|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
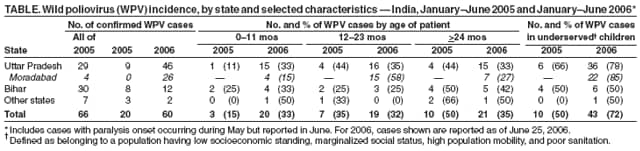
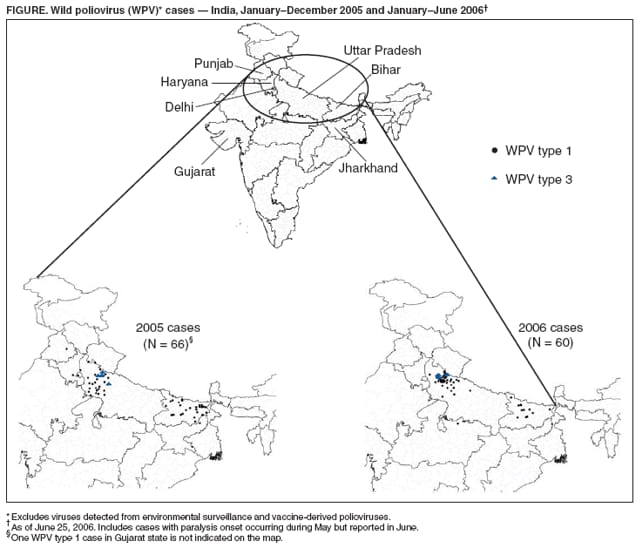
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- India, January 2005--June 2006The global eradication of poliomyelitis has reached a critical stage. The disease remains endemic in only four countries (Afghanistan, India, Nigeria, and Pakistan), which have reported most of the cases in 2006 (1). India is the most populous of the polio-endemic countries. Beginning in 2005, the Government of India (GOI) and its partners intensified eradication efforts by implementing additional immunization and surveillance strategies, including introduction of monovalent oral poliovirus vaccine types 1 and 3 (mOPV1 and mOPV3, respectively)* (2). The number of reported cases decreased from 134 in 2004 to 66 in 2005. However, cases have resurged in 2006; as of June 25, 2006, a total of 60 cases had been reported. Although intense local transmission continues in certain areas (i.e., western Uttar Pradesh [UP]), interruption of wild poliovirus (WPV) transmission in India is feasible with continued effective interventions. This report summarizes progress toward polio eradication in India from January 2005 through June 2006. Acute Flaccid Paralysis (AFP) SurveillanceAFP surveillance is essential to polio eradication. AFP surveillance in India continues at high levels of sensitivity, with surveillance indicators above current World Health Organization (WHO) operational targets.† In UP and Bihar, the only two Indian states where polio remains endemic, the annual nonpolio AFP rate was >10 cases per 100,000 population aged <15 years, and adequate stool specimen collection was above 80% from January 2005 through June 2006. Virologic testing of stool specimens from AFP patients in India is conducted at eight national laboratories, all of which are accredited by WHO as part of the Global Polio Laboratory Network (3). Despite an increased workload (55,535 specimens tested in 2005 compared with 35,885 in 2004), the laboratories sustained high levels of performance. Results of primary virus isolation were communicated to India's National Polio Surveillance Project within 28 days of specimen receipt at the laboratory for 99% of specimens tested in 2005. The mean interval from receipt of primary culture results to final poliovirus categorization (i.e., wild or vaccine related) was 6 days. WPV EpidemiologyIndia reported 66 polio cases from 35 districts with onset of paralysis in 2005, of which 62 (94%) were WPV type 1 (WPV1) and four (6%) were WPV type 3 (WPV3). All four WPV3 cases occurred in UP. As of June 25, India had reported 60 polio cases (57 WPV1 and three WPV3) in 2006 with onset of paralysis occurring through May 2006. These 60 cases came from 20 districts, compared with 20 cases from 18 districts for the same period in 2005 (Figure). Of the cases reported in 2006, a total of 46 were from UP state, 12 from Bihar state, one from Madhya Pradesh state bordering UP, and one from Jharkhand state bordering Bihar. Twenty-six (43%) cases, including all three WPV3 cases, were reported from Moradabad district in UP. Forty-three (72%) of all cases reported in 2006 occurred in underserved§ children, compared with 31 (47%) of all such cases reported in 2005. In Moradabad district, >85% of cases in 2006 were in the underserved population. In India, the majority of 2006 cases have occurred in children aged <2 years; 33% of 2006 cases have been reported in children aged <12 months, compared with only 15% in 2005. In Moradabad, >50% of 2006 cases have been reported in children aged 12--23 months (Table). Genetic sequencing of WPVs isolated in India reveal that the number of distinct genetic clusters¶ of WPV1 decreased from three in 2004 to two in 2005 to one in 2006 (as of June 25, 2006) (3). Within the surviving WPV1 cluster, distinct lineages (roughly corresponding to chains of transmission) have been reduced in UP and Bihar to two each in 2006 from five and four each, respectively, in 2005. Only one WPV3 lineage persists in India and is located in only one district (Moradabad) in UP. Weekly environmental sewage sampling in three urban wards of Mumbai detected WPV1 in 85 (53%) of 159 samples in 2004, in 16 (10%) of 156 samples in 2005, and in two (5%) of 42 samples in the first half of 2006, most recently in January 2006.** Genetic sequencing indicated that the isolates were closely related to viruses found in Bihar and UP. Although three WPV1 cases were reported from Mumbai and nearby districts in 2004, no WPV cases were reported there from January 2005 through June 2006, despite highly sensitive surveillance. Immunization ActivitiesRoutine vaccination coverage with 3 doses of OPV continues to be low in the polio-endemic states (Bihar, 27%; western UP, 38%; and eastern UP, 45%) (UNICEF, unpublished data, 2005). To improve these coverage rates, new strategies are being planned and gradually implemented, including hiring and training more staff dedicated to routine immunization, expanding vaccine-preventable disease surveillance, and launching immunization campaign activities specifically for all routine immunizations covered under WHO's Expanded Program on Immunization. GOI conducted 10 supplementary immunization activity (SIA)†† rounds during 2005, including two nationwide rounds and eight subnational rounds in states and districts where WPV was detected or where a high risk for WPV circulation existed. During the first 6 months of 2006, GOI conducted four SIAs, two nationwide and two subnational rounds; GOI is planning four more SIAs for the remainder of 2006. Continued monitoring of SIAs revealed that the percentage of missed houses increased from approximately 8% during January--April 2005 to an average of 11% in all rounds during May 2005--January 2006 in the densely populated Moradabad district in UP, indicating a decline in SIA quality.§§ SIAs added mOPV1 in April 2005, and it was used in most SIA rounds conducted during April--November in Bihar, UP, Mumbai (Maharashtra state), and polio-free states that had documented cases of WPV1 importation. However, mOPV1 was not used in consecutive rounds until 2006, when, for the first time, four consecutive mOPV1 rounds were conducted in western UP. In December 2005, mOPV3 was first used in eradication activities in western UP, after detection of WPV3 in Moradabad district. Trivalent OPV (tOPV) continues to be used in the routine childhood immunization program and in SIAs in states at low risk for polio transmission (1). Reported by: Ministry of Health and Family Welfare, Government of India; National Polio Surveillance Project; Immunization and Vaccine Development Dept, WHO Regional Office for South-East Asia, New Delhi; Poliovirus Laboratory Network, Ahmedabad, Bangalore, Chennai, Coonoor, Kasauli, Kolkata, Lucknow, and Mumbai; UNICEF, New Delhi, India. Immunization, Vaccines and Biologicals Dept, WHO, Geneva, Switzerland. Div of Viral Diseases and Global Immunization Div, National Center for Immunization and Respiratory Diseases; SJ Doshi, MD, EIS Officer, CDC. Editorial Note:The polio eradication program in India reached several milestones in 2005 and early 2006 toward the goal of ending polio transmission in India. The use of mOPV1 during large-scale SIAs had a substantial impact on virus transmission in polio-endemic areas where high coverage was maintained and achieved; mOPV1 was instrumental in stopping local virus transmission in Mumbai, where sewage samples indicated only imported viruses. The number of virus lineages persisting in western UP decreased from five in 2005 to two in 2006 after use of mOPV1. In Bihar, the use of mOPV1, combined with increased government support, led to a reduction in lineages from four in 2005 to two in 2006. Although three times as many cases were reported from India during the first half of 2006 compared with the same period in 2005, genetic-sequencing data indicate that transmission is now restricted to only one circulating WPV1 genetic cluster, and over half of the chains of virus transmission present in 2004 have been eliminated. The geographic distribution of WPV1 circulation has contracted since 2005, with no WPV cases identified in the southern Indian states, West Bengal, or in the western states of Maharashtra or Rajasthan. Delhi, which is adjacent to UP, has not reported a WPV case in 2006. Even in UP, the resurgence of cases is restricted to a circumscribed area of a few districts of western UP, centered on Moradabad district. Moreover, WPV3 has been identified in only two administrative blocks in one district in western UP in 2006, compared with four administrative blocks in three districts in 2005. The polio laboratory network remains a cornerstone of India's polio eradication program. By strengthening management techniques in 2005 and introducing new technologies in early 2006, the laboratories continued to provide rapid results. Genetic data generated by the Global Specialized Laboratory in Mumbai have been used to target immunization efforts in the most critical areas. For example, during SIAs, vaccinators are now deployed along major train routes, after genetic data and epidemiologic investigations identified these routes as channels of virus transmission across districts and states. UP and Bihar remain the source of ongoing WPV transmission in India and exportation of WPV to other countries, including the polio-free countries of Angola (with spread to the Democratic Republic of Congo and Namibia), Bangladesh, and Nepal (4,5). Data from UP and Bihar confirm that most WPV circulation is occurring in areas with inadequate SIA quality, suggesting that the early 2006 resurgence of cases has resulted from reduced community participation in vaccination campaigns and decline in the quality of vaccine program implementation. Western UP is a particularly challenging area for interrupting polio because of high population density, a large birth cohort, poor sanitation, and high population mobility. These characteristics are especially evident in areas such as Moradabad, where a large population resides with low socioeconomic standing, marginalized social status, and poor sanitation. To improve SIA quality in areas at high risk for polio transmission, several strategies were used during 2005 and early 2006 on the basis of recommendations from the India Expert Advisory Group on Polio Eradication (IEAG), including 1) development and licensure of mOPV1 and mOPV3 for use in SIAs, 2) deployment of additional personnel to areas at high risk for polio transmission, 3) enhanced social mobilization efforts targeted to underserved population groups missed during previous SIAs, 4) use of mobile teams to vaccinate children at transit points (e.g., train stations or markets), and 5) increased engagement and accountability of GOI leaders and workers (2). In May 2006, IEAG recommended increased emphasis on administering a dose of mOPV1 to all infants at birth to 1) vaccinate infants before they are infected with competing enteric pathogens that might reduce the efficacy of OPV and 2) help decrease the population immunity gap in areas of UP at high risk for polio transmission. Improved surveillance and maintenance of recent gains in SIA coverage in Bihar also were recommended (6). As a result of these new programmatic strategies, field monitors reported improvement of SIA quality in Bihar in all four rounds in 2006, compared with the rounds held in the second half of 2005. Reports from Moradabad also indicate that the number of missed houses during vaccination activities steadily decreased, from 11% in January 2006 to 8% by April 2006. Additional monitoring measures to identify and target underserved children and those in transit will help ensure that all children are reached. The decrease in genetic diversity and geographic spread of the virus suggests that India might be in the final stages of polio eradication. A resurgence of cases occurred in a localized area of western UP because of problems with immunization campaign quality. Improvements in SIA implementation in the remaining areas of virus transmission, effective social mobilization and communication activities targeting the underserved population, and enhanced community and political commitments are needed to eradicate the disease in India. References
* mOPV contains polio vaccine virus against either WPV type 1 or type 3 only; it does not provide protection against other WPV types. mOPV does provide greater immunity to the specific WPV type than does the same number of doses of trivalent OPV. † The current WHO operational target for countries at high risk for polio transmission is a nonpolio AFP rate of at least two cases per 100,000 population aged <15 years and adequate stool specimen collection from >80% of AFP cases where two specimens are collected >24 hours apart, both within 14 days of paralysis onset, and shipped on ice or frozen ice packs to a WHO-accredited laboratory. § Defined as belonging to a population having low socioeconomic standing, marginalized status, high population mobility, and poor sanitation. ¶ All WPVs isolated in India are sequenced across the interval encoding the major capsid protein (VP1) (approximately 900 nucleotides), and results are analyzed to determine the likely origin (by state and district) of the virus. Isolates within a cluster share >95% VP1 nucleotide sequence identity. ** Although sewage samples continue to be collected, no laboratory results have been available since the end of March 2006 because of a fire in April in the Global Specialized Laboratory in Mumbai. †† Mass campaigns conducted during a brief period (days to weeks) in which 1 dose of OPV is administered to all children aged <5 years, regardless of vaccination history. The geographic extent of campaigns (national versus subnational) is determined by analysis of surveillance data. OPV can be administered at fixed sites, by mobile teams during house-to-house visits, by mobile teams at transit points (e.g., train stations or markets), or through a combination of strategies, depending on local circumstances. §§ SIA quality is defined by the number of missed houses during house-to-house vaccination activities and the number of houses designated incorrectly by vaccinators.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 7/19/2006 |
|||||||||
|