 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Homicide Among Intimate Partners ---United States, 1981--1998Leonard J. Paulozzi, M.D., M.P.H 1 1Division of Violence Prevention AbstractProblem/Condition: A substantial percentage of all homicides in the United States are committed by intimate partners of the victims. Among females, approximately 1 in 3 homicides are intimate partner homicides (IPHs). Intimate partner homicides cannot be tracked by using death certificates because death certificates do not record the victim's relationship to the perpetrator. Reporting Period Covered: This report summarizes information regarding IPHs that occurred in the United States during 1981--1998. Description of the System: This report is based on Supplemental Homicide Reports (SHRs) collected by the Federal Bureau of Investigation (FBI) as part of their Uniform Crime Reporting System. SHRs are filed voluntarily by police departments for homicides occurring within their jurisdiction. SHRs include demographic variables regarding victims and perpetrators, their relationship, and weapon(s) used. Data from the SHR file were weighted by comparison with homicide data from death certificates to compensate for underreporting. IPHs were restricted to victims aged >10 years. Results: The risk for death from IPH among males was 0.62 times the risk among females. However, the rate among black males was 1.16 times the rate among black females. Among racial groups, rates among blacks were highest, and the rates among Asian or Pacific Islanders were lowest. Rates were highest among females aged 20--49 years and among males aged 30--59 years. During the study period, rates among white females decreased 23%, and rates among white males decreased 61.9%. Rates among black females decreased 47.6%, and rates among black males decreased 76.4%. Highest rates occurred in the southern and western states among both white and black females. A graded increase in IPH risk occurred with community population size. Approximately 50% of IPHs were committed by legal spouses and 33% by boyfriends or girlfriends for both male and female victims. IPH rates were less than expected during the months of January, October, and November. Interpretation: Although total homicide rates have fluctuated during 1981--1998, IPH rates have decreased steadily during this period, and among certain subpopulations, the decrease has been substantial. Decreases are temporally associated with the introduction of social programs and legal measures to curb intimate partner violence, but a causal relationship has not been established. Likewise, no confirmed explanation exists for the greater decrease in rates among males compared with rates among females. The differences in IPH rates by race indicate that economic, social, and cultural factors are involved. The analysis by community population size and state demonstrates that regional sociocultural differences might be involved also. Access to firearms might be a key factor in both male and female IPHs. Public Health Actions: The descriptive epidemiology of IPH is changing rapidly and should continue to be monitored. Understanding the reasons for the recent decreases in IPHs might help identify methods for primary and secondary prevention and further reduce IPH rates. INTRODUCTIONHomicide is among the six leading causes of death for persons aged 1--44 years and accounts for approximately 18,000 deaths annually in the United States (1). The majority of homicides are committed by persons known to the victim (2). Approximately one in three homicides of females is committed by current or former spouses or boyfriends, a group collectively referred to as intimate partners (3). Among male homicide victims, 5% are killed by intimate partners. Unlike other causes of death, intimate partner homicides (IPHs) cannot be described by using death certificate information, because death certificates do not record the victim's relationship to the perpetrator(s). The only nationwide information regarding IPHs comes from the Federal Bureau of Investigation's (FBI) Supplemental Homicide Reports (SHRs) database. The SHR database contains reports completed by police departments throughout the United States. Submission of crime data to the FBI is voluntary, and the system does not capture all homicides. However, the true number of homicides can be estimated by comparing FBI homicide counts with homicide counts from CDC's National Center for Health Statistics (NCHS). This report uses FBI SHR data, adjusted by comparison with NCHS data, to describe the risk for IPH by demographic variables (e.g., race, sex, age, year, month, state, and community population size) during 1981--1998. METHODSThe SHR began in the 1960's. The data collection form did not change during 1981--1998. Participating police departments complete the forms for every homicide that occurs within their jurisdictions and submit the forms monthly to the FBI as part of the Uniform Crime Reporting Program (4). All homicides that occur in the United States are included, and these homicides include U.S. residents and non-U.S. residents. Deaths of U.S. residents abroad are not included. Data are not updated to reflect the results of subsequent investigation after they are submitted (5). Throughout this report, homicide rates refer to rates of victims rather than rates of perpetrators. SHRs are used to record intentional homicides, both premeditated and nonpremeditated, and unintentional or negligent homicides (e.g., a hunter shot by another hunter). These categories are assigned as a result of police investigation, not by medical examiners or the judicial system. This study excluded negligent homicides; homicides termed justifiable, which is defined by the FBI as the killing of a person committing a felony; and homicides resulting from legal intervention. SHRs also include the relation of the victim to the offender if known when the SHRs are submitted. This study included homicides where the victim was aged >10 years and the perpetrator was an intimate partner. SHR relationship categories classified as intimate partner relationships are spouse, ex-spouse, common-law spouse, boyfriend, girlfriend, and homosexual relationships. SHRs include no separate category for ex-boyfriend or ex-girlfriend, although such persons are also regarded as intimate partners by CDC (6). Such persons would probably have been categorized as acquaintances by the FBI and therefore would not have been included in this study. This report uses the term same-sex instead of homosexual. In incidents involving >2 homicides, the SHRs were not explicit as to which homicide victim was the intimate partner of the perpetrator. Therefore, in incidents in which >2 victims were aged >10 years, the victim who was the intimate partner could not be identified with certainty. Such incidents were dropped from the analysis. In incidents in which only one of the multiple victims was aged >10 years, we assumed that the victims aged <10 years were not the intimate partners of the perpetrator. Initial comparison of the total number of homicides in SHRs with the total number of homicides not caused by legal intervention (International Classification of Diseases, Ninth Revision, E960--E969 [7]) and reported by NCHS indicated that the SHR database had included 85%--90% of homicides recorded on death certificates during 1981--1998. The completeness of SHR records varied by state and year. Therefore, SHR IPH counts in each stratum were weighted by the ratio of total homicides for victims aged >10 years in vital records to total homicides for victims aged >10 years in SHR for that same stratum. IPH rates per 100,000 population were calculated by using the weighted counts. Denominators were obtained from the U.S. Census Bureau, and denominators were restricted to the population aged >10 years to match the numerators. Rates were age-adjusted to the year 2000 U.S. population by using the direct method. For the analysis by community population size, only the total population of U.S. residents in each community type each year was obtained from the FBI (8); therefore, age-adjustment and restriction of the population to persons aged >10 years was not possible. Because data were reported by county and city police departments, the FBI divided the U.S. population into nonoverlapping strata (i.e., counties and cities) as determined by whether their police departments were part of Metropolitan Statistical Areas (MSAs) and whether they were county or city agencies. An MSA is defined as a city of >50,000 persons and the suburban counties that surround it. City police departments were further stratified by city size. For the analysis of the distribution of IPHs by month, we calculated the expected number of deaths occurring in each month under the assumption that the same number of IPHs occurred each day of the year. Risk was measured by the ratio of the observed number over the expected number each month. The weapon type used in homicides is not explicitly linked to the victims or the perpetrators in multiple-homicide and multiple-offender incidents in this data set. Therefore, the analysis of weapon type is restricted to one-victim, one-perpetrator incidents. Such incidents represented 97% of all IPH incidents among victims aged >10 years. Rates based on <11 deaths had large relative standard errors (RSEs) of >30% and are not presented (1). Rates based on <18 deaths had RSEs of 23%--29%. These rates are presented, but are considered to be unstable. No testing for statistical significance was performed, and these results are considered descriptive. RESULTSDuring 1981--1998, a total of 346,258 homicides were recorded in the SHR database, and a total of 381,408 homicides (excluding those involving legal intervention) were recorded in the vital records database. Among the SHR homicides, 16,809 were dropped from the analysis because they were classified as negligent manslaughter or justifiable homicide or were associated with legal intervention (i.e., homicide associated with police intervention). An additional 28,927 homicides were dropped from the analysis because they involved multiple victims aged >10 years or because the age, race, or sex of the victim was missing. Consequently, 300,522 SHR homicides were available for analysis. The average weight applied to the IPH counts to generate the estimated number of IPHs was the ratio of vital records homicides (381,408) to 300,522 or 1.28. Of 300,522 records, SHRs recorded 35,601 (11.8%) IPHs (i.e., one victim aged >10 years) with complete information on age, race, and sex. After weighting, an estimated 45,513 (11.9%) IPHs occurred during 1981--1998. Of these 45,513, approximately 28,991 (63.7%) of homicides were perpetrated against females, 93.8% of males were victimized by females, and 99.5% of females were victimized by males. Estimated rates of IPH varied by sex and race (Table 1). Overall, male IPH rates were 62.2% of female rates. Rates among females exceeded rates among males for all races except blacks, where IPH rates among males were greater than IPH rates among females. The highest overall and sex-specific rates were reported among blacks, followed by American Indian/Alaska Natives (AIAN), whites, and Asian or Pacific Islanders, in that order. Ethnicity data were collected only during 1980--1987 and were not analyzed for this report. Risk for IPH was greater for persons aged 20--29 years than for those aged 10--19 years (Figure 1). IPH risk peaked for black females aged 20--29 years, white females and black males aged 30--39 years, and white males aged 40--49 years. For all groups except black females, IPH rates for those aged >80 years exceeded those for persons aged 10--19 years. Rates among blacks exceeded rates among whites for females and males in all age groups. Rates among white females exceeded rates among white males for every age group, whereas rates among black males surpassed rates among black females in the 30--39 years of age group, and remained greater through successive age groups. Overall, 113 homicides occurred among persons aged 10--14 years, 0.3% of the total (not presented). IPHs occurred at ages as young as 12 years. A total of 1,845 homicides occurred among those aged 15--19 years, which is 4.1% of the total. The 2,666 homicides among those aged >65 years accounted for 5.9% of the total. Persons aged >20--64 years accounted for approximately 90% of IPH. During 1981--1998, IPHs decreased by 47.2% in the United States. IPH rates have decreased among both whites and blacks (Figure 2). During 1981--1998, rates among white females decreased 23%, and rates among white males decreased 61.9%. Rates among black females decreased 47.6%, and rates among black males decreased 76.4%. As a result of the greater decrease in rates among black males versus black females, black females, as of 1998, had the highest rates among black and white males and females. Overall, rates among males decreased 67.8%, and rates among females decreased 30.1%. The risks for IPH among white and black females varied across states, but were highest in southern states. Rates among males are not indicated by state because of the unstable IPH rates for both races. Rates among white females were higher in southern states and Rocky Mountain states (Figure 3). Rates were lowest among white females in New England and the upper Midwest. Among black females (Figure 4), the highest rates were clustered in southern states, but rates were unstable in many western and New England states. The highest rate among white females was in South Carolina; the highest rate among black females was in Arkansas. The risk for IPH consistently decreased with decreasing city size for both males and females (Table 2). MSA cities of >250,000 persons had rates two to three times the rates of cities of <10,000 persons. However, rural non-MSA counties indicated rates comparable to those of MSA cities of 50,000--99,999 persons. Approximately 50% of all IPH victims of either sex were killed by their legal spouses (Table 3). Approximately 33% were killed by boyfriends or girlfriends. The proportion of IPHs committed by same-sex partners was much greater for males than females. Among black victims of both sexes and female AIAN victims, a greater percentage was killed by boyfriends or girlfriends than by current spouses. Among male AIAN victims, an equal percentage was killed by girlfriends as by current spouses. Among white and Asian victims of both sexes, a greater percentage was killed by current spouses than by boyfriends or girlfriends. Firearms were the major weapon type used in IPHs among both sexes (Table 4). Males were more likely to be killed by knives than females, whereas females were more likely to be killed by blunt objects or blows delivered by the hands or feet. Boyfriends and girlfriends and common-law spouses were much less likely to be killed by firearms than spouses and ex-spouses. Male victims killed by girlfriends or common-law spouses were equally likely to be killed by firearms and knives. In the analysis of the distribution of deaths by month, observed numbers exceeded expected numbers (i.e., the observed-to-expected ratio exceeded one) during the summer months among both white and black males (Figure 5). This pattern was less noticeable for females (Figure 6). For all race-sex groups, January, October, and November were below expectations, although the deficit was least noticeable among white females. The difference between the peak and nadir months was greatest among white males, for whom the risk for IPH was 30% greater in July than in October. DISCUSSIONDuring 1981--1998, substantial variation occurred in the risk for IPH by race, sex, age group, time, state, and community size. Populations identified with the highest estimated rates were the same as those identified in previous studies using the SHRs (9). Data from this analysis indicated that females have an overall greater risk for IPH victimization than males. This was consistent with studies of sex-specific rates of nonfatal intimate partner assaults from emergency department data (10,11). Surveys that focused on more serious assaults (e.g., those accompanied by injuries) also reported a greater rate of assaults on females (12,13), whereas surveys that included a substantial share of assaults without physical injuries between partners report equal victimization rates (14,15). The general interpretation of the data was that males have a size and strength advantage that reduces their risk for injury in any physical confrontation with a woman (16). Why IPH rates among black males were greater than rates among black females is unclear. Also unclear is why white males were at approximately the same risk as white females for IPH in the early 1980s. One possible explanation is that females used lethal weapons more often in altercations with male intimate partners to compensate for their size and strength disadvantage. Intimate partner altercations involving firearms and knives are substantially more likely to result in death than other types of altercations (17). During 1981--1998, blacks had the highest IPH rates for both sexes. Rates among whites and Asian or Pacific Islanders were lowest, with rates among AIAN in between those among blacks and whites. Higher rates for nonfatal intimate partner altercations have been reported among nonwhites (12,13). One study reported a greater rate of IPHs among AIAN (18). These rate differences among racial groups could partially or fully be explained by socioeconomic differences. Females with low education and income levels have a greater risk for intimate partner violence (IPV) (12,19,20--24). The risk for IPH begins at puberty and increases substantially when adolescents reach ages 20--29 years. Younger females have a greater risk for IPV as well as IPH (12,20,21,23,25). This risk could be evident because females tend to move away from the protection of home in their twenties. However, the highest risk for IPH, at least for a white female, does not occur until her thirties. IPH risk for black and white females decreases substantially thereafter. For males, the highest risk for IPH occurs approximately 10 years after the peak periods for females of the same race and decreases more slowly with age. Previous studies reported that the mean age of male perpetrators of IPH is 3--4 years greater than that of their victims (3) and that risk increases with the age difference (25). Rates of nonfatal IPV also have decreased (26). The identification of domestic violence as a national problem, subsequent legal and social measures (e.g., legal advocacy services, hotlines, shelters) to remedy domestic violence, as well as rising divorce rates, have led to greater percentages of abused females ending cohabitation with abusers (27,28). These measures might be expected to equally reduce rates among males and females in parallel. However, data indicated that greater decreases occurred in IPH rates among males during 1981--1998. In 1981, rates among males were only slightly less than rates among females, whereas in 1998, rates among males had decreased to less than half the rates among females. The reason for the more substantial decreases in rates among males compared with females is not known. Firearm-related homicide rates among males might have been reduced by simplifying the process by which females can leave their abusers. Theoretically, a female who does not live with her attacker could be less likely to kill him with his own firearm. In addition, overall rates among females might not have decreased as much as rates among males because of social and legal changes that have brought about an increase in IPH rates among females in less formal noncohabiting relationships with males. During 1976--1995, the only type of IPH to increase was that of white females by their boyfriends, where the rate increased 29% (3,29). A comparison of trends in IPH with trends in total homicides demonstrates that other nonspecific factors might be involved. The most appropriate comparison is with total homicides among adults because teenage IPHs account for <5% of all IPHs, whereas teenage homicides account for a majority of the variation in overall homicide rates during 1981--1998 (9). The comparison documents that IPH decreases occurred at the same time as decreases in total homicides. During 1981--1998, total homicide rates among persons aged >20 years decreased 30.9% among females and 43.1% among males. Therefore, the decrease in female IPH (30.1%) is essentially the same as the decrease in total adult female homicides, whereas the decrease in male IPH (67.8%) is more substantial than the corresponding decrease in total adult male homicides. Possibly, the nonspecific demographic, social, and economic changes also contributed to the decrease in IPH among both sexes (30). Comparison of rates by state for white and black females indicates a pattern similar to that of all homicides, with greater rates in the southern and western states when stratified by race (31). This regional variation might be attributable to differences in cultural and social norms. For example, southerners might be more likely to endorse violence in response to insults (32,33). The steady increase in risk for IPH with urbanization is consistent with the pattern for homicide (9) and nonfatal violence among intimate partners (12,22). However, the relation might be confounded by an association between black race and urban residence (34). An increased risk from residence in rural, non-MSA counties compared with non-MSA cities has not been reported for all homicides. The distribution of IPHs by relationship indicates differences by sex and race. However, these differences cannot be interpreted as risk differences without translating them into rates. Such analysis has been conducted previously for whites and blacks (3), but not for other races. Previous analysis indicates that IPH victimization rates are greater for wives than girlfriends and for husbands than boyfriends. However, these differences have been decreasing perhaps because laws and services addressing IPV historically have been directed toward married persons (28). The weapon type used also varies by the victim's sex and relationship to the perpetrator. The percentage of male IPH victims killed with firearms (59.1%) is less than the percentage of all male homicide victims killed with firearms during the same time period (69.1%). Knives were used to kill 35.1% of male IPH victims and 16.1% of all male homicide victims during the same period. In contrast, the percentage of female IPH victims killed with firearms (64.1%) is greater than the percent of all female homicide victims killed with firearms (47.5%). Knives account for 17.4% of all female homicides and 16.1% of female IPH. Therefore, female IPH victims are more likely to be killed with a gun than are all female homicide victims, whereas male IPH victims are more likely to be killed with a knife than are all male homicide victims. Overall, the figures demonstrate the importance of reducing access to firearms in households affected by IPV (17,35). Firearms are more likely to be used by spouses than by girlfriends in the killing of male intimate partners. This finding might be a result of the association noted previously between IPHs among unmarried partners and black race. Firearms are less likely to be present in nonwhite households in the United States (36). Finally, the lower observed-to-expected ratios for IPHs during January, October, and November have not been reported previously. However, a summer increase and autumn decrease in police dispatches for domestic violence disputes have been described in California (37). This seasonal pattern is distinct from that noted among all homicides, where increased rates are observed in the summer, but the winter is the period of lowest rates (38,39). Strengths and Limitations The strengths of SHR data include data that are population-based and national in scope, a substantial number of cases, and the use of consistent data collection techniques during the study period. Unlike vital records, SHR data also include certain information regarding the perpetrators of homicides. The deficiencies of the database are also multiple and well-documented. These include underreporting, errors in the assignment of relationships, failure to identify relationship in a substantial portion of cases, and other missing information (5,40,41). The database's limitations regarding the handling of data for multiple victims and multiple perpetrators make studying IPH for such incidents difficult. In addition, the FBI does not include a separate relationship category for ex-boyfriends and ex-girlfriends, resulting in a definition of an intimate partner that is possibly narrower than CDC prefers (6). The FBI accepts the police department assignment of race in all cases, and the accuracy of this information is unknown. The level of accuracy may inflate or deflate IPH rates, especially for Asian or Pacific Islanders and AIAN. Finally, deaths are categorized by place of occurrence rather than place of death, which means that certain nonresidents are included and certain residents are omitted. Although this limitation is probably not a substantial problem for the United States overall, it might be a more substantial problem for death rates by state and city size. Differences between places of residence and places where homicides occurred would be expected to be less of a problem for IPH than for other types of homicide because IPHs are more likely to occur at the victim's home (42). NCHS included justifiable homicides of persons committing a felony by private citizens in its definition of a homicide, whereas such deaths were not included in this study. However, this definitional difference is limited. The FBI reports that such homicides account for approximately 1.5% of all homicides reported (43). Therefore, this factor should not have an effect on the accuracy of the results. Underreporting is probably the primary weakness of the database. Underreporting occurs because SHRs are not completed for all homicides and because perpetrators are unknown for a substantial portion of SHRs when they are sent to the FBI (2). Weighting the data to match homicide rates provided by NCHS was designed to address the problem of missing SHRs. No reason exists to suspect that the percentage of recognized IPHs recorded on SHRs is different from the percentage for other types of homicides. However, certain characteristics of a police agency that could not be incorporated into the weighting process (e.g., its community population size), might be related to the risk for IPH and its likelihood of being reported. This would confound the analysis by community population size, but would not affect the relative risks by race, sex, age group, month, year, or state. The problem of police reports failing to identify perpetrators at the time of SHR completion is not corrected by weighting. However, perpetrators might be less likely to be unidentified for IPHs than for non-IPHs because of the nature of the event (44). One study reported that the number of stranger (perpetrated) homicides, so labeled on SHRs filed by a sample of urban police departments, was 60.3% of the number eventually determined to have been perpetrated by strangers (45). In contrast, SHRs classified as family homicides were 91.5% of the number that were eventually determined to be perpetrated by family members. Therefore, SHR data might fail to identify approximately 10% of all IPHs. The percentage of homicides solved by police does not appear to vary appreciably by year or victim's age, at least among adults (9). Percentage varies by state, but not enough to change the relative ranking (46). The SHR database is useful for monitoring IPH, but its utility might diminish as increasing numbers of police agencies stop submitting SHRs and begin using a new system called the National Incident-Based Reporting System (NIBRS) (5). NIBRS is expected to bridge the gaps in IPH data as well as nonfatal violence between intimate partners. For example, NIBRS will include the victim-perpetrator relationship for nonfatal violence. Also, NIBRS will be able to address multiple-victim and multiple-perpetrator incident data. CONCLUSIONThis report provides information regarding the rapidly changing descriptive epidemiology of IPH. It documents sharp reductions in IPH risk overall for certain groups and notable, persisting disparities in risk by race, sex, and place of residence. Progress in reducing IPHs will depend in part on contributions from public health professionals (47). Efforts to date have focused on primary and secondary prevention (17). Secondary prevention has focused on early identification and intervention for violent couples identified through encounters with the legal and health-care systems. The predominance of firearms among weapons used to commit IPHs might help focus attention on secondary prevention of IPH through the hazards of firearm ownership by such couples. This could be accomplished by requiring police to confiscate firearms used in incidents of partner violence and restricting firearm possession by persons subject to restraining orders. Such laws have been enacted in certain states (48,49). Emphasis should focus on evaluating such interventions and developing novel interventions that protect groups at highest risk (e.g., females aged 20--29, blacks and AIAN, residents of MSAs, and residents of the southern and western states). Etiologic research priorities should begin with a better understanding of the characteristics of perpetrators and a better understanding of the reasons for the substantial decrease in IPHs during 1981--1998. References
Table 1 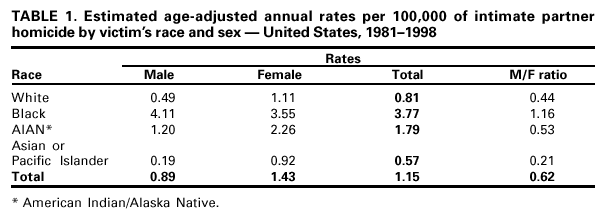 Return to top. Figure 1 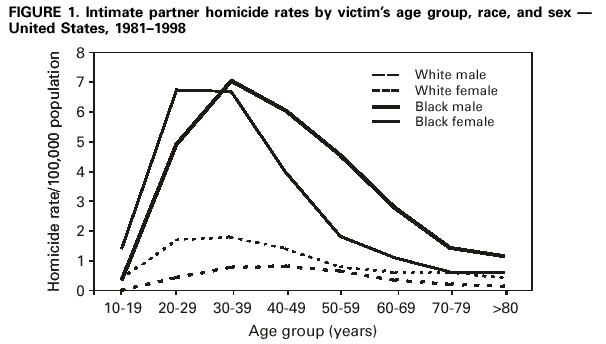 Return to top. Table 2 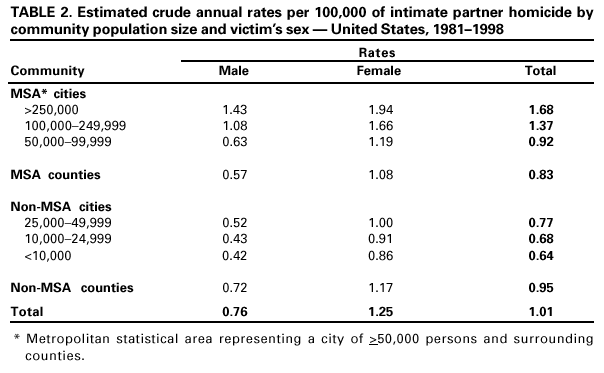 Return to top. Figure 2 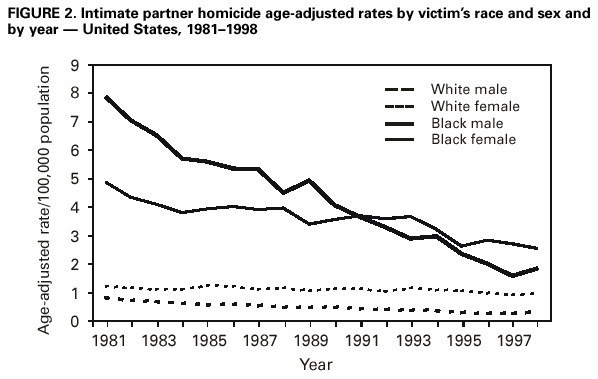 Return to top. Table 3 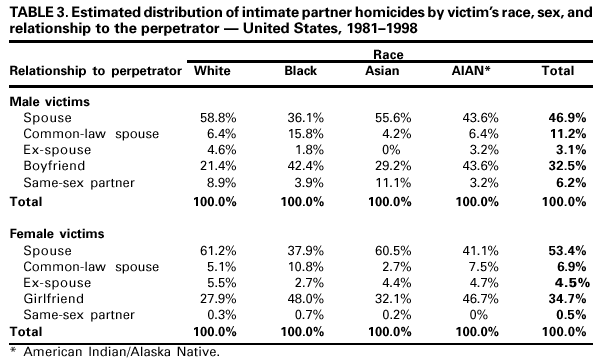 Return to top. Figure 3 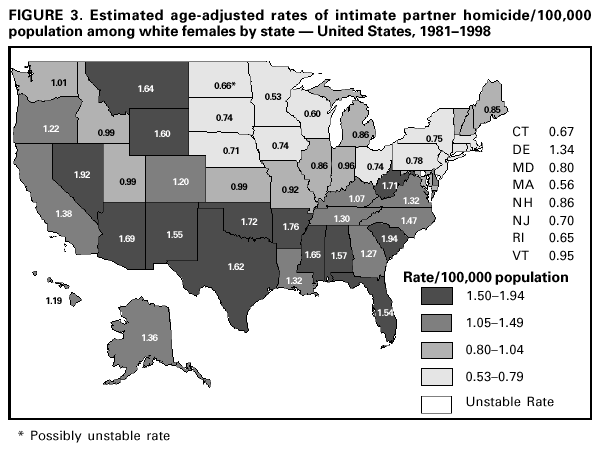 Return to top. Table 4 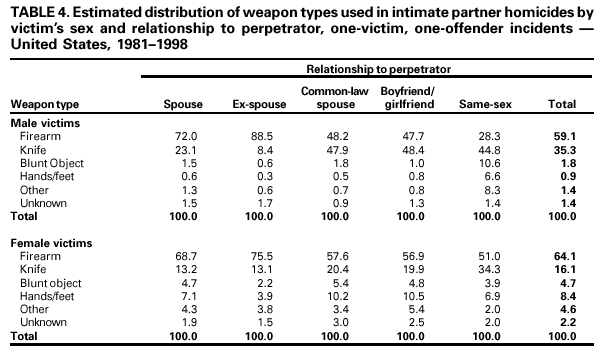 Return to top. Figure 4 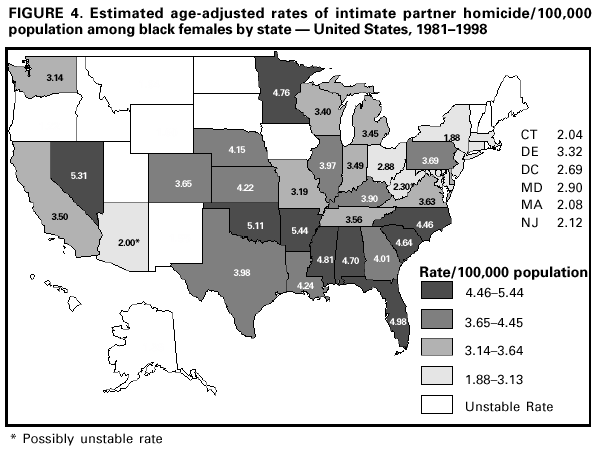 Return to top. Figure 5 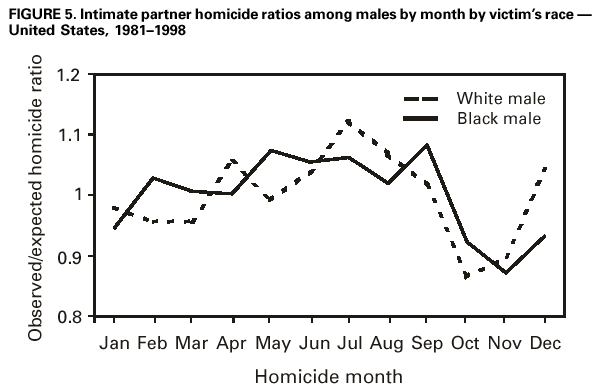 Return to top. Figure 6 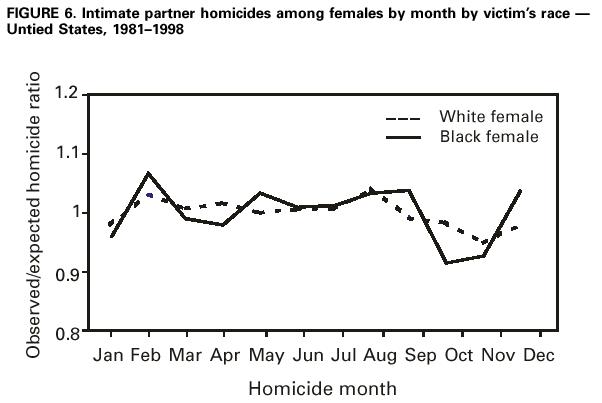 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/12/2001 |
|||||||||
This page last reviewed 10/12/2001
|