
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Primary and Secondary Syphilis --- Jefferson County, Alabama, 2002--2007
In June 2006, the Alabama Department of Public Health (ADPH) requested assistance from CDC to investigate and control a multiyear epidemic of syphilis in Jefferson County. The county had experienced a decrease in primary and secondary (P&S) syphilis cases, from 279 in 1995 to nine in 2002. By 2005, the incidence had begun to rise substantially, culminating with 238 cases in 2006 and 166 in 2007. Beginning in August 2006, CDC assisted the Jefferson County Department of Health (JCDH) in investigating the increase in cases and in planning control measures. This report summarizes the results of that investigation, which found that the characteristics of cases during 2002--2004 differed substantially from cases during 2005--2007. Declines in U.S. syphilis rates, which reached their lowest point in 2000, led to optimism that syphilis elimination (defined as the absence of sustained syphilis transmission) in the United States was possible, and CDC's National Syphilis Elimination Plan was launched in 1999 (1). Although increased U.S. syphilis rates in the early 2000s have been reported to be associated primarily with transmission among men who have sex with men (MSM) (2), the findings from this investigation indicate reemergence of syphilis among women and heterosexual men in Jefferson County. Public health officials in other areas should remain alert for similar epidemiologic shifts. Public health departments should facilitate access to effective treatment in sexually transmitted disease (STD) clinics or other settings, consider selective screening in high-prevalence populations (e.g., in correctional settings), and ensure adequate partner notification and treatment.
Outbreak Investigation
Jefferson County includes the city of Birmingham, and in 2007 was the county of residence for 658,779 persons (3), 14.2% of the state population. Most of the population is white (56.3%), black (41.2%), or Asian (1.3%), and 2.9% are of Hispanic ethnicity.* The county is served by one public STD clinic. During 2002--2007, 60.2% of all P&S syphilis cases in the county were reported from this clinic. By Alabama state law, clinicians and laboratories must report syphilis cases and positive syphilis laboratory tests within 7 days of diagnosis or identification.
This report focuses on P&S syphilis because these cases represent the earliest stages of infection and approximate syphilis incidence. For STD investigations, the interview period is defined as the interval during which sexual contact might have resulted in syphilis transmission; for primary syphilis this interval includes the 3 months before symptom onset as well as the time with symptoms, and for secondary syphilis this includes the 6 months before symptom onset as well as time with symptoms (4).
For this analysis, MSM were defined as men who reported sex with men only or sex with men and women; men who had sex with women (MSW) were defined as men who reported sex with women only. Based on the assumption that nearly all syphilis among women is acquired through heterosexual transmission, heterosexuals were defined as all women and MSW.
Sources of data for this investigation included local case reports, interview data, and data from the National Electronic Telecommunications System for Surveillance (NETSS). Syphilis patients were interviewed by JCDH staff members using the standard CDC interview form,† which includes questions on demographic variables, methods of detection, information source, treatment date, sex and number of partners, intravenous drug use, symptoms, laboratory results, and contact tracing information. Beginning in 2003, these interviewers also used a supplemental expanded interview form developed by ADPH that requested additional behavioral information, including information on noninjection drug use during the past 12 months and whether the patients reported any anonymous sex partners during the past 3 months. Investigators reviewed 1) all reports of P&S syphilis among Jefferson County residents whose first positive laboratory specimens were collected during January 2002--April 2006 and 2) data from expanded supplemental interviews conducted during January 2003--April 2006. Although original case reports and supplemental interview data were available to CDC investigators only for cases reported through April 2006, for this report, NETSS provided local case report data through 2007 for Jefferson County, including data on sex, race, ethnicity, age group, information source, and syphilis stage; sex of partner data on these cases through 2007 were provided by JCDH. Proportions were compared statistically using chi-square tests with a two-sided significance level of p<0.05. Medians were compared using Kruskal-Wallis tests with a significance level of p<0.05.
During 2002--2007, 580 P&S syphilis cases were reported, including 197 cases (34.0%) of primary syphilis and 383 cases (66.0%) of secondary syphilis. Of the 568 cases for which data on race/ethnicity were available, 494 cases (87.0%) were in blacks, 69 (12.1%) were in whites, four (0.7%) were in Asians, and one was in a Hispanic (0.2). Of the 529 cases for which sex of partners data were available, 88 cases (16.6%) were in MSM, 223 cases (42.2%) were in MSW, and 218 cases (41.2%) were in women. Reported P&S rates (per 100,000 population) increased from 1.4 in 2002 to a peak of 36.2 in 2006, and then decreased to 25.2 in 2007 (Figure 1). The proportion of cases in persons aged <30 years increased from 22.4% during 2002--2004 to 37.4% during 2005--2007 (p=0.016). No significant changes by race and ethnicity were observed from the period 2002--2004 to 2005--2007. The proportion of cases occurring among heterosexuals increased from 53.8% during 2002--2004 to 87.7% during 2005--2007 (p<0.001). The proportion of cases with primary syphilis increased from 25.4% during 2002--2004 to 35.1% during 2005--2007 (p=0.114). During 2002--April 2006, MSW were more likely than women (57.0% versus 19.2%, p<0.001) or MSM (22.0%, p<0.001) to have primary syphilis (Table).
During 2002--2007, most cases were detected in the county STD clinic (60.2%), other public clinics (9.1%), health maintenance organization (HMO) or private physician offices (9.5%), hospitals or emergency departments (8.2%), and correctional facilities (6.5%). Cases were more likely to be reported from other public clinics during 2002--2004 (19.4%) than during 2005--2007 (7.8%, p=0.002); differences for other provider types were not significant. During 2002--April 2006, median time from laboratory specimen to treatment was 0 days in the STD clinic, 4.5 days in HMOs and private physician offices, 6.5 days in correctional facilities, 11.5 days in hospitals, and 20 days in emergency departments (p<0.001).
Risk Factor Analysis
Of 580 cases reported during 2002--2007, 240 (41.4%) were reported during January 2002--April 2006 and had case reports available at the time CDC investigative assistance began in August 2006. A total of 169 of these had supplemental interview data available, permitting risk factor analyses. Heterosexuals were more likely than MSM to report exchange of money or drugs for sex (27.1% vs. 6.8%, p=0.001). (Table) Heterosexuals were more likely to use crack cocaine (30.9% versus 11.5%, p=0.046), whereas MSM were more likely to use methamphetamines (11.5% versus 0.0%, p<0.001). Two patients (both women) reported intravenous drug use, and 60% of cases identified in corrections were in patients who reported exchange of money or drugs for sex. The median number of sex partners during the interview period was 2.0 and did not vary by sex or sex of partners.
Public Health Response
In response to the epidemic, JCDH 1) extended its STD clinic hours beyond regular business hours, staying open until 6:00 p.m. four evenings a week; 2) increased from five to seven the number of staff dedicated to interviewing and providing partner services for syphilis patients; 3) collaborated with a community-based organization, AIDS in Minorities, to provide education and referral for screening in postal code areas with high-morbidity; and 4) launched a media campaign using advertisements on buses, billboards, radio, and television.
Reported by: EW Hook, MD, Univ of Alabama-Birmingham and Jefferson County Dept of Health; M Fleenor, MD, Jefferson County Dept of Health; S Langston, MPH, Alabama Dept of Public Health. J Beltrami, MD, SM Berman, MD, H Weinstock, MD, Div of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention; D Dowell, MD, TH Dinh, MD, EIS Officers, CDC.
Editorial Note:
National data on the sex of the partners of syphilis patients have only become available since 2005, when CDC requested this information with national case reports (5). Therefore, before 2007, trends in heterosexual and same-sex transmission of syphilis can only be estimated using male-to-female rate ratios. Male-to-female ratios close to 1 are assumed to indicate predominantly heterosexual transmission, whereas higher male-to-female ratios are thought to indicate transmission among MSM (2). After 2000, when syphilis rates in the United States reached their lowest point since reporting began (6), male-to-female rate ratios increased, suggesting increasing transmission among MSM. This conclusion was consistent with local epidemiologic reports (2). Although P&S syphilis rates increased disproportionately among men, they also increased among women every year during 2004--2007 (5), suggesting that although rate increases were proportionally greater among MSM, increasing heterosexual transmission also occurred. Most of the increase in P&S syphilis among women in the United States during 2004--2007 was in the South, where syphilis rates remained higher than in other regions§ (5). During 2003--2007, rates among women increased 69% in South, increased 22% in the West, and decreased in other regions (Figure 2).
This investigation in Jefferson County, Alabama, found that increases in syphilis incidence during 2002--2007 occurred mainly among heterosexuals. Compared with MSM, heterosexuals with syphilis were more likely to report drug use, particularly cocaine, and exchange of sex for money or drugs. These findings are reminiscent of syphilis epidemiology in the late 1980s and early 1990s, when transmission occurred predominantly among heterosexuals and was associated with crack cocaine and exchange of drugs for sex (7). In the past, these epidemiologic associations were used to support the screening of populations in detention (1), because arrestees often were detained for commercial sex work and for drug-related charges. For example, in two cities with heterosexual syphilis outbreaks that were brought under control (during 1996--2002 and 1997--2002), 40% of cases in females that were likely to contribute to ongoing transmission were identified in detention (8). Screening in correctional facilities has been shown to be feasible and effective in limiting syphilis transmission, especially in communities with predominantly heterosexual transmission (1).
Timely treatment of syphilis prevents complications and limits transmission. In Jefferson County, women and MSM were less likely than heterosexual men to present with primary syphilis. This also has been observed nationally (9) and might be related to the anatomic location of primary syphilis lesions (which are often painless and of unappreciated significance); in women and MSM, these lesions might more often occur on the vagina or cervix, or anus, respectively, sites that are difficult to notice. Encouraging women and MSM at risk for syphilis to examine themselves for lesions might help decrease time to treatment, although relevant evaluations of this approach are just beginning. Increasing the use of STD clinics, which were associated with shorter time to treatment than other settings, especially emergency departments, might decrease time to treatment. All health-care providers who suspect primary syphilis in a patient should presumptively treat for it at the time of examination (4).
The findings in this report are subject to at least three limitations. First, underreporting was likely because reporting depends on patients seeking care, health-care providers diagnosing syphilis, and reporting to the health department. An estimated 20% of syphilis infections are never diagnosed or reported (10). Second, although JCDH attempted to conduct supplemental interviews for all patients with reported cases starting in 2003, supplemental interview data were not available for all reported cases. Interviewed patients might have represented those who were easier to contact, and the analysis might have underrepresented persons with certain risk factors, such as drug use. Finally, responses to interviews might be subject to recall and information bias given the sensitive nature of some questions (e.g., regarding the number of sex partners and drug use).
With the epidemic now growing in different populations and requiring different prevention approaches, adequate containment will be a challenge. Public health officials should include data on sex of partners with case reporting, as recommended by CDC (1). STD programs should employ methods that have been successful in the past, including serologic screening in high-prevalence populations such as in corrections settings, facilitating access to effective treatment, and accessing and treating partners, particularly those most likely to sustain transmission (8).
Acknowledgment
The findings in this report are based, in part, on contributions by S Yu, MPH, Jefferson County Dept of Health.
References
- CDC. The National Plan to Eliminate Syphilis from the United States, 2006. Atlanta, GA: US Department of Health and Human Services, CDC; 2006. Available at http://www.cdc.gov/stopsyphilis/seeplan2006.pdf.
- CDC. Primary and secondary syphilis---United States, 2002. MMWR 2003;52:1117--20.
- US Census Bureau. Table 1: annual estimates of the population for counties of Alabama. Available at http://www.census.gov/popest/counties/tables/CO-EST2007-01-01.xls.
- CDC. Sexually transmitted diseases treatment guidelines, 2006. MMWR 2006;55(No. RR-11).
- CDC. Sexually transmitted disease surveillance 2007. Atlanta, GA: US Department of Health and Human Services, CDC; 2008. Available at http://www.cdc.gov/std/stats07/main.htm.
- CDC. Primary and secondary syphilis---United States, 2003--2004. MMWR 2006;55:269--73.
- Rolfs RT, Goldberg M, Sharrar RG. Risk factors for syphilis: cocaine use and prostitution. Am J Public Health 1990;80:853--7.
- Kahn RH, Peterman TA, Arno J, Coursey EJ, Berman SM. Identifying likely syphilis transmitters: implications for control and evaluation. Sex Transm Dis 2006;33:630--5.
- Beltrami J, Weinstock HS. Primary and secondary syphilis among men who have sex with men in the United States, 2005. Paper presented at 17th International Society for STD Research. Seattle, WA: July 29--August 1, 2007.
- Cates W. Estimates of the incidence and prevalence of sexually transmitted diseases in the United States. American Social Health Association Panel. Sex Transm Dis 1999;26(4 Suppl):S2--7.
* U.S. Census Bureau. State and county quickfacts. Available at http://quickfacts.census.gov/qfd/states/01/01073.html.
† CDC form 73.54 8-91.
§ South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont. West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin.
FIGURE 1. Number of primary and secondary syphilis cases among men who have sex with men (MSM), among men who have sex with women only (MSW), and among women --- Jefferson County, Alabama, 2002--2007*
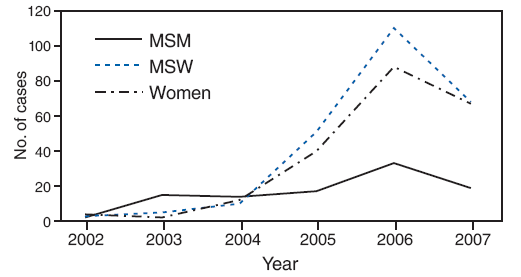
* Data from Jefferson County Department of Health (JCDH)/CDC investigation January 2002--April 2006 supplemented with 2006--2007 data provided by JCDH.
Alternative Text: The figure above shows the number of primary and secondary syphilis cases among men who have sex with men, men who have sex with women only, and women in Jefferson County, Alabama, from 2002 through 2007. The data show a sharp increase in the number of cases among men who have sex with women and only and women from 2004 to 2007, followed by a sharp decrease to 2007.
FIGURE 2. Rates* of primary and secondary syphilis among women, by region† --- United States, 2000--2007
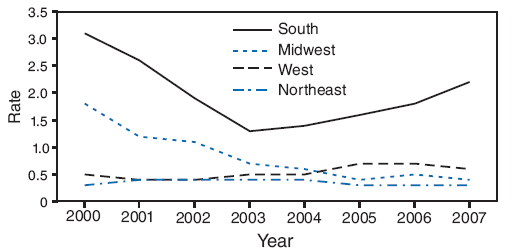
* Per 100,000.
† South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont.
Alternative Text: The figure above shows the rate of primary and secondary syphilis cases among women by U.S. region, from 2000 through 2007. For the South region, the data show a sharp decrease in the rate from 2000 to 2003, followed by a steady increase to 2007.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 5/7/2009