross-reactivity of antigens results in antibody responses that are typically group-specific, but not necessarily
species-specific, after infections with these pathogens. For
example, serologic tests that detect antibodies reactive with
R. rickettsii might have resulted from previous infections with other spotted
fever group rickettsial species. Similarly,
antibodies reactive with E. chaffeensis or
A. phagocytophilum occasionally react with the other ehrlichial species, which might
impede epidemiologic distinction between the ehrlichial infections
(83). Most patients with E. ewingii infections
develop antibodies that react with E. chaffeensis
antigens. Little cross-reactivity of
Rickettsia with Ehrlichia or Anaplasma
speciesexists. Certain serologically confirmed cases of infection thought to be RMSF, HME, or HGA might represent
infections with the other agent or with another antigenically related species. The predominance of
non-R. rickettsii species in tick vectors collected in RMSF-endemic areas suggests that related organisms of undetermined pathogenicity might play
a role in human illness (84). This occurrence is especially true for persons who are infected with rickettsial organisms
from endemic areas outside of the United States.
Nucleic Acid Detection
Amplification of specific DNA by PCR provides a rapid method for detecting TBRD infections. These tests
are available from CDC, certain state health laboratories, and a limited number of research and commercial
laboratories (Box). Conventional PCR tests have no specified standard, and
diagnostic sensitivity and specificity might vary
among individual assays (80). Doxycyline treatment, in particular, can also decrease the sensitivity of PCR
(45). In studies of A. phagocytophilum
infection, PCR was estimated as 60%--70% sensitive
(53), and for diagnosis of infection with
E. chaffeensis, PCR was estimated to be 52%--56% sensitive
(25) to 87% sensitive (85). For RMSF, PCR is
probably more useful for detecting the etiologic agent in a skin biopsy or autopsy tissue specimen than it is in an acute
blood sample because, typically, low numbers of rickettsiae circulate in the blood in the absence of advanced disease
or fulminant infection (18). PCR testing of skin biopsies alone does not offer ideal sensitivity, and a negative result
does not exclude the diagnosis because of focality of vessel involvement. Laboratory confirmation of RMSF in the acute
stage is improved when PCR is used in conjunction with IHC staining. PCR of whole blood specimens is more useful
for confirming HME, HGA, and E. ewingii infection because of the tropism of these pathogens for circulating
WBC. However, no optimal time frame has been established that is ideal for sample collection to ensure the highest
sensitivity for diagnosing ehrlichioses or anaplasmosis. New techniques (e.g., real-time PCR) might offer the
advantages of speed, reproducibility, quantitative capability, and low risk for contamination, compared with conventional PCR
(86).
IHC Staining
Another approach to diagnosing TBRD is immunohistochemical (IHC) staining of antigens in
formalin-fixed, paraffin-embedded biopsy or autopsy tissues. This test can be particularly useful to diagnose fatal TBRD in
those patients for whom diagnostic levels of antibodies have not developed before death. For patients with a rash, IHC
or immunofluorescence staining of a skin biopsy can be a critical diagnostic technique for RMSF. Immunostaining of
skin biopsy specimens has been reported to be 100% specific and 70% sensitive in diagnosing RMSF
(35). This method has been used to diagnose fatal and nonfatal cases of RMSF
(18,87--89). Because rickettsiae might be focally distributed
in tissue, this test might not always detect the agent. Autopsy tissues also are appropriate for evaluation and
include the liver, spleen, lung, heart, kidney, and brain. The IHC method is most useful in documenting the presence of
organisms in patients before initiation of antibiotic therapy or within the first 48 hours after antibiotic therapy has been
initiated. IHC techniques also are available for diagnosing cases of ehrlichioses and anaplasmosis from bone marrow biopsies
and tissue obtained at autopsy of fatal cases, including the spleen, lymph nodes, liver, and lung
(90--92). Immunostaining for spotted fever group rickettsiae,
E. chaffeensis, and A.
phagocytophilum is offered by CDC and certain
university-based hospitals and commercial laboratories in the United States (Box).
Culture
Because the agents that cause TBRD are obligate intracellular pathogens, they must be isolated by using cell
culture techniques that are typically more labor-intensive and time-consuming than serologic, molecular, or IHC
assays. Theoretically, any laboratory capable of performing routine viral isolations might have the expertise to isolate
these pathogens. However, R. rickettsii is classified as a Biosafety Level-3 (BSL-3) agent, and attempts to isolate this agent
should be made only in laboratories equipped to handle BSL-3 pathogens
(93). Laboratories attempting culture of
R. rickettsii bacteria need to comply completely with federal regulations
(42 C.F.R. [2004]) regarding the registration and use
of select agents (93). As a result, culture is rarely used for diagnosis, and other methods (e.g., serology, PCR,
or immunostaining) are used to confirm infection.
The following is a summary of salient features of diagnostic testing:
Blood smear microscopy might reveal presence of morulae in infected leukocytes, which is highly suggestive of
HGA or, less commonly, HME.
Blood smears are not useful to diagnose RMSF.
Examination of paired serum samples obtained 2--3 weeks apart that demonstrate a rise in antibody titer is the
most appropriate approach to confirm TBRD.
Patients usually do not have diagnostic serum antibody titers during the first week of illness; therefore, an
inability to detect antibodies (IgG or IgM) in acute-phase
serum does not exclude TBRD.
Immunohistochemistry of a biopsied skin lesion or
autopsy tissues is useful for RMSF diagnosis in patients for whom
diagnostic titers of antibodies have not yet
developed.
Whole blood specimens might be useful for a PCR confirmation of HME, HGA, and
E. ewingii infection; however, a negative result does not rule out the diagnosis.
Surveillance and Reporting
National reporting requirements are determined collaboratively by the Council of State and Territorial
Epidemiologists and CDC. RMSF, anaplasmosis, and all forms of ehrlichiosis are nationally notifiable diseases. RMSF
became nationally notifiable in 1989 and anaplasmosis and ehrlichiosis, in 1998. When health-care providers identify a potential case
of TBRD, they should notify the local health department. The local health department, in cooperation with the
state health department, can assist the health-care provider in
obtaining appropriate diagnostic testing to confirm
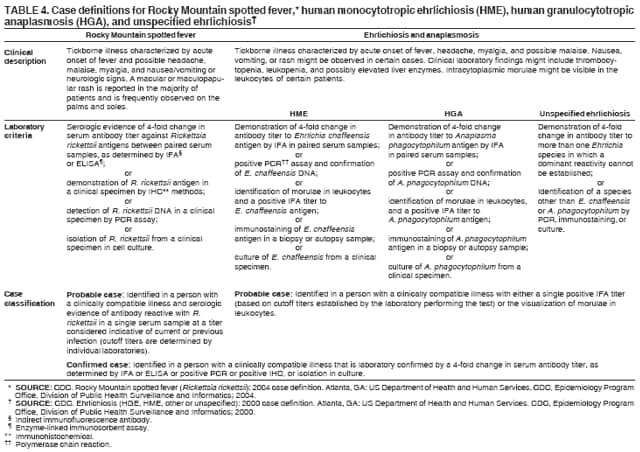
the diagnosis. All confirmed or probable cases of RMSF, HME, HGA, and
E. ewingii infection should be reported to
the state health department. The case definitions for confirmed and probable cases of RMSF, HME, and HGA have
been reported (Table 4; 33,94). Each state health department compiles case reports and submits them to CDC, where
data are compared and disseminated via the MMWR Weekly
and annual Surveillance Summaries.
Since 1981, CDC has collected and analyzed surveillance data on RMSF by using two complementary systems.
States submit reports electronically via the National Electronic Telecommunications System for Surveillance (NETSS) as part
of the National Notifiable Disease Surveillance System. NETSS reports capture diagnosis, date of onset, and
basic demographic and geographic data related to the case. In addition, physicians are encouraged to complete a
standardized case report form (CRF; Appendix) and forward it to the state health
department, where it is compiled with similar reports and forwarded to CDC. The CRF summarizes demographic, epidemiologic, and outcome data that are
not reported in NETSS. Data collected on the CRF are useful in summarizing the epidemiologic characteristics of
disease and focusing on prevention and
treatment.This process includes
examininglesser understood aspects of these
conditions (e.g., the role of immunosuppression as a risk factor for disease; the prevalence of severe outcomes of
infection, including death; and hospitalization trends). In 2001, the form was expanded to include reporting of other
common TBRD, including HGA and HME, in addition to RMSF.
A surveillance system is critical for studying the changing epidemiology of TBRD and for developing effective
prevention strategies and public health education programs. The
detection of a cluster of RMSF cases in a region of Arizona where
the disease was not known to occur and subsequent prevention and control initiatives underscore the vital role of
surveillance and reporting in protecting the public's health. By the end of 2004, the highest number of RMSF cases was
reported to CDC (n = 1,514), suggesting potential increased
activity. However, underreporting of TBRD is probably
common.
The following is a summary of salient features of surveillance and reporting:
RMSF, HME, HGA, and other ehrlichioses are reportable diseases in the United States.
Physicians who identify a potential case of TBRD should notify the local health department, which can assist
with obtaining diagnostic testing to confirm the diagnosis.
Surveillance and reporting of TBRD are key components of public health education and disease prevention efforts.
Prevention
No licensed vaccines for TBRD exist. Avoiding tick bites and promptly removing attached ticks remain the best
disease prevention strategies. Persons should limit their exposure to tick-infested habitats, including wooded or grassy
areas. Persons should walk on cleared trails and avoid brushing against tall grass and other vegetation. This practice
is particularly essential during periods of peak tick activity (i.e., late spring and summer) but should be
observed, regardless of the season. Protective clothing, including a hat, long-sleeved shirts, pants, socks, and closed-toe shoes
are helpful in preventing ticks from reaching the skin and attaching. Wearing light-colored clothing is
preferred because crawling ticks can be seen easily.
Various over-the-counter products containing DEET
(N,N-diethyl-m-toluamide) are available for application
on exposed skin and clothing to repel ticks. The higher the concentration of DEET, the longer the duration of
protection per application. Products with DEET concentrations as low as 10% and those containing 25%--35% concentrations
are considered optimal. No evidence exists that concentrations >50% are more efficacious or provide longer duration
of protection (95). The American Academy of
Pediatrics has recommended that DEET concentrations no greater than
20%--30% should be used for children (96). Products containing permethrin (e.g., permanone) can be used to treat
outer clothing (e.g., shirts and pants) and should not be applied to skin. Permethrin is available commercially as a
spray-on preparation. It should be applied evenly to outer clothing, according to label directions in a
well-ventilated area. Clothing should be allowed to completely dry before being worn. Pre-treated clothing is available and remains effective for
multiple launderings. The use of DEET and permethrin should be considered by persons who enter heavily infested tick
habitats where the risk for being bitten is high and the potential for TBRD infection exists.
Adults entering wooded or grassy areas should inspect themselves and their children frequently for ticks.
Because several hours might elapse before ticks attach and inject pathogens, frequent checks increase the likelihood of
finding ticks before they transmit an infectious agent. The
duration of tick attachment necessary to transmit
rickettsial organisms is substantially variable and has been reported to be as little as 2--10 hours
(97) to 10--20 hours (98) for R.
rickettsii. Limited data exist regarding the interval of transmission after tick attachment for
A. phagocytophilum, but animal studies indicate that 24--48 hours might elapse before pathogen transmission
(99,100). No comparable data exists for E.
chaffeensis. Sites where ticks commonly attach include, but are not limited to, the scalp, waist,
armpits, groin, and under socks and the beltline. Pets should also be checked for ticks because they can carry ticks back to
their homes and human companions. Regular application of ectoparasite control on pets helps to reduce the risk for
human exposure to ticks.
If an attached tick is found, it should be removed by grasping with tweezers or fine-tipped forceps close to the
skin and gently pulling with constant pressure. Folk remedies, including gasoline, kerosene, petroleum jelly, fingernail
polish, or lit matches should never be used to extract ticks
(101). Removing the tick with bare hands should be avoided
because fluids containing infectious organisms might be present in the tick's body and at the wound site. Ticks that have
been removed should not be crushed between the fingers to prevent contamination, and hands should be washed to
avoid potential conjunctival inoculation. The bite wound should then be disinfected.
The following is a summary of salient features of prevention:
Avoid tick bites, which is key to the prevention of TBRD.
Limit exposure to tick habitats, including grassy and wooded areas.
Inspect the body carefully for ticks after being in a tick habitat.
Remove attached ticks immediately by grasping with tweezers close to skin and pulling gently with steady pressure.
TBRD Cases
The following TBRD cases were observed in health-care settings. Information from the cases can be used to reinforce
medical management information related to TBRD
(3,22,102) and are intended to illustrate certain common pitfalls in the
diagnosis and treatment of TBRD. The case reports include a description of the case and salient features that can be considered
when dealing with a potential case of TBRD.
Case 1
In June 2001, a girl aged 5 years was taken to an ED in Missouri with a 3-day history of intermittent fever,
headache, mild nausea, and a sore throat. On physical examination, the patient had a fever of
105°F (40.6ºC) and a
maculopapular rash on her legs, including the soles of her feet.
What should be included in the differential diagnosis?
Possible causes of fever and rash in this child
include meningococcemia, RMSF, HME, enteroviral
infections, Kawasaki disease, drug reactions, and streptococcal disease with exanthem.
What additional information would assist with the diagnosis?
Determine how long the rash has been present and when and where it appeared relative to onset of fever.
The parent should be queried concerning medication use, immunocompromising conditions, and recent
activities that could have led to animal exposures
(including dogs), sick contacts, recent travel, outdoor activities (e.g.,
hiking, camping, and playing in brushy areas or backyard), and real or potential tick exposures.
The parent noticed the rash, which began on the arms and legs, on the same day that the child was taken to
the ED. They did not own a dog, and no history of recent travel out of the local area and no history of a tick bite
were noted, although the parent said that ticks were in the area around their house.
What laboratory tests might be useful?
A CBC, comprehensive metabolic panel, blood culture, and a rapid Streptococcus pharyngitis screen should be performed. An acute serum should be obtained for IgG and IgM antibodies to
R. rickettsii, E. chaffeensis, and
A. phagocytophilum, but subsequent management of the patient should not depend on results. PCR
for E. chaffeensis and A.
phagocytophilum using EDTA whole blood might be useful if these tests are available from
a reference laboratory.
Laboratory results included a WBC count of 8,800
x 109 cells/L (normal: 4.5--11.0 x
109 cells/L), with 5% bands (normal: 0%--5%), 70% neutrophils (normal: 45%--75%), 17% lymphocytes (normal: 16%--46%), and
8% monocytes (normal: 4%--11%). The platelet count was 50 x
109 cells/L (normal: 150--350 x
109 cells/L). Serology results were not available for 3 days.
How does this information assist with the diagnosis?
The time of year for these clinical signs should raise suspicion for TBRD. A normal WBC is
frequently observed in patients with viral infections and with RMSF. Patients with RMSF will commonly develop moderate
to severe thrombocytopenia as the disease progresses,
although a normal platelet count is frequently observed early
in the course of illness. If serologic results are not immediately available, the clinician should not be dissuaded
from initiating therapy if it is clinically indicated.
What actions, including treatment, should be taken?
On the basis of history, clinical signs, geographic location, and time of year, suspicion of a TBRD is
reasonable. An appropriate course of action would include treatment with doxycycline (2.2 mg/kg body weight
administered orally twice daily for a minimum of 5
days) and close follow-up to ascertain clinical response to therapy
while continuing to rule out other possible causes. Appropriate antimicrobial therapy for other suspected etiologies
should be considered until they can be reasonably excluded. For example, certain
experts recommend administering an intramuscular dose of ceftriaxone, pending blood culture results,
because meningococcal disease cannot be reliably distinguished from TBRD on clinical grounds alone. Convalescent-phase serology for RMSF, HGA, and
HME should be performed 2--4 weeks later to confirm the diagnosis.
What preventive measures can the patient and her
family take to prevent infection in the future?
The most effective preventive measure is to 1) limit exposure to ticks during peak periods of activity
(primarily April--September), 2) inspect body and clothing thoroughly for ticks after being in wooded or grassy
areas, 3) remove attached ticks immediately by grasping with tweezers or forceps close to the skin and pulling gently with steady pressure,
and 4) apply insect repellant (e.g., DEET) when exposure to grassy or wooded areas is anticipated.
Case 1 synopsis. This patient's clinical history suggested exposure to ticks, although no definitive indication of a
tick bite was reported. Ticks are small (particularly in their nymphal and larval stages), and bites frequently go
unnoticed because ticks might attach in places that are difficult to observe (e.g., the scalp, axillae, and inguinal regions). Up
to 40% of patients with RMSF report no history of a tick bite
(10,11). Therefore, the clinician should not be
dissuaded from making a diagnosis of RMSF when no report
of a tick bite is made. The clinical signs and laboratory values and
a history that are compatible with tick exposure should guide the diagnosis and therapeutic
actions. Serum samples collected on days 7 and 35 of illness demonstrated rising IgG antibody titers to
R. rickettsii at 32 and 2,048, respectively.
Case 2
In mid-August 2003, a male child aged 14 months was taken to a community health clinic in Arizona after 1 day of
fever 103.7°F
(39.8°C). On physical examination, the child had a maculopapular rash that involved his palms and soles.
On auscultation, abnormal breath sounds were detected in the right lower lung. The parent stated that they had not
traveled out of the local area recently. No one else in the family was ill, and the child was up-to-date on vaccinations.
Chest radiographic evaluation revealed a possible right lower lobe infiltrate. On the basis of clinical and radiographic
findings, pneumonia and roseola infantum were diagnosed. The child was administered an intramuscular injection of ceftriaxone
and sent home with a prescription for oral amoxicillin/clavulanate.
The next day, the child was taken back to the clinic with vomiting and rash that was petechial. His fever was
105.7°F (41°C). He was admitted to the hospital, and antibiotic treatment for pneumonia was continued. On day 3
of hospitalization, the child developed DIC. Remarkable laboratory findings included: WBC count, 16.2 x
109 cells/L (normal: 4.5--11.0 x
109 cells/L); platelet count, 46 x
109 platelets/L (normal: 150--350 x
109 cells/L); aspartate aminotransferase (AST), 291 U/L (normal: 10--40 U/L); and alanine aminotransferase (ALT), 99 U/L (normal:
10--55 U/L). The child's condition worsened, and 7 days after the onset of illness, he died of pulmonary hemorrhage.
Case 2 synopsis. A serum sample collected 5 days before the child's death tested negative by IFA for IgM and
IgG antibodies reactive with R.
rickettsii.However, R.
rickettsii DNA was detected in serum by PCR assay. RMSF can have
a rapid course; 50% of RMSF deaths occur within 9 days
of illness onset (10,11). IgM and IgG antibodies are
typically not detectable before the second week of illness; therefore, serology will be not useful in diagnosing the infection in
its earliest stages. Fever and rash in a young child can be caused by various enteroviruses, human herpesvirus
6, N. meningitidis, measles virus, R.
rickettsii, and E. chaffeensis, among other agents. Common causes of
bacterial pneumonia in a child this age might include
Streptococcus pneumoniae, Staphylococcus aureus, Streptococcus
pyogenes, and, less commonly, M. pneumoniae.
Although this child lived in an area where RMSF is not common (e.g., Arizona),
the diagnosis should not be excluded because of geography. Although RMSF is more common in the south central
and south Atlantic states, it should be considered endemic throughout the contiguous United States
(10). TBRD are seldom treated with the appropriate antibiotic, unless they are suspected. In this context, the majority of broad
spectrum antimicrobials, including penicillins, cephalosporins, aminoglycosides, erythromycin, and sulfa-containing drugs are
not effective against rickettsiae, ehrlichiae, or anaplasmae.
Case 3
In early June 1996, a man aged 52 years who was
HIV-seropositive sought medical care at a hospital in Florida. He had a
4-day history of fever, headache, myalgias, nausea, and vomiting. The patient had been previously healthy, with no known
previous opportunistic infections. An absolute CD4+ lymphocyte count of 164
cells/µl was documented 2 months before this
visit.
Physical examination revealed an acutely ill man; the patient had a fever of
103.5ºF (39.7ºC) and experienced dizziness and
low blood pressure when he stood up (orthostatic
hypotension). He reported that 2 weeks before admission, he had been bitten by
a tick while hiking in central Georgia.
A CBC and chemistry panel and, because of the history of a tick bite, serologic tests for
E. chaffeensis were ordered. Remarkable laboratory findings included hemoglobin 11.5 g/dL (normal: 13--18 g/dL); WBC count,
2.0 x 109 cells/L (normal: 4.5--11.0 x
109 cells/L), with 66% neutrophils (normal: 45%--75%), 18% bands (normal: 0%--5%),
8% lymphocytes (normal: 16%--46%), and 8% monocytes (normal: 4%--11%); and platelet count, 16 x
109 cells/L (normal: 150--350 x
109 cells/L). Peripheral blood smears revealed ehrlichial morulae in 2.5% of all
leukocytes, including monocytes, lymphocytes, atypical
lymphocytes, neutrophils, and metamyelocytes. ALT was
73 U/L (normal: 10--55 U/L), and AST was 358 U/L (normal:
10--40 U/L).
On the basis of laboratory and clinical findings, a diagnosis of HME was made, and intravenous doxycycline (100
mg every 12 hours) was initiated. Despite doxycycline therapy, the patient remained febrile, severely thrombocytopenic,
and continued to have elevated liver enzymes. He developed right lower lobe pneumonia and renal failure and died 6
days after hospitalization.
Case 3 synopsis. Patient sera obtained on days 1 and 5 of hospitalization were negative for IgG and IgM
antibodies reactive with E. chaffeensis. However, the correct diagnosis was revealed on admission by a finding of morulae in
leukocytes, and this diagnosis was subsequently confirmed when
E. chaffeensis DNA was detected by using PCR in whole
blood specimens from the patient, and the agent was isolated in cell culture. HME can be a severe disease, particularly
in immunosuppressed persons. HME does not commonly cause rash in adults; therefore, history of tick
exposure and characteristic leukopenia and thrombocytopenia were most useful in arriving at a diagnosis. Although morulae
were observed in the patient's peripheral blood, microscopy is
generally insensitive, and morulae are reported to be
observed in only 1%--20% of patients with HME
(45,47). Therefore, a diagnosis of HME would need to be confirmed by PCR, serology,
or immunostaining, or culture isolation.
Case 4
In mid-May 1999, a female aged 69 years went to her physician in upstate New York. She had a 3-day history
of nausea, vomiting, fatigue, and fever. She said that her dog had died 2 days earlier after a brief illness characterized
by signs similar to her own. Physical examination revealed no abnormalities. Her temperature was
100.4ºF (38ºC).
What should be included in the differential diagnosis?
Possible diagnoses that should be considered include viral syndrome, foodborne illness, and urinary tract
infection.
What additional information would assist with the diagnosis?
Patient should be queried regarding other signs and symptoms, recent activities and travel, exposure to other
ill persons, foods consumed, and contact with ticks. The patient had no other symptoms to report and
reported no unusual activities or recent travel.
What diagnostic tests, if any, are needed?
Because the patient's symptoms were nonspecific, a CBC should be ordered. Results will not be
available until the next day.
On the basis of the signs present when the patient first went to her physician, she was diagnosed
with gastroenteritis and instructed to return within 24--48 hours, if her symptoms did not improve. The patient
would be contacted regarding her laboratory test
results. The next day, the patient returned with continued
fever and changes in mental status. Her temperature remained at
100.4ºF (38ºC), but she was notably confused
and lethargic. Her physical examination was unremarkable
and did not reveal the presence of a rash.
Laboratory tests obtained on the previous day revealed
a WBC count of 3.8 x 109 cells/L (normal: 4.5--11.0 x
109 cells/L); a platelet count of 99 x
109 cells/L (normal: 150--350 x
109 cells/L); and a hemoglobin concentration of
12.7 g/dL (normal: 12--16 g/dL).
How does this information assist with the diagnosis?
On the basis of the patient's thrombocytopenia, leukopenia, and worsening clinical condition, encephalitis
and sepsis should be included in the differential diagnosis.
What actions, including treatment, should be taken?
On the basis of presenting signs and laboratory tests, the patient was hospitalized and intravenous
levofloxacin therapy was initiated for fever of unknown cause. Blood, urine, and stool cultures were ordered as well as
serologic assays for B. burgdorferi, E.
chaffeensis, and A. phagocytophilum, and PCR for E. chaffeensis and
A.
phagocytophilum.
The patient's temperature returned to normal within 48 hours, her nausea and vomiting resolved, and her
blood counts returned to normal. She was discharged after
3 days. Blood, urine, and stool cultures revealed no
specific pathogens, and serologic assays were negative for
antibodies reactive with B. burgdorferi,
E. chaffeensis, and A.
phagocytophilum.
Case 4 synopsis. IHC staining of tissues from the patient's dog, submitted by the veterinarian to CDC,
demonstrated abundant spotted fever group rickettsial
antigens, and rickettsiae were identified within and around blood vessels
in multiple tissues, including brain and testes. The cause of the dog's illness was identified as RMSF. This information
was communicated to the patient's physician. When the physician contacted the
patient, she reported that her fatigue and headache had persisted after discharge from the hospital. The patient was treated with oral doxycycline, and all
symptoms resolved within 1 week. Subsequent testing of the patient's sera for early and late convalescent-phase antibody
titer confirmed a diagnosis of RMSF. Titers of IgM and IgG antibodies were 1,024 and 512, respectively, on day 17
and declined to 256 and 256, respectively, on day 89 after illness onset. The
patient did not recall a tick bite and had not seen
or removed ticks from her dog, although her dog roamed freely in wooded areas before its illness. Dogs can serve as sentinels
for RMSF in human populations, and infections in canines
have been associated with increased risk for infection in their
owners (22).
Case 5
In May 2001,a man aged 38 years sought medical
attention in Tennessee with complaints of headache, fever,
sore throat, and vomiting. He was treated 3 days previously by his primary care physician who diagnosed pneumonia
and prescribed azithromycin and levofloxacin, but his fevers persisted. He was taken to the ED by his wife, and she said
that he had new onset of confusion. He had no pets or animal exposures. He worked as a construction manager and
was frequently outdoors in wooded areas but did not recall a tick bite.
What should be included in the differential diagnosis?
The initial signs and symptoms were nonspecific, but the patient's confused state raised concern for
possible involvement of the CNS. During the summer months, the differential diagnosis included viral
meningitis (particularly enteroviral), arboviral meningoencephalitis (West Nile virus and others), TTP, and TBRD.
Bacterial meningitis and herpes simplex virus (HSV) encephalitis do not have confined seasonality
but also could cause this presentation. Sepsis and other multisystem illnesses are associated with
encephalopathy, however, so the differential diagnosis
remained broad.
The patient had an oral temperature of
103.4°F (39.7ºC); blood pressure, 100/60 mmHg; and heart rate,
120 beats/minute. The skin examination revealed diffuse erythema with a several scabs on the lower legs. Examination of
the abdomen revealed moderate epigastric tenderness with deep palpation but no rebound tenderness or
organomegaly. Neurologic examination was nonfocal,
except for altered mentation (i.e., Glasgow coma score: 13).
Laboratory testing revealed the following: WBC,
11.9 x 109 cells/L (normal: 4.5--11.0 x
109 cells/L); 84% segmented neutrophils (normal: 45%--75%); 8% band neutrophils (normal: 0%--5%); 3% lymphocytes
(normal: 16%--46%); 5% monocytes (normal: 4%--11%);
platelets, 50 x 109 cells/L (normal: 150--350 x
109 cells/L); total bilirubin, 3.5 mg/dL (normal: 0--1.0 mg/dL); AST, 439
U/L (normal: 10--40 U/L); ALT, 471 U/L (normal:
10--55 U/L); and alkaline phosphatase, 236 U/L (normal: 45--115
U/L). Lumbar puncture revealed a WBC of 0, RBC of 1
with normal glucose of 55 mg/dL and normal protein of 20
mg/dL. Creatinine was elevated at 3.9 mg/dL (normal:
0.6--1.5 mg/dL). Computed tomography scan of the head
did not demonstrate an acute abnormality.
How does the physical examination and laboratory information change the differential diagnosis?
Because of the normal lumbar puncture, meningitis (i.e., viral or bacterial) was a less likely diagnosis.
However, examination of the CSF might be unremarkable in patients with encephalitis. The presence of thrombocytopenia
and elevated transaminases was suggestive of TBRD. Additional considerations included acute cholecystitis, sepsis
(possibly associated with DIC), toxic-shock syndrome (rash with multiple organ failure), and TTP (i.e., acute renal failure
with fever, altered mental status, and thrombocytopenia).
What additional tests should be performed?
Appropriate diagnostic studies should include blood culture, serologic testing for RMSF and HME (and PCR
for these if available), prothrombin time and partial thromboplastin time, examination of the peripheral blood
smear (with particular attention for
schistocytesor intracellular morulae), and ultrasound of the gallbladder to evaluate
for inflammation.
The coagulation studies were within normal limits, and no schistocytes or morulae were observed on
smear. Abdominal ultrasound revealed a normal gallbladder but mild splenomegaly. Therapy was initiated with
ceftriaxone and vancomycin. Approximately 6 hours later, the
patient developed seizures, and acyclovir and doxycycline
were added to the course of medicine to effectively treat
herpesvirus infection and TBRD. A magnetic resonance
imaging scan of the brain was normal, and electroencephalography
revealed nonspecific slowing. Antibodies to R.
rickettsii and E. chaffeensis were not detected
in acute sera. HSV PCR on CSF was negative. Blood cultures did not grow
bacteria. The patient defervesced, and mental status normalized over the next 3 days.
Case 5 synopsis. Serum obtained 31 days after the initial signs and symptoms contained no antibodies
to R. rickettsii but had an IgG titer of 256 to
E. chaffeensis, retrospectively confirming the diagnosis of HME.
Whereas headache is a nearly universal complaint among patients with HME, altered sensorium might be observed in up to
20% of cases (6). Other CNS manifestations include seizures, meningismus, cranial nerve palsies, focal weakness, and coma.
A lymphocytic pleocytosis can be observed in the CSF in approximately 50% of patients with HME who undergo
lumbar puncture (103). Neutrophilic pleocytosis can be observed early in the course of the illness. Neuroimaging studies
are usually normal or nonspecific. TBRD should be included in the differential
diagnosis of patients presenting with clinical evidence of CNS infection or CSF findings suggestive of aseptic meningitis.
Case 6
In July 1994,a man aged 44 years went to see his physician in central Minnesota. He complained of a
1-week history of fever, chills, generalized myalgias, and right temporomandibular joint pain. When he became ill, he
treated himself empirically with ampicillin, which was available at home, for 2 days. Because the patient experienced no
clinical improvement, he sought medical care. The patient worked outdoors and was frequently in wooded areas. Fourteen
days before he went to his physician, he removed two deer ticks that had been
attached to his skin for an unknown period.
Physical examination findings. The patient had a low-grade fever of
100.6ºF (38.1ºC). Examination of heart,
lungs, and abdomen were normal. No lymphadenopathy, hepatosplenomegaly, or skin rash were noted.
Cardiovascular, pulmonary, gastrointestinal, or neurological symptoms were not present. Overall, physical examination
was unremarkable, except for fever.
Laboratory findings. No laboratory evaluations were performed during the visit. A presumptive diagnosis of
acute Lyme disease was made, and empirical treatment with amoxicillin and probenecid was initiated; a 1-week follow-up
visit was scheduled. Five days after the outpatient visit, the patient died suddenly at home. He had complained of
shortness of breath the day before his death.
Case 6 synopsis. Histopathologic examination of the patient's heart revealed widespread transmural myocarditis
with neutrophilic and lymphocytic infiltrates. Postmortem serum specimens were evaluated initially for presumptive
carditis as a result of B. burgdorferi infection. Serum titers of IgG and IgM antibodies to
B. burgdorferi were not detected by ELISA and western blotting. PCR assays of serum and whole blood
for B. burgdorferi also were negative.
However, antibody titers to A. phagocytophilum
(formerly known as E. equi) were significantly elevated at titer >256 by
IFA methods. Detection of DNA extracted by PCR from whole blood and positive IHC staining of cardiac tissue confirmed
a diagnosis of anaplasmosis. Although infection with
A. phagocytophilum was demonstrated in this case, the pathogenesis
of the associated carditis was less clear
(104).
The diagnosis of HGA can be difficult because of the nonspecific nature of the febrile illness frequently observed
when the patient first seeks medical care. In regions where both Lyme disease and HGA are known to occur,
distinguishing between the diseases in the early stages of illness might be difficult. Because treatment should be initiated before
a definitive diagnosis is made, selection of an antimicrobial effective against both rickettsial organisms and
B. burgdorferi (e.g., doxycycline) is recommended. This case also underscores the importance of close follow-up of
patients treated for TBRD on an outpatient basis. Because these diseases can rapidly progress, clinicians should
emphasize to patients the need to return for reevaluation if substantial improvement is not observed within 24--48 hours of initiation
of treatment.
Conclusion
TBRD continue to cause severe illness and death in otherwise healthy adults and children, despite the availability
of low cost, effective antimicrobial therapy. The greatest challenge to clinicians is the difficult diagnostic dilemma posed
by these infections early in their clinical course when antibiotic therapy is most effective.
Early clinical presentations of HME, HGA, RMSF, and
E. ewingii infection include fever, headache, myalgia, and
malaise and are difficult to distinguish from other infectious and noninfectious diseases. Rash is observed frequently in
RMSF, occasionally in HME, and rarely in HGA. TBRD tend to occur seasonally, with the majority of cases occurring during
the warmer spring and summer months. However, cases might develop year-round. A detailed history of recent recreational
or occupational activities might reveal potential exposure to ticks, although the absence of a history of a
recent tick bite should not dissuade clinicians from considering a diagnosis of TBRD.
TBRD can be life-threatening. Severe manifestations of TBRD include prolonged fever, renal failure,
myocarditis, meningoencephalitis, hypotension, acute respiratory distress syndrome, and multiple organ failure. Patients usually do
not have diagnostic serum antibody levels during the first week of illness; therefore, an inability to detect antibodies (IgG or
IgM) in acute-phase serum does not exclude TBRD. Health-care providers should not delay treatment while waiting for a
diagnosis; rather, they should empirically provide treatment if they suspect TBRD. Doxycycline is the drug of choice for the treatment
of presumptive or confirmed TBRD in both adults and children.
Examination of paired serum samples obtained during
acute illness and 2--3 weeks later that demonstrate a rise
in antibody titer is the most appropriate approach to confirm TBRD. Physicians who identify a potential case of
TBRD should notify the local health department, which can assist with obtaining diagnostic testing to confirm the diagnosis.
No licensed vaccines for TBRD are available. Avoiding tick bites and promptly removing attached ticks remain
the best disease prevention strategies.
Acknowledgments
The preparers acknowledge Jim Gathany, CDC, for the tick photographs and Karoyle Colbert, CDC, for creating the tick distribution map.
* Mountain: Montana, Idaho, Wyoming, Colorado, New Mexico, Arizona, Utah, Nevada. East South Central: Kentucky, Tennessee, Alabama, Mississippi.
East North Central: Ohio, Indiana, Illinois, Michigan, Wisconsin. West South Central: Arkansas, Louisiana, Oklahoma, Texas. West North Central:
Minnesota, Iowa, Missouri, North Dakota, South Dakota, Nebraska, Kansas. Pacific: Washington, Oregon, California. New England: Massachusetts, Connecticut,
Rhode Island, New Hampshire. South Atlantic: Delaware, Maryland, Virginia, District of Columbia, West Virginia, North Carolina, South Carolina, Georgia,
Florida. Mid-Atlantic: New York, New Jersey, Pennsylvania.
References
Dumler JS, Barbet AF, Bekker CPJ, et al. Reorganization of genera in the families Rickettsiaceae and Anaplasmataceae in the order
Rickettsiales: unification of some species of Ehrlichia with Anaplasma,
Cowdria with Ehrlichia and
Ehrlichia with Neorickettsia, descriptions of six new
species combinations and designation of Ehrlichia
equi and `HGE agent' as subjective synonyms of Ehrlichia phagocytophila. Int J Syst Evol
Microbiol 2001;51:2145--65.
Kirkland KB, Wilkinson WE, Sexton DJ. Therapeutic delay and mortality in cases of Rocky Mountain spotted fever. Clin Infect
Dis 1995;20:1118--21.
Thorner AR, Walker DH, Petri WA Jr. Rocky Mountain spotted fever. Clin Infect Dis 1998;27:1353--60.
Fishbein DB, Dawson JE, Robinson LE. Human ehrlichiosis in the United States, 1985--1990. Ann Intern Med 1994;120:736--43.
Bakken JS, Krueth J, Wilson-Nordskog C, Tilden RL, Asanovich K, Dumler JS. Clinical and laboratory characteristics of human
granulocytic ehrlichiosis. JAMA 1996;275:199--205.
O'Reilly M, Paddock C, Elchos B, Goddard J, Childs J, Currie M. Physician knowledge of the diagnosis and management of Rocky
Mountain spotted fever---Mississippi, 2002. Ann NY Acad Sci 2003; 990:295--301.
Helmick CG, Bernard KW, D'Angelo LJ. Rocky Mountain spotted fever: clinical, laboratory, and epidemiological features of 262 cases. J
Infect Dis 1984;150:480--8.
Treadwell TA, Holman RC, Clarke MJ, Krebs JW, Paddock CD, Childs JE. Rocky Mountain spotted fever in the United States, 1993--1996.
Am J Trop Med Hyg 2000; 63:21--6.
Dalton MJ, Clarke MJ, Holman RC, et al. National surveillance for Rocky Mountain spotted fever, 1981--1992: epidemiologic summary
and evaluation of risk factors for fatal outcome. Am J Trop Med Hyg 1995;52:405--13.
Gardner SL, Holman RC, Krebs JW, Berkelman R, Childs JE. National surveillance for the human ehrlichioses in the United States,
1997--2002, and proposed methods for evaluation of data quality. Ann NY Acad Sci 2003;990:80--9.
Demma LJ, Holman RC, McQuiston JH, Krebs JW, Swerdlow DL. Epidemiology of human ehrlichiosis and anaplasmosis in the United
States, 2001--2002. Am J Trop Med Hyg 2005;73:400--9.
Marshall GS, Jacobs RF, Schutze GE, et al. Ehrlichia chaffeensis seroprevalence among children in the southeast and south-central
regions of the United States. Arch Pediatr Adolesc Med 2002;156:166--70.
Marshall GS, Stout GG, Jacobs RF, et al. Antibodies reactive to
Rickettsia rickettsii among children living in the southeast and south central
regions of the United States. Arch Pediatr Adolesc Med 2003;157:443--8.
Bustamante ME, Varela G. Una nueva rickettsiosis en Mexico: existencia de la fiebre manchada americana en los estados de Sinaloa y
Sonora. México D.F., México: Revista del Instituto de Salubridad y Enfermedades Tropicales; 1943;4:189--210.
Demma LJ, Traeger MS, Nicholson WL, et al. Rocky Mountain spotted fever from an unexpected tick vector in Arizona. N Engl J
Med 2005;353:587--94.
Ripoll CM, Remondegui CE, Ordonez G, et al. Evidence of rickettsial spotted fever and ehrlichial infections in a subtropical territory of
Jujuy, Argentina. Am J Trop Med Hyg 1999;61:350--4.
Yevich SJ, Sanchez JL, DeFraites RF, et al. Seroepidemiology of infections due to spotted fever group rickettsiae and
Ehrlichia species in military personnel exposed in areas of the United States where such infections are endemic. J Infect Dis 1995;171:1266--73.
Paddock CD, Brenner O, Vaid C, et al. Short report: concurrent Rocky Mountain spotted fever in a dog and its owner. Am J Trop Med
Hyg 2002;66:197--9.
Elchos BN, Goddard J. Implications of presumptive fatal Rocky Mountain spotted fever in two dogs and their owner. J Am Vet Med
Assoc 2003;223:1450--2.
Carpenter CF, Gandhi TK, Kong LK, et al. The incidence of ehrlichial and rickettsial infection in patients with unexplained fever and
recent history of tick bite in central North Carolina. J Infect Dis 1999;180:900--3.
Olano JP, Masters E, Hogrefe W, Walker DH. Human monocytotropic ehrlichiosis, Missouri. Emerg Infect Dis 2003;9:1579--86.
Standaert SM, Dawson JE, Schaffner W, et al. Ehrlichiosis in a golf-oriented retirement community. N Engl J Med 1995;333:420--5.
Belongia EA, Reed KD, Mitchell PD, et al. Tickborne infections as a cause of nonspecific febrile illness in Wisconsin. Clin Infect Dis
2001; 32:1434--9.
Nadelman RB, Horowitz HW, Hsieh T-C, et al. Simultaneous human granulocytic ehrlichiosis and Lyme borreliosis. N Engl J Med
1997;337:27--30.
Buller RS, Arens M, Hmiel SP, et al. Ehrlichia ewingii, a newly recognized agent of human ehrlichiosis. N Engl J Med 1999;341:148--55.
Paddock CD, Folk SM, Shore GM, et al. Infections with
Ehrlichia chaffeensis and Ehrlichia
ewingii in persons coinfected with human immunodeficiency virus. Clin Infect Dis 2001;33:1586--94.
Childs JE, Paddock CD. The ascendancy of Amblyomma americanum as a vector of pathogens affecting humans in the United States. Annu
Rev Entomol 2003;48:307--37.
Breitschwerdt EB, Hegarty BC, Hancock SI. Sequential evaluation of dogs naturally infected with
Ehrlichia canis, Ehrlichia
chaffeensis, Ehrlichia equi, Ehrlichia
ewingii, or Bartonella vinsonii. J Clin Microbiol 1998;36:2645--51.
CDC. Ehrlichiosis (HGE, HME, other or unspecified): 2000 case definition. Atlanta, GA: US Department and Health and Human
Services, CDC, Division of Public Health Surveillance and Informatics; 2004. Available at
http://www.cdc.gov/epo/dphsi/casedef/ehrlichiosis_current.htm.
Jensenius M, Fournier P-E, Raoult D. Tick-borne rickettsioses in international travellers. Int J Infect Dis 2004;8:139--46.
McDonald JC, MacLean JD, McDade JE. Imported rickettsial disease: clinical and epidemiological features. Am J Med 1988;85: 799--805.
Paddock CD, Sumner JW, Comer JA, et al. Rickettsia parkeri: a newly recognized cause of spotted fever rickettsiosis in the United States.
Clin Infect Dis 2004;38:805--11.
McCall CL, Curns AT, Rotz LD, et al. Fort Chaffee revisited: the epidemiology of tick-borne rickettsial and ehrlichial diseases at a natural
focus. Vector Borne Zoonotic Dis 2001;1:119--27.
Davis AE, Bradford WD. Abdominal pain resembling acute appendicitis in Rocky Mountain spotted fever. JAMA 1982;247:2811--2.
Hattwick MAW, Retailliau H, O'Brien RJ, Slutzker M, Fontaine RE, Hanson B. Fatal Rocky Mountain spotted fever. JAMA 1978;
240:1499--503.
Sexton DJ, Corey GR. Rocky Mountain "spotless" and "almost spotless" fever: a wolf in sheep's clothing. Clin Infect Dis 1992;15: 439--48.
Bakken JS, Dumler JS. Ehrlichiosis and anaplasmosis. Infect Med 2004;21:433--51.
Jacobs RF, Schutze GE. Ehrlichiosis in children. J Pediatr 1997;131:184--92.
Fichtenbaum CJ, Peterson LR, Weil GJ. Ehrlichiosis presenting as a life-threatening illness with features of the toxic shock syndrome. Am J
Med 1993;95:351--7.
Harkess JR. Ehrlichiosis. Infect Dis Clin North Amer 1991;5:37--51.
Walker DH, Raoult D. Rickettsia
rickettsii and other spotted fever group rickettsiae (Rocky Mountain spotted fever and other spotted fevers).
In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett's principles and practice of infectious diseases. 6th ed. Philadelphia,
PA: Churchill Livingstone; 2005:2287--95.
Weber D, Cohen MS, Rutala WA. The acutely ill patient with fever and rash. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas,
and Bennett's principles and practice of infectious diseases. 6th ed. Philadelphia, PA: Churchill Livingstone; 2005:729--46.
Fishbein DB, Dennis DT. Tick-borne disease---a growing risk. N Engl J Med 1995;333:452--3.
Bakken JS, Aguero-Rosenfeld ME, Tilden RL, et al. Serial measurements of hematologic counts during the active phase of human
granulocytic ehrlichiosis. Clin Infect Dis 2001;32:862--70.
Kaplowitz LG, Fischer JJ, Sparling PF. Rocky Mountain spotted fever: a clinical dilemma. In: Remington JB, Swartz HN, eds. Current
clinical topics in infectious diseases. Vol. 2. New York, NY: McGraw-Hill; 1981:89--108.
Lochary ME, Lockhart PB, Williams WT Jr. Doxycycline and staining of permanent teeth. Pediatr Infec Dis J 1998;17:429--31.
Grossman ER, Walchek A, Freedman H, Flanagan C. Tetracyclines and permanent teeth: the relation between dose and tooth color.
Pediatr 1971;47:567--70.
Abramson JS, Givner LB. Should tetracycline be contraindicated for treatment of presumed Rocky Mountain spotted fever in children less than
9 years of age? Pediatrics 1990;86:123--4.
Wallman IS, Hilton HG. Teeth pigmented by tetracycline. Lancet 1962;1:827--9.
Weyman J, Porteous JR. Tetracycline discolouration and bands in human teeth. Brit Dent J 1963;115:499.
American Academy of Pediatrics.
Ehrlichia infections (human ehrlichioses). In: Pickering LK, Baker CJ, Overturf GD, Prober CG, eds. 2003
Red Book: report of the Committee on Infectious Diseases, 26th ed. Elk Grove Village, Illinois: American Academy of Pediatrics, Committee
on Infectious Diseases; 2003:266--9.
American Academy of Pediatrics. Rocky Mountain spotted fever. In: Pickering LK, Baker CJ, Overturf GD, Prober CG, eds. 2003 Red
Book: report of the Committee on Infectious Diseases. 26th ed. Elk Grove Village, Illinois: American Academy of Pediatrics; 2003:532--4.
Holman RC, Paddock CD, Curns AT, Krebs JW, McQuiston JH, Childs JE. Analysis of risk factors for fatal Rocky Mountain spotted
fever: evidence for superiority of tetracyclines for therapy. J Infect Dis 2001;184:1437--44.
Brouqui P, Raoult D. In vitro susceptibility of the newly recognized agent of ehrlichiosis in humans,
Ehrlichia chaffeensis. Antimicrob Agents Chemother 1992;36:2799--803.
Klein MB, Nelson CM, Goodman JL. Antibiotic susceptibility of the newly cultivated agent of human granulocytic ehrlichiosis: promising
activity of quinolones and rifamycins. Antimicrob Agents Chemother 1997;41:76--9.
Burgdorfer W. Rocky Mountain spotted fever. In: Hubbert WT, McCullough WF, Schnurrenberger PR, eds. Diseases transmitted from animals
to man. 6th ed. Springfield, IL: Charles C. Thomas; 1975:396--404.
Niebylski ML, Peacock MG, Schwan TG. Lethal effect of
Rickettsia rickettsii on its tick vector
(Dermacentor andersoni). Appl Environ
Microbiol 1999;65:773--8.
Pretzman C, Daugherty N, Poetter K, Ralph D. The distribution and dynamics of
Rickettsia in the tick population of Ohio. Ann NY Acad
Sci 1990;590:227--36.
Pancholi P, Kolbert CP, Mitchell PD, et al.
Ixodes dammini as a potential vector of human granulocytic ehrlichiosis. J Infect Dis
1995;172:1007--12.
Magnarelli LA, Stafford KC III, Mather TN, Yeh M-T, Horn KD, Dumler JS. Hemocytic
Rickettsia-like organisms in ticks: serologic
reactivity with antisera to Ehrlichiae and detection of DNA of agent of human granulocytic ehrlichiosis by PCR. J Clin Microbiol 1995;33:2710--4.
Kenyon RH, Williams RG, Oster CN, Pedersen CE Jr. Prophylactic treatment of Rocky Mountain spotted fever. J Clin Microbiol 1978;8:102--4.
Paddock CD, Holman RC, Krebs JW, Childs JE. Assessing the magnitude of fatal Rocky Mountain spotted fever in the United States:
comparison of two national data sources. Am J Trop Med Hyg 2002;67:349--54.
Walker DH, Hawkins HK, Hudson P. Fulminant Rocky Mountain spotted fever: its pathologic characteristics associated with
glucose-6-phosphate dehydrogenase deficiency. Arch Pathol Lab Med 1983;107:121--5.
Brouqui P, Bacellar F, Baranton G, et al. Guidelines for the diagnosis of tick-borne bacterial diseases in Europe. Clin Microbiol Infect
Dis 2004;10:1108--32.
Bakken JS, Haller I, Riddell D, Walls JJ, Dumler JS. The serological response of patients infected with the agent of human
granulocytic ehrlichiosis. Clin Infect Dis 2002;34:22--7.
Clements ML, Dumler JS, Fiset P, Wisseman CL Jr, Snyder MJ, Levine MM. Serodiagnosis of Rocky Mountain spotted fever: comparison of
IgM and IgG enzyme-linked immunosorbent assays and indirect fluorescent antibody test. J Infect Dis 1983;148:876--80.
Comer JA, Nicholson WL, Olson JG, Childs JE. Serologic testing for human granulocytic ehrlichiosis at a national referral center. J
Clin Microbiol 1999;37:558--64.
Ammerman NC, Swanson KI, Anderson JM, et al. Spotted-fever group
Rickettsia in Dermacentor variabilis, Maryland. Emerg Infect
Dis 2004;10:1478--81.
Everett ED, Evans KA, Henry RB, McDonald G. Human ehrlichiosis in adults after tick exposure: diagnosis using polymerase chain reaction.
Ann Intern Med 1994;120:730--5.
Fenollar F, Raoult D. Molecular genetic methods for the diagnosis of fastidious microorganisms. APMIS 2004;112:785--807.
Dumler JS, Gage WR, Pettis GL, Azad AF, Kuhadja FP. Rapid immunoperoxidase demonstration of
Rickettsia rickettsii in fixed cutaneous
specimens from patients with Rocky Mountain spotted fever. Am J Clin Pathol 1990;93:410--4.
Walker DH, Cain BG, Olmstead PM. Laboratory diagnosis of Rocky Mountain spotted fever by immunofluorescent demonstration
of Rickettsia rickettsii in cutaneous lesions. Am J Clin Pathol 1978;69:619--23.
Procop GW, Burchette JL Jr, Howell DN, Sexton DJ. Immunoperoxidase and immunofluorescent staining of
Rickettsia rickettsii in skin biopsies: a comparative study. Arch Pathol Lab Med 1997;121:894--9.
Dawson JE, Paddock CD, Warner CK, et al. Tissue diagnosis of Ehrlichia chaffeensis in patients with fatal ehrlichiosis by use
of immunohistochemistry, in situ hybridization, and polymerase chain reaction. Am J Trop Med Hyg 2001;65:603--9.
Marty AM, Dumler JS, Imes G, Brusman HP, Smrkovski LL, Frisman DM. Ehrlichiosis mimicking thrombotic thrombocytopenic purpura.
A case report and pathological correlation. Hum Pathol 1995;26:920--5.
Dumler JS, Dawson JE, Walker DH. Human ehrlichiosis: hematopathology and immunohistologic detection of
Ehrlichia chaffeensis. Hum Pathol 1993;24:391--6.
US Department of Health and Human Services. Possession, use, and transfer of select agents and toxins; final rule, 42 CFR, Parts 72 and
73. Federal Register 2005;70(52):13294--325.
CDC. Rocky Mountain spotted fever
(Rickettsia rickettsii): 2004 case definition. Atlanta, GA: US Department and Health and Human
Services, CDC, Division of Public Health Surveillance and Informatics; 2004. Available at
http://www.cdc.gov/epo/dphsi/casedef/rockycurrent.htm.
Fradin MS, Day JF. Comparative efficacy of insect repellents against mosquito bites. N Engl J Med 2002;347:13--8.
American Academy of Pediatrics. International Travel. In: Pickering LK, Baker CJ, Overturf GD, Prober CG, eds. 2003 Red Book: report of
the Committee on Infectious Diseases. 26th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2003:93--8.
Moore JJ. Time relationships of the wood-tick in the transmission of Rocky Mountain spotted fever. J Infect Dis 1911;8:339--47.
Spencer RR, Parker RR. Rocky Mountain spotted fever: infectivity of fasting and recently fed ticks. Public Health Rep 1923;38:333--9.
Katavolos P, Armstrong PM, Dawson JE, Telford SR III. Duration of tick attachment required for transmission of granulocytic ehrlichiosis.
J Infect Dis 1998;177:1422--5.
des Vignes F, Piesman J, Heffernan R, Schulze TL, Stafford KC III, Fish D. Effect of tick removal on transmission of
Borrelia burgdorferi and Ehrlichia phagocytophila by
Ixodes scapularis nymphs J Infect Dis 2001;183:773--8.
Needham GR. Evaluation of five popular methods of tick removal. Pediatrics 1985;75:997--1002.
Masters EJ, Olson GS, Weiner SJ, Paddock CD. Rocky Mountain spotted fever: a clinician's dilemma. Arch Intern Med 2003;163: 769--74.
Ratnasamy N, Everett ED, Roland WE, McDonald G, Caldwell CW. Central nervous system manifestations of human ehrlichiosis. Clin Infect
Dis 1996;23:314--9.
Jahangir A, Kolbert C, Edwards W, Mitchell P, Dumler JS, Persing DH. Fatal pancarditis associated with human granulocytic ehrlichiosis in a
44-year-old man. Clin Infect Dis 1998;27:1424--7.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].