|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
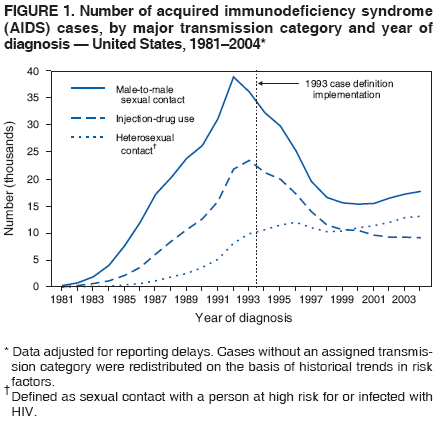
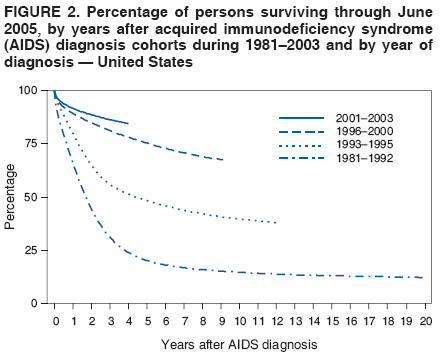
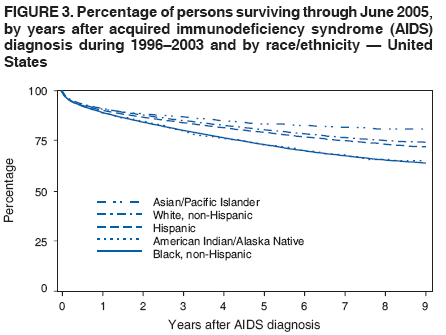
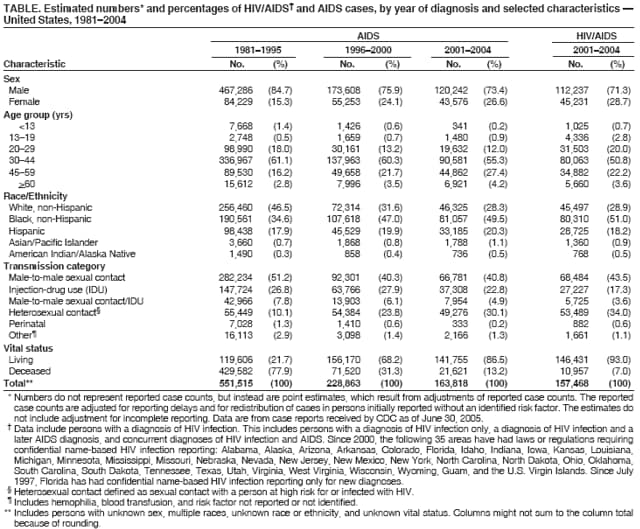
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Epidemiology of HIV/AIDS --- United States, 1981--2005In June 1981, the first cases of what was later called acquired immunodeficiency syndrome (AIDS) in the United States were reported in MMWR (1). Since 1981, the human immunodeficiency virus (HIV) epidemic has continued to expand in the United States; at the end of 2003, approximately 1,039,000--1,185,000 persons in the United States were living with HIV/AIDS, an estimated 24%--27% of whom were unaware of their infection (2). This report highlights several major epidemiologic features of the U.S. HIV epidemic, including the decrease in overall AIDS incidence, the substantial increase in survival after AIDS diagnosis (especially since highly active antiretroviral therapy [HAART] became the standard of care in 1996), and the continued disparities among racial/ethnic minority populations. These findings emphasize the need for a comprehensive national surveillance system, expanding the use of new HIV-testing technologies, promoting knowledge of HIV serostatus, and improving access to care and prevention interventions. The analysis described in this report included 1) HIV/AIDS case reports (i.e., HIV infection with or without AIDS) from the 35 areas (33 states, Guam, and the U.S. Virgin Islands) with integrated, confidential, name-based HIV/AIDS surveillance of sufficient duration to produce reliable data (i.e., 2001--2004) and 2) AIDS case reports from the District of Columbia, the 50 states, and U.S. territories received by CDC through June 30, 2005. Cases of AIDS and HIV/AIDS were analyzed by year of earliest reported diagnosis of AIDS or HIV infection, respectively. Estimated case counts reflect adjustments made to annual numbers to account for case reporting delays and deaths. Cases without an assigned HIV-transmission category were redistributed based on historical trends in risk factors (3). For the analysis of trends and the impact of HAART on these trends, AIDS cases were divided into three cohorts on the basis of year of diagnosis: 1981--1995 (pre-HAART), 1996--2000 (early HAART), and 2001--2004 (HAART era). Survival analysis was conducted using the Kaplan-Meier method. At the end of 2004, an estimated 1,147,697 HIV or AIDS cases had been diagnosed and reported to CDC (3). AIDS cases increased rapidly in the 1980s and peaked in 1992 (an estimated 78,000 cases diagnosed) before stabilizing in 1998; since then, approximately 40,000 AIDS cases have been diagnosed annually (3). Over the course of the epidemic, before this stabilization and during early prevention and treatment advances, the number of AIDS cases decreased 47% from 1992 to 1998, and decreases occurred in all demographic and transmission categories (4) (Table, Figure 1). The majority of AIDS cases continue to occur among males; however, the proportion of all AIDS cases increased from 15% (1981--1995) to 27% (2001--2004) for females (Table). Among age groups, the proportion of all AIDS cases decreased from 1.4% (1981--1995) to 0.2% (2001--2004) for persons aged <13 years (Table). Racial and ethnic minority populations have been disproportionately affected by the HIV epidemic. During 1981--1995, non-Hispanic whites were the predominant racial/ethnic group among persons who had AIDS diagnosed (47%); however, over time the proportion of cases among racial and ethnic minorities increased (2001--2004 cohort: non-Hispanic blacks accounted for 50%, and Hispanics accounted for 20%) (Table). Over time, all HIV-transmission categories demonstrated decreases in AIDS case numbers; however, the proportion of all AIDS cases for high-risk heterosexual contact (i.e., sexual contact with a person at high risk for or infected with HIV) during 1981--1995 was 10% and increased to 30% during 2001--2004 (Table). During 2001--2004, an estimated 157,468 persons had HIV/AIDS diagnosed in the 35 areas reporting to CDC (Table), with the annual case number decreasing from 41,270 in 2001 to 38,730 in 2004. Fifty-one percent of HIV/AIDS cases diagnosed during 2001--2004 were among blacks. In 2004, estimated HIV/AIDS case rates for blacks (76.3 per 100,000 population) and Hispanics (29.5 per 100,000) were 8.5 and 3.3 times higher, respectively, than rates for whites (9.0 per 100,000) (3). Among males and females, case rates among blacks (males: 131.6 per 100,000; females: 67.0 per 100,000) were seven and 21 times higher, respectively, than rates for whites (males: 18.7 per 100,000; females: 3.2 per 100,000) (3). Among HIV/AIDS cases reported during 2001--2004, the most common route of HIV infection was attributed to male-to-male sexual contact (men who have sex with men [MSM]) (44%), followed by heterosexual contact (34%), injection-drug use (IDU) (17%), MSM/IDU (4%), and perinatal (0.6%) (Table). Although the HIV/AIDS case trend (2001--2004) for MSM was stable, the estimated annual percentage change for all other transmission categories indicated a substantial decrease, with the greatest decrease occurring for IDU (9.1%) (5). During 1981--2004, a total of 522,723 deaths among persons with AIDS have been reported to CDC (Table). Substantial increases in survival after diagnosis of AIDS have been observed, particularly since 1996 (Figure 2). The proportion of persons living at 2 years after AIDS diagnosis was 44% for those with AIDS diagnosed from 1981--1992, 64% for 1993--1995, and 85% for 1996--2000. Survival for more than 1 year after diagnosis for persons with AIDS diagnosed during 1996--2003 was greater among Asians/Pacific Islanders, whites, and Hispanics, than among blacks and American Indians/Alaska Natives (Figure 3). Reported by: E Schneider, MD, MK Glynn, DVM, T Kajese, MSPH, MT McKenna, MD, Div of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), CDC. Editorial Note:HIV epidemiology continues to evolve. Although considerable progress has been made in reducing the impact of the HIV epidemic, certain populations, especially racial and ethnic minorities, continue to bear a disproportionate burden (6). Survival differences among racial and ethnic minorities might be attributed in part to late HIV diagnosis and differential access to care (7). Comprehensive and culturally sensitive approaches to prevention, treatment, and care are needed to reduce disparities in infection rates and disease progression. An estimated 252,000--312,000 persons in the United States are unaware that they are infected with HIV and, therefore, are unaware of their risk for HIV transmission (2). CDC and its partners are working together using a comprehensive approach to better understand risk behaviors and barriers that prevent persons from getting tested for HIV and accessing medical and preventive services (8). Analysis of data collected by the National HIV Behavioral Surveillance System, which surveys populations at high risk for HIV to assess prevalence and trends in risk behavior, HIV testing, and use of prevention services, revealed that of MSM surveyed in five U.S. cities, 25% were infected with HIV and of those, 48% were unaware of their infection (9). These results underscore the need to increase HIV testing and prevention efforts among populations at high risk. With the advent of HAART, the overall progression of HIV infection to AIDS and from AIDS to death has slowed (10). Consequently, AIDS surveillance no longer serves as a reliable surrogate for monitoring HIV-infection trends. Conducting timely, accurate, complete, and confidential name-based HIV surveillance, which includes both the initial and subsequent collection of relevant clinical and laboratory information (e.g., CD4 count, viral load), is critical for monitoring the changing spectrum of HIV disease (11). The use of potent combination antiretroviral therapy has also been linked to the development of adverse consequences (e.g., metabolic complications and viral resistance), which can pose challenges to clinical management (12). CDC and its partners conduct supplemental studies to monitor clinical outcomes of HIV/AIDS cases, including integrating laboratory technologies with HIV/AIDS surveillance to monitor variant, atypical, and drug-resistant strains of HIV (13). The national surveillance system for HIV/AIDS has evolved with advances in the understanding of this epidemic (4,11). The system now includes surveillance data from persons diagnosed with HIV to describe the epidemiology more accurately. CDC and the Council of State and Territorial Epidemiologists recommend that all states and territories conduct confidential, name-based HIV surveillance. As of May 2006, a total of 43 states and five territories had implemented confidential, name-based HIV-infection reporting. This integrated surveillance provides the only population-based monitoring of the HIV epidemic in the United States and provides invaluable epidemiologic data to local, state, and federal agencies to improve resource allocation, program planning, and evaluation for HIV-prevention and treatment services. Diagnosis of asymptomatic HIV infection in a person does not necessarily signify recent infection. On average, 8--11 years elapse before a person has onset of symptoms of HIV infection (14). To provide a population-based estimate of HIV incidence (i.e., new HIV infections), CDC, in conjunction with 34 state and local health departments, is conducting HIV-incidence surveillance by using STARHS (Serologic Testing Algorithm for Recent HIV Seroconversion) (15). Knowledge of newly acquired (e.g., <6 months) HIV infections will enable more accurate monitoring of trends among persons recently infected. This will allow more effective targeting of treatment and prevention measures, thereby increasing opportunities to interrupt HIV transmission. CDC expects to report data from this system in late 2006. Despite impressive accomplishments, many new challenges have arisen since the beginning of the HIV epidemic. A comprehensive national surveillance system must be complete and timely to better identify and monitor trends in HIV risk, HIV infection, and HIV infection outcomes. Twenty-five years into the HIV epidemic, surveillance data continue to highlight the need for a multifaceted approach that promotes knowledge of serostatus (e.g., via routine HIV testing), linkage to care, and risk-reduction strategies for seronegative persons at high risk for HIV infection and persons living with HIV. Acknowledgments This report is based on data contributed by state, territorial, and local health departments. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/1/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|