 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Primary and Secondary Syphilis --- United States, 1999In October 1999, CDC, in collaboration with other federal partners, launched the National Plan to Eliminate Syphilis in the United States. In 1998, Congress initiated funding for the syphilis elimination effort. Syphilis elimination is defined as the absence of sustained transmission (i.e., no transmission after 90 days of the report of an imported index case). The national goal for syphilis elimination is to reduce primary and secondary (P&S) syphilis to <1000 cases (rate: 0.4 per 100,000 population) and to increase the number of syphilis-free counties to 90% by 2005 (1). To describe the epidemiology of syphilis in the United States, CDC analyzed notifiable disease surveillance data for 1999. This report summarizes the results of that analysis, which indicate that, in 1999, P&S syphilis declined to a rate of 2.5 cases per 100,000 population, the lowest rate ever reported, and that syphilis transmission increasingly is concentrated in a few geographic areas. Summary data for syphilis cases reported to state health departments and the District of Columbia for 1999 were sent quarterly and annually to CDC. These data included the number of syphilis cases by patients' county of residence, sex, stage of disease, racial/ethnic group, and age group. Data on reported P&S syphilis were analyzed for this report because these cases better represented incidence (i.e., newly acquired infections within the evaluated time) than reported cases of latent infection, which are usually acquired months or years before diagnosis. P&S syphilis rates were calculated by using population denominators from the U.S. Bureau of the Census (2). The 1999 rates and numbers of cases were compared with data for 1998 (3) and 1997 (4). In 1999, 6657 cases of P&S syphilis were reported in the United States (2.5 per 100,000 population), a 5.4% decrease from the 7035 cases (rate: 2.6) reported in 1998 and a 22% decrease from the 8556 cases (rate: 3.2) reported in 1997. The South continues to have the highest rate in the country (4.5) (Figure 1)*. From 1998 to 1999, rates declined 10% in the South (from 5.0 to 4.5) and 12.5% in the Northeast (0.8 to 0.7). The rate for the West remained unchanged (1.0), and the rate for the Midwest increased from 1.9 in 1998 to 2.2 in 1999. P&S syphilis rates have declined in 28 states since 1998, and 39 states have rates below the national health objective for 2000 of 4.0. Nine of the 11 states that have rates above the 2000 objective are in the South. The rates for 1999 increased in 14 states; increases were largest in Indiana (from 3.6 to 7.6), Oklahoma (2.9 to 5.6), and Washington (0.8 to1.4). In 1999, of 3115 U.S. counties, 2473 (79.4%) reported no cases of P&S syphilis, compared with 2430 (78.0%) counties reporting no cases in 1998 and 2324 (74.6%) in 1997. In 1999, 2850 (91.5%) counties reported rates below the 2000 objective. Of the 265 counties (8.5% of all counties) with P&S syphilis rates above the 2000 objective, 243 were in the South. In 1999, 22 counties and Baltimore, Maryland; Danville, Virginia; and St. Louis, Missouri, accounted for 50% of all reported P&S syphilis cases in the United States (Table 1). The overall rate for 63 of the largest cities in the United States (population >200,000) was 5.1 cases per 100,000 persons; 24 large cities had rates higher than the 2000 objective. Cities with the highest rates of P&S syphilis were Indianapolis, Indiana (50.0); Nashville, Tennessee (46.8); and Baltimore, Maryland (38.1). The 1999 reported rate of P&S syphilis in blacks (15.2) was 30 times the rate reported in whites (0.5); the 1999 rate for blacks declined 10% compared with 1998. The rate for Hispanics increased 20% (from 1.5 in 1998 to 1.8 in 1999). The increase in rate for Hispanics was attributed to an increased number of cases in men; the number of cases in women remained stable. Rates for American Indians/Alaska Natives and for Asians/Pacific Islanders were unchanged from 1998 (2.7 and 0.4, respectively). Rates for P&S syphilis in 1999 were 45% higher for men (2.9) than for women (2.0). The male-to-female rate ratio in 1999 was 1.5:1, and has been increasing since 1994, when it was 1:1. The increase occurred in all racial/ethnic groups except Asians/Pacific Islanders and American Indians/Alaska Natives. The greatest increase occurred among Hispanics, from 2.3:1 in 1998 to 2.9:1 in 1999. An increase in the male-to-female rate ratio occurred in 16 (62%) of the 26 states that reported >25 cases in 1999. The male-to-female rate ratio was remarkably high in some cities, such as Seattle (38:1) and San Francisco (25:1). Reported by: State and local health depts. Epidemiology and Surveillance Br, Statistics and Data Management Br, Div of Sexually Transmitted Disease Prevention, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:The number and rate of P&S syphilis cases reported in 1999 were the lowest ever reported in the United States (1) with a 22% decline in both cases and rates since 1997, reflecting the substantial progress that has been made since efforts to eliminate syphilis began. The disease has become increasingly concentrated in a few geographic areas; in 1999, 50% of P&S syphilis cases occurred in <1% of counties; approximately 80% of counties reported no cases of syphilis. Although syphilis rates remain higher in the South than in other regions, the South had a 32% decline in the P&S syphilis rate from 1997 to 1999, illustrating that the greatest improvements in disease control have taken place where syphilis incidence has been greatest. Eliminating syphilis would reduce the likelihood of human immunodeficiency virus (HIV) transmission and improve reproductive health by preventing spontaneous abortions, stillbirths, and developmental disabilities caused by congenital syphilis. In addition, syphilis elimination would help to rebuild the capacity of communities to control infectious diseases and reduce racial disparities (1). Syphilis continues to disproportionately affect minority populations despite progress in reducing this racial disparity. P&S syphilis rates for blacks have remained substantially higher than those for whites. However, the magnitude of this difference has decreased 30% since 1997. The persistence of racial disparities in syphilis incidence is, in part, attributable to differences between blacks and whites regarding poverty and in access to and use of health-care services, especially in the rural South (5,6). In addition, rates increased 20% among Hispanics, due to an increase among males. Historically, rates of syphilis have been higher for men than women. The male-to-female rate ratio peaked at 3.5:1 in 1980 during the height of syphilis transmission among men who have sex with men (MSM) and decreased to 1:1 in 1994; since then, it has increased gradually. The causes of the increasing trend in the male-to-female rate ratio are not understood completely. However, one important factor is the development since 1997 of several large outbreaks of syphilis among MSM, many of whom were co-infected with HIV (7--9). In outbreaks in King County, Washington; Chicago, Illinois; and southern California, 20%--73% of MSM with syphilis also had HIV infection. Substantial increases in syphilis among MSM also have been reported in other U.S. cities. Despite national progress toward syphilis elimination, increases in rates have occurred in several states and cities. The increase in rates in these states may, in part, reflect improved reporting and case finding resulting from the national syphilis elimination effort; however, the increases also may be attributed to increases in populations that have been difficult to reach for purposes of syphilis prevention and control, such as MSM, who previously have not been a focus of the national syphilis elimination effort. The findings in this report are subject to at least three limitations. First, the quality of surveillance activities and data vary at local and state levels. Second, sexually transmitted disease reporting is incomplete. Finally, cases among patients attending public sector clinics may be more likely to be reported than cases diagnosed in the private sector, which could magnify the racial/ethnic differences in reported rates; persons of minority race/ethnicity may be more likely to attend public clinics. The variation in the demographic characteristics of syphilis patients over time and among regions highlights the need to recognize and respond to the changing epidemiology of this disease. Because increases in syphilis may emerge in areas or subpopulations that are not specifically targeted by ongoing elimination efforts, it is necessary to continually reassess and refine surveillance, prevention, and control strategies. To sustain progress toward syphilis elimination, communities must understand local patterns of syphilis transmission and develop intervention strategies, including education, risk reduction, and screening of persons at risk for this disease. Syphilis elimination must also be viewed as an entry point for building broader public health capacity to control infectious diseases and to ensure reproductive health among historically underserved communities (1). References
* Northeast=Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont; Midwest=Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin; South=Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia; West=Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. Table 1 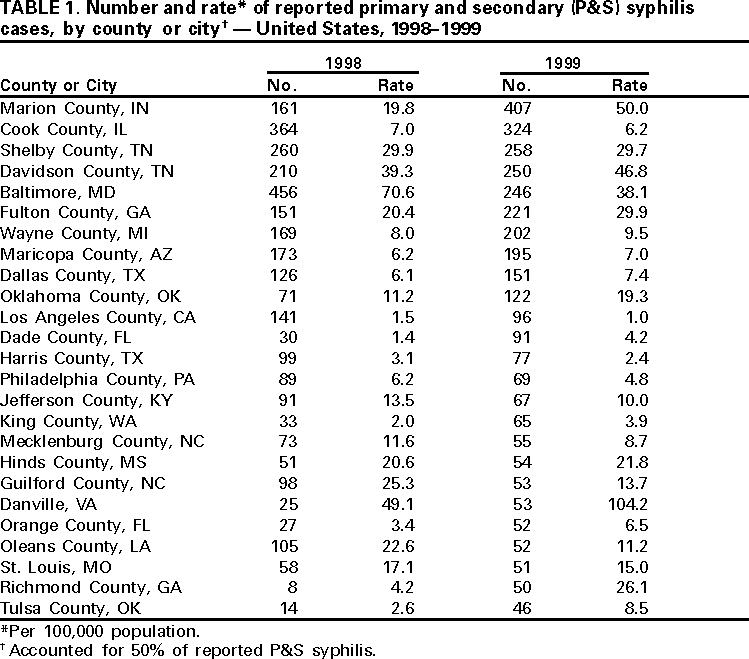 Return to top. Figure 1  Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 2/22/2001 |
|||||||||
This page last reviewed 5/2/01
|