Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Indicators for Occupational Health Surveillance
Prepared by
Catherine Thomsen, MPH1
Jacquelyn McClain, MPH2
Kenneth Rosenman, MD3
Letitia Davis, ScD4
1Oregon Department of Human Services, Portland, Oregon
2McKing Consulting, Atlanta, Georgia
3Michigan State University, East Lansing, Michigan
4Massachusetts Department of Public Health, Boston, Massachusetts
In collaboration with
CDC and the Council of State and Territorial Epidemiologists, Atlanta, Georgia
The material in this report originated through a cooperative agreement between the National Institute for Occupational Safety and Health,
John Howard, MD, Director; the Division of Surveillance, Hazard Evaluations, and Field Studies, Terri Schnorr, PhD, Director; and the Council of State
and Territorial Epidemiologists.
Corresponding preparer: Amy V. Patel, MPH, Council of State and Territorial Epidemiologists, 2872 Woodcock Blvd., Suite 303, Atlanta, GA
30341. Telephone: 770-458-3811; Fax: 770-458-8516; E-mail: [email protected].
Summary
Each year, millions of the estimated 140 million U.S. workers are injured on the job or become ill from exposure to hazards
at work. These work-related injuries and illnesses result in substantial human and economic costs for workers, employers, and
society; estimated direct and indirect costs of work-related injuries and illnesses are approximately $170 billion annually. In 1998,
the Council of State and Territorial Epidemiologists (CSTE) and CDC's National Institute for Occupational Safety and
Health (NIOSH) convened a work group that identified priority occupational health conditions to be placed under
surveillance, addressed cross-cutting surveillance concerns, and made recommendations regarding the role of states in a
comprehensive nationwide surveillance system for work-related disease, injuries, and hazards. CSTE recommendations led to the generation
of 19 occupational health indicators (OHIs) and one Employment Demographic Profile, which were developed during
2001--2003. The OHIs complement other guidelines for state-based occupational health surveillance to address overall state and national
goals to improve public health. These OHIs are intended to help states build occupational health capacity by providing them with
tools to collect and generate important, basic information concerning the occupational health status of the state population and
to identify areas in which to focus prevention efforts. In 2005, CSTE released a report compiling OHI data from 13 states.
NIOSH provides funding for the OHIs because they are now a required component of state-based cooperative agreements for
occupational health surveillance. This report introduces the OHIs and describes CSTE's approach to developing this new occupational
health surveillance tool.
Introduction
Approximately 140 million persons are employed in the United States
(1). Every year, millions of these workers
are injured on the job or become ill as a result of exposure to safety and health hazards at
work. These injuries and illnesses result in substantial human and economic costs not only for workers and employers but also for society. In 2003,
workers' compensation (WC) insurance claims cost approximately $55 billion
(2). Estimated direct and indirect costs of
work-related injuries and illnesses are approximately $170 billion annually
(3).
Public health surveillance is vital to preventing occupational diseases, injuries, and fatalities
(4). Surveillance data are needed to determine the magnitude of the problem of work-related injuries and illnesses, identify workers at greatest risk,
and establish prevention priorities. Data are also necessary to measure the effectiveness of prevention activities and to
identify workplace health and safety problems that need further investigation. Although surveillance of occupational diseases
and injuries in the United States has improved substantially during the last decade, it remains inadequate. The only
current nationwide surveillance system is for fatal occupational injuries, and surveillance of occupational illnesses and
nonfatal occupational injuries is limited and fragmented.
State health agencies play a central role in public health surveillance. However, national statistics on occupational
injuries and illnesses have been collected primarily outside of the public health infrastructure and rely nearly entirely on data
reported by employers. State health agencies that have access to various public health data systems are uniquely positioned to 1)
provide critical data on occupational diseases, 2) generate information necessary to evaluate the conventional occupational injury
data sources, 3) link surveillance findings with intervention efforts, and 4) integrate occupational health into mainstream
public health (5).
Occupational Health Indicators
In 1998, the Council of State and Territorial Epidemiologists (CSTE), in association with CDC's National Institute
for Occupational Safety and Health (NIOSH), convened the Occupational Health Surveillance Work Group (Work Group)
to recommend state-based surveillance activities through 2010. The Work Group identified priority occupational
health conditions to be placed under surveillance, addressed surveillance concerns that are common to more than one
specific condition, and offered recommendations regarding the role of states in a nationwide comprehensive surveillance system
for work-related diseases, injuries, and hazards
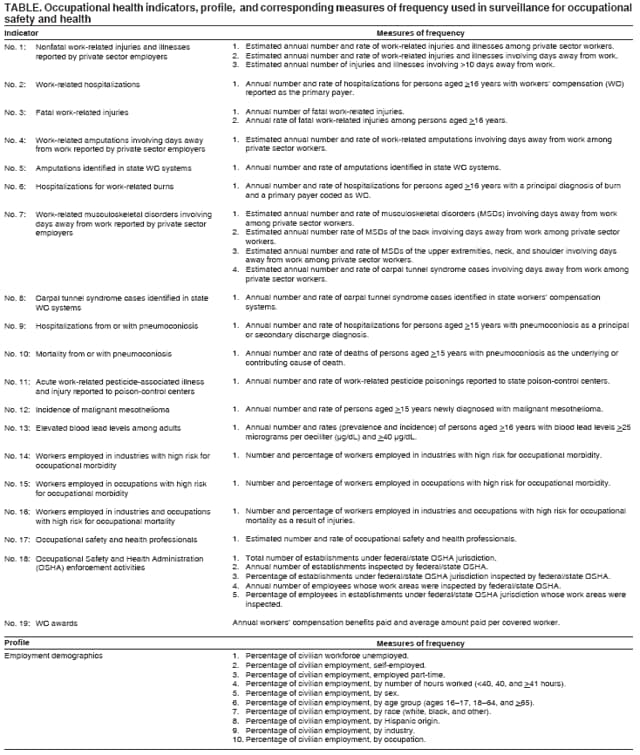
(5). During 2001--2003, the Work Group developed 19 occupational
health indicators and one employment demographic profile recommended for use by the states (Table). These OHIs are intended
to complement other guidelines for state-based surveillance of occupational injuries and illnesses
(5--7) as part of overall state and national goals to improve public health
(8).
In selecting the indicators, the Work Group considered the following criteria:
Availability of easily obtainable statewide
data.The ability to use existing data available in the majority of states
was considered critical for developing indicators. Although certain states might have access to other sources of data
for occupational health surveillance, these OHIs represent a core or minimum set of indicators.
Public health importance of the occupational health effect or exposure to be measured.
Factors considered in determining public health importance included the
extent of the effect or exposure, severity of the health
effect, economicimpact, emergent status of the condition, and level of public concern.
Potential for intervention activities.
Indicators should be used to affect program and policy development at the
state level to protect worker safety and health.
The OHIs were piloted among 13 states by using data from 2000, during which the OHI definitions were refined and
a technical guidance document for states implementing the OHIs was developed
(6).The results of the pilot tests are
detailed in CSTE's 2005 report, Putting Data to Work:
Occupational Health Indicators from Thirteen Pilot States for 2000
(9).
The Work Group has acknowledged limitations in the
design of these OHIs. The underlying data sources
were developed for purposes other than public health surveillance. In addition, substantial variability in source data
frequently occurs among the states. Because of these limitations, caution is advised when interpreting the OHIs. Factors affecting
quality and comparability of state OHI data include
underreporting of occupational injuries and illnesses;
variability in recognition by health-care providers of the occupational etiology of injuries and illnesses;
difficulties in attributing diseases with long latency (e.g., silicosis) or from multifactorial causes (e.g., lung cancer)
to occupational exposure(s);
exclusion of special populations from certain data sources (e.g., persons self-employed or in the military);
injury, illness, and death coding errors;
state-specific differences in structure of administrative databases used for surveillance (e.g., WC and hospital
discharge data).
Data Sources
Data for the OHIs are derived from multiple sources.
Death certificates. All states send death certificate data to the National Vital Statistics System in CDC's National
Center for Health Statistics. The cause-of-death section on the certificate contains the contributing and underlying causes
of death. For injury-related deaths, all state death certificates include a query concerning whether the incident occurred
at work.
Cancer registries. Data on cancer incidence are centralized in registries in all except five states that collect data
from multiple sources, including hospitals and laboratories. The North American Association of Central Cancer Registries
has standards for the operation of registries; however, not all cancer registries meet these standards. Reporting
typically includes in situ or malignant neoplasms, but slight variations exist among states.
State hospital discharge data.
Nearly all acute-care hospitals participate in mandatory or voluntary systems for
compiling discharge data at the state level.The majority of hospital medical records are maintained electronically and
contain standard demographics, diagnoses, and billing information. Although these data sets do not include explicit
information concerning work-relatedness of the health conditions for which a patient is hospitalized, the designation of WC as
the expected primary payer is a suitable proxy. For several conditions, the diagnoses might indicate work-relatedness
(10).
State WC systems. WC is a no-fault insurance system designed to limit the legal liability of employers
while compensating workers who sustain work-related injuries or illnesses. All states have WC systems, and employers in
all states, except in Texas, are required to provide insurance for employees. Separate federal systems exist for certain
groups (e.g., federal workers, and longshore and harbor workers). States' WC claim coding systems, eligibility,
reimbursement, and other regulations differ substantially. Therefore, OHIs in which WC data are used can be used to monitor
trends within states over time but should not be used to compare states.
Occupational safety and health professionals.
Membership in occupational safety and health
professional associations reflects the availability of resources to prevent occupational injuries and illnesses. However, membership
has multiple limitations, including 1) member addresses might not represent work locations, 2) membership rolls
might include retired occupational health professionals, and 3) certain occupational health professionals might not be
members of these organizations.
Survey of occupational injuries and illnesses.
The Bureau of Labor Statistics (BLS) Annual Survey of
Occupational Injuries and Illnesses provides national and state level estimates of the numbers and rates of work-related injuries
and illnesses. In a nationwide sample, employers are asked questions concerning work-related injuries and illnesses.
Although survey data are detailed, occupational diseases are not well documented, and evidence suggests that injuries
are underreported (11--13). The national estimates
exclude public sector workers, self-employed persons, household
workers, and workers on small farms.
Census of fatal occupational injuries.
The BLS Census of Fatal Occupational Injuries (CFOI) includes
work-related fatalities resulting from unintentional and intentional injuries. CFOI uses multiple data sources to
identify, document, and verify work-related injury deaths. Therefore, CFOI is considered a nearly complete ascertainment of
work-related injury deaths (14).
Poison-control centers. Nearly all U.S. poison-control centers (PCCs) submit real-time data to the American
Association of Poison Control Centers for inclusion in its Toxic Exposure Surveillance System
(15).PCCs receive telephone
calls concerning actual or potential exposures to substances. Although PCCs record whether a call is work-related, the
call might be miscoded or not completed. In addition, health-care workers with experience in managing
work-related poisoning might be less likely than other health-care workers to use PCCs. Therefore, underreporting might vary by
state, according to the experience and expertise of health-care workers and by the level of underused PCC services.
Adult blood lead epidemiology and surveillance.
The Adult Blood Lead Epidemiology and Surveillance
(ABLES) system is a state-based program funded by NIOSH. Surveillance of elevated blood lead levels identifies industries
and occupations in which workers are exposed to lead. The U.S. Department of Labor Occupational Safety and
Health Administration (OSHA) mandates blood lead level testing of persons working when airborne lead exceeds a certain
level. However, ABLES does not capture persons who have been exposed to lead and whose employers do not comply
with OSHA's biologic monitoring requirements nor does it capture persons who have been tested by laboratories that do
not comply with the reporting requirement. In addition, the threshold reported varies from state-to-state, and not all
states receive ABLES funding; therefore, national data do not represent all states.
OSHA integrated management information system. OSHA and state agencies conduct worksite inspections
to determine compliance with health and safety standards. Inspection data are maintained in the Integrated
Management Information System (IMIS), including the type of inspection, reason for inspection, inspection date, state, and
worksite type and number of employees. The number of unique establishments inspected (and therefore unique workers affected)
is difficult to quantify because IMIS entries are listed by inspections rather than by
establishment. Because IMIS is an administrative database, the data are updated with each subsequent inspection.
The following data sources are used to quantify the appropriate population at risk (i.e., denominators) for the calculation
of rates:
U.S. Census. The Census Bureau takes the census of the entire United States during years that end in zero. In the
2000 census, the long form sent to approximately one in six households was used to obtain information concerning labor
force status, place of employment, occupation, industry, work status, and income. After a debate concerning undercounting
the population, the Census Bureau performed a coverage measurement survey and decided not to adjust the 2000
census.
County business patterns. The Census Bureau annually produces County Business Patterns (CBP) to provide
economic data by industry. CBP counts the number of
employees in the primary industry of an establishment. CBP data include
the number of establishments, employment, and payroll for each county. Data do not include self-employed persons;
persons working in private households, on farms, and on railroads. In addition, the data do not include the majority of
federal, state, and local government employees. Each year, CBP quantifies the number of full- and part-time employees
on company payrolls for the week that includes March 12th.
Current population survey. The Census Bureau conducts
theCurrent Population Survey (CPS) for BLS. The CPS is
a monthly survey of approximately 60,000 households that represent the civilian,
noninstitutionalized U.S. population and collects information concerning demographics, employment status, hours worked, and the industry and occupation
of each household member aged >15 years. In addition, the CPS data provide statistics that represent where persons
live (not where they work) and undercount persons who have no permanent address or are migratory.
National Academy of Social Insurance (NASI). NASI is a nonprofit, nonpartisan organization dedicated to the study
of social insurance programs (e.g., WC). NASI estimates
benefits, coverage, costs, and the number of covered workers,
by using state unemployment insurance data. WC frequently awards payments that are disbursed over time; therefore,
awards do not reflect the full cost of injuries and illnesses accurately within a given year. State WC coverage and systems
vary from state-to-state, so comparisons are problematic.
Quarterly census of employment and wages.
The BLS Quarterly Census of Employment and Wages (QCEW)
provides a comprehensive tabulation of employment and wage information. Employment is calculated for the number of
workers covered by state unemployment insurance laws during the month. QCEW excludes persons in the military,
self-employed persons, private household workers, and railroad workers. QCEW reports industry for the state, county, and
metropolitan levels as long as confidentiality can be maintained.
Conclusion
The OHIs are intended to help states build capacity for occupational health surveillance by providing them with tools
to generate vital basic information concerning the occupational health status of the state population. Because multiple states
do not yet have adequate occupational health surveillance programs, these OHIs provide an essential mechanism by which
states can learn to use and apply available occupational health data. OHI data will be most useful when multiple years of data
are available to highlight trends within each state. States and the nation can use these OHIs to measure the burden
of occupational injury and illness, prioritize state
occupational health needs, target resources, and measure progress in
preventing work-related diseases and injuries. Additional
states are encouraged to join this initiative. NIOSH provides funding for
the OHIs because they are now required as a component of state-based cooperative agreements for
occupational health surveillance (16). CSTE will also continue to work with NIOSH and states to implement the OHIs by periodically
publishing state and national OHI data. Based on evaluation of the OHIs and changes in data sources and public health priorities,
CSTE might add, modify, or delete OHIs in the future.
The OHIs are a critical part of a larger CSTE initiative to develop public health surveillance indicators across program
areas for states to use in generating a comprehensive picture of the populations' public health status. Recommended indicators
also
have been developed for injury (17) and chronic disease
(18) surveillance, and the OHIs are serving as a model
for environmental public health indicators
(19) currently under development. Detailed information concerning the OHIs
are available at http://www.cste.org.
References
Bureau of Labor Statistics. Employment situation summary. Washington, DC: US Department of Labor, Bureau of Labor Statistics; 2006.
Available at http://www.bls.gov/news.release/empsit.nr0.htm.
National Academy of Social Insurance. Workers' compensation: benefits, coverage, and costs, 2003. Washington, DC: National Academy of
Social Insurance; 2005. Available at
http://www.nasi.org/usr_doc/NASI_Workers_Comp_Report.pdf.
Leigh JP, Markowitz SB, Fahs M, Shin C, Landrigan PJ. Occupational injury and illnesses in the United States: estimates of costs, morbidity
and mortality. Arch Intern Med 1997;157:1557--68.
CDC. NIOSH safety and health topic: surveillance. Atlanta, GA: US Department of Health and Human Services, CDC, National Institute
for Occupational Safety and Health; 2006. Available at
http://www.cdc.gov/niosh/topics/surveillance.
Council of State and Territorial Epidemiologists. The role of the states in a nationwide, comprehensive surveillance system for work-related
diseases, injuries and hazards: a report from NIOSH--States Surveillance Planning Work Group. Atlanta, GA: Council of State and
Territorial Epidemiologists; 2001. Available at
http://www.cste.org/pdffiles/FINREP.pdf.
Council of State and Territorial Epidemiologists. Occupational health indicators: a guide for tracking occupational conditions and
determinants. Atlanta, GA: Council of State and Territorial Epidemiologists; 2006. Available at
http://www.cste.org/pdffiles/Revised%20Indicators_12.14.04.pdf.
CDC. Guidelines: minimum and comprehensive state-based activities in occupational safety and health. Cincinnati, OH: US Department of
Health and Human Services, CDC, National Institute for Occupational Safety and Health; 1995. (DHHS [NIOSH] publication no. 95-107). Available
at http://www.cdc.gov/niosh/pdfs/95-107.pdf.
CDC. About CDC's health protection goals. Atlanta, GA: US Department of Health and Human Services, CDC; 2006. Available at
http://www.cdc.gov/about/goals/goals.htm.
Council of State and Territorial Epidemiologists. Putting data to work: occupational health indicators from thirteen pilot states for 2000.
Atlanta, GA: Council of State and Territorial Epidemiologists; 2005. Available at
http://www.cste.org/pdffiles/newpdffiles/CSTE_OHI.pdf.
Sorock GS, Smith E, Hall N. An evaluation of New Jersey's hospital discharge database for surveillance of severe occupational injuries. Am J
Ind Med 1993;23:427--37.
Rosenman KD, Kalush A, Reilly MJ, Gardiner JC, Reeves M, Luo Z. How much work-related injury and illness is missed by the current
national surveillance system? J Occup Environ Med 2006;48:357--65.
Azaroff LS, Levenstein C, Wegman DH. Occupational injury and illness surveillance: conceptual filters explain underreporting. Am J Public
Health 2002;92:1421--9.
Conway H, Svenson J. Occupational injury and illness rates,
1992--96: why they fell. Monthly Labor Review 1998;121:36--58.
Bureau of Labor Statistics. National census of fatal occupational injuries in 2004. Washington, DC: US Department of Labor, Bureau of
Labor Statistics, Safety and Health Statistics Program; 2005. Available at
http://www.bls.gov/news.release/pdf/cfoi.pdf.
Watson WA, Litovitz TL, Rodgers GC Jr, et al. 2004 Annual report of the American Association of Poison Control Centers Toxic
Exposure Surveillance System. Washington, DC: American Association of Poison Control Centers; 2005. Available at
http://www.poison.org/prevent/documents/TESS%20Annual%20Report%202004.pdf.
CDC. NIOSH state-based occupational safety and health surveillance. Bethesda, MD: US Department of Health and Human Services,
National Institutes of Health; 2006. NIOSH publication no. PAR-04-106. Available at
http://grants.nih.gov/grants/guide/pa-files/PAR-04-106.html.
Davies M, Connolly A, Horan J. State Injury Indicators Report. Atlanta, GA: US Department of Health and Human Services, CDC,
National Center for Injury Prevention and Control; 2001.
Council of State and Territorial Epidemiologists. The State Environmental Health Indicators Collaborative (SEHIC). Atlanta, GA: Council of
State and Territorial Epidemiologists; 2004.Available at
http://www.cste.org/pdffiles/2006/AboutSEHICforCSTE525.pdf.
Occupational Health Indicators Working Group, May 2006
Henry Anderson, MD, Wisconsin Department of Health and Family Services, Madison, Wisconsin; Carrie Breton, MPH, Massachusetts Department
of Public Health, Boston, Massachusetts; David Bonauto, MD, Washington Department of Labor and Industries, Olympia, Washington; Geoffrey
Calvert, MD, National Institute for Occupational Safety and Health, CDC; Robert Castellan, MD, National Institute for Occupational Safety and
Health, CDC; Dawn Castillo, MPH, National Institute for Occupational Safety and Health, CDC; Letitia Davis, ScD, Massachusetts Department of
Public Health, Boston, Massachusetts; Kitty Gelberg, PhD, New York State Department of Health, Troy, New York; Robert Harrison, MD,
California Department of Health Services, Richmond, California; Kitty Herrin, North Carolina Department of Health and Human Services, Raleigh,
North Carolina; KM Monirul Islam, MD, Wisconsin Department of Health and Family Services, Madison, Wisconsin; Thomas Largo, MPH,
Michigan Department of Community Health, Lansing, Michigan; Kim Lim PhD, Maine Department of Labor, Augusta, Maine; Barbara Materna,
PhD, California Department of Health Services, Richmond, California; Alfred May, MPH, MFS, Maine Department of Health and Human
Services, Augusta, Maine; Jackie McClain, MPH, McKing Consulting, Atlanta, Georgia; Jane McGinnis MA, MS, Nebraska Department of Health and
Human Services, Lincoln, Nebraska; Katherine McGreevy, PhD, New Jersey Department of Health and Senior Services, Trenton, New Jersey; Stephanie
Moraga-McHaley MS, University of New Mexico School of Medicine, Albuquerque, New Mexico; Karen Mulloy, DO, University of New Mexico School
of
Medicine, Albuquerque, New Mexico; John Myers, MS, National Institute for Occupational Safety and Health, CDC; Florence Reinisch,
MPH, California Department of Health Services, Richmond, California; Robert Roscoe, MS, National Institute for Occupational Safety and Health,
CDC; Kenneth Rosenman, MD, Michigan State University, East Lansing, Michigan; Lee Sanderson, PhD, National Institute for Occupational Safety
and Health, CDC; Patricia Schleiff, MS, National Institute for Occupational Safety and Health, CDC; Martha Stanbury, MSPH, Michigan Department
of Community Health, Lansing, Michigan; Thomas St. Louis, MSPH, Connecticut Department of Public Health, Hartford, Connecticut; John P.
Sestito, JD, National Institute for Occupational Safety and Health, CDC; Catherine Thomsen, MPH, Oregon Department of Human Services,
Portland, Oregon; David Valiante, MS, New Jersey Department of Health and Senior Services, Trenton, New Jersey.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].