Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
A Comprehensive Immunization Strategy to Eliminate
Transmission of Hepatitis B Virus Infection in the United States
Recommendations of the Advisory Committee on Immunization
Practices (ACIP) Part 1: Immunization of Infants, Children, and Adolescents
Please note:
Errata have been published for this article. To view the errata,
please click here and here.
Prepared by
Eric E. Mast, MD1, Harold S. Margolis,
MD,1 Anthony E. Fiore, MD,1 Edward W. Brink,
MD,2 Susan T. Goldstein,
MD,1 Susan A. Wang, MD,1 Linda A.
Moyer,1 Beth P. Bell, MD,1 Miriam J. Alter,
PhD1
1Division of Viral Hepatitis, National Center for Infectious Diseases,
2Immunization Services Division, National Immunization Program
The material in this report originated in the National Center for Infectious Diseases, Rima F. Khabbaz, MD, Director, Division of Viral Hepatitis,
John W. Ward, MD, Director; and the National Immunization Program, Anne Schuchat, MD, Director, Immunization Services Division, Lance
E. Rodewald, MD, Director.
Corresponding preparer: Eric E. Mast, MD, Division of Viral Hepatitis, National Center for Infectious Diseases, 1600 Clifton Road, NE, MS
G-37, Atlanta, GA 30333. Telephone: 404-371-5460; Fax: 404-371-5221; E-mail: [email protected].
Summary
This report is the first of a two-part statement from the Advisory Committee on Immunization Practices (ACIP)
that updates the strategy to eliminate hepatitis B virus (HBV) transmission in the United States. The report provides
updated recommendations to improve prevention of perinatal and early childhood HBV transmission, including implementation
of universal infant vaccination beginning at birth, and to increase vaccine coverage among previously unvaccinated children
and adolescents. Strategies to enhance implementation of the recommendations include 1) establishing standing orders
for administration of hepatitis B vaccination beginning at birth; 2) instituting delivery hospital policies and procedures and
case management programs to improve identification of and administration of immunoprophylaxis to infants born to mothers
who
are hepatitis B surface antigen (HBsAg) positive and to mothers with unknown HBsAg status at the time of delivery; and
3) implementing vaccination record reviews for all children aged 11--12 years and children and adolescents aged <19 years
who were born in countries with intermediate and high levels of HBV endemicity, adopting hepatitis B vaccine requirements
for school entry, and integrating hepatitis B vaccination services into settings that serve adolescents. The second part of the
ACIP statement, which will include updated recommendations and strategies to increase hepatitis B vaccination of adults, will
be published separately.
Strategy to Eliminate Hepatitis B Virus Transmission
Hepatitis B virus (HBV) is a bloodborne and sexually transmitted virus. Rates of new infection and acute disease are
highest among adults, but chronic infection is more likely to occur in persons infected as infants or young children. Before hepatitis
B vaccination programs became routine in the United States, an estimated 30%--40% of chronic
infections are believed to have resulted from perinatal or early childhood transmission, even though <10% of reported cases of hepatitis B occurred
in children aged <10 years (1). Chronically infected persons are at increased lifetime risk for cirrhosis and
hepatocellular carcinoma (HCC) and also serve as the main reservoir for continued HBV transmission.
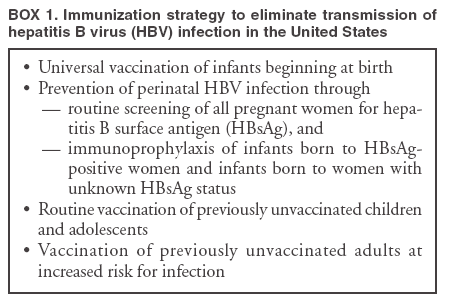
Hepatitis B vaccination is the most effective measure to prevent HBV infection and its consequences. Since they were
first issued in 1982, recommendations for hepatitis B vaccination have evolved into a comprehensive strategy to eliminate
HBV transmission in the United States (2--6)
(Box 1). A primary focus of this strategy is universal vaccination of
infants to prevent early childhood HBV infection and to eventually protect adolescents and adults from infection. Other components
include routine screening of all pregnant women for hepatitis B surface antigen (HBsAg) and postexposure immunoprophylaxis
of infants born to HBsAg-positive women, vaccination of children and adolescents who were not previously vaccinated,
and vaccination of unvaccinated adults at increased risk for infection.
To date, the immunization strategy has been implemented with considerable success. Recent estimates indicate that >95%
of pregnant women are tested for HBsAg, and case management has been effective in ensuring high levels of initiation
and
completion of postexposure immunoprophylaxis among identified infants born to HBsAg-positive women
(7). Hepatitis B vaccine has been successfully integrated into the childhood vaccine schedule, and infant vaccine coverage levels are
now equivalent to those of other vaccines in the childhood schedule. During 1990--2004, incidence of acute hepatitis B in
the United States declined 75%. The greatest decline (94%) occurred among children and adolescents, coincident with an
increase in hepatitis B vaccine coverage. As of 2004, among U.S. children aged 19--35 months, >92% had been fully vaccinated with
3 doses of hepatitis B vaccine (8). This success can be attributed in part to the established infrastructure for vaccine delivery
to children and to federal support for perinatal hepatitis B prevention programs.
Vaccine coverage among adolescents has also increased substantially. Preliminary data demonstrate that 50%--60%
of adolescents aged 13--15 years have records indicating vaccination (with 3 doses) against hepatitis B (CDC, unpublished
data, 2003). As of November 2005, a total of 34 states require vaccination for middle-school entry
(9). Certain programs provide hepatitis B vaccine to youth who engage in behaviors that place them at high risk for HBV infection (i.e., injection-drug
use, having more than one sex partner, and male sexual activity with other males), and adolescent hepatitis B vaccination
is included as a Health Plan Employer Data Information Set (HEDIS) measure
(10).
Despite these successes, challenges remain. Even with
improvements in the management of pregnant women,
only approximately 50% of expected births to HBsAg-positive women are identified (on the basis of application of
racial/ethnic-specific HBsAg prevalence estimates to U.S. natality data) for case management, which maximizes timely delivery
of postexposure immunoprophylaxis (11; CDC, unpublished data, 2004). The need for proper management of women
without prenatal care, including HBsAg testing at the time of admission for delivery and administration of the first dose of vaccine
to infants <12 hours of birth, is underscored by the higher prevalence of HBsAg seropositivity among these women than
among women who are screened prenatally (12). Even when maternal HBsAg testing does occur, certain infants of
HBsAg-positive mothers do not receive postexposure immunoprophylaxis because of testing errors and lapses in reporting of test results
(13), and infants of women with unknown HBsAg status at the time of delivery often do not receive a birth dose of vaccine
(14). Birth dose coverage in 2004 was only 46% (National Immunization Survey, unpublished data, 2004), and coverage has
not returned to levels from before July 1999 (54%), when recommendations were made to temporarily suspend administration
of hepatitis B vaccines at birth until vaccines that do not contain thimerosal as a preservative became available
(15). Among adolescents, efforts to prevent HBV transmission are hampered by the low rate of health-care visits in this age group
compared with that of young children and the frequency of initiation of high-risk behaviors.
To address these remaining challenges and accelerate progress toward elimination of HBV transmission in the United States,
the ACIP has updated the hepatitis B immunization recommendations for infants, children, and adolescents and supplemented
the recommendations with strategies for implementation. The recommendations and implementation strategies address prevention
of perinatal and early childhood transmission and routine vaccination of children and adolescents. A main focus is on
universal infant vaccination beginning at birth, which provides a "safety net" for prevention of perinatal infection, prevents early
childhood infections, facilitates implementation of universal vaccination recommendations, and prevents infections in adolescents
and adults. The second part of the ACIP statement, which includes updated recommendations and implementation strategies
to increase hepatitis B vaccination among unvaccinated adults, will be published separately
(16).
Major Updates to the Recommendations
This report provides updated recommendations and
approaches to address challenges in implementing the strategy
to eliminate HBV transmission in the United States. These include the following measures:
Improve prevention of perinatal and early childhood HBV transmission.
Implement delivery hospital policies and procedures, case-management programs, and laws and regulations to improve identification of infants born to HBsAg-positive mothers and to mothers with unknown HBsAg status at the time of delivery, ensure administration of
appropriate postexposure immunoprophylaxis to these infants beginning at birth, and administer a birth dose of hepatitis B vaccine
to medically stable infants who weigh >2,000 g and who are born to HBsAg-negative mothers.
Improve vaccine coverage of children and adolescents who were not previously vaccinated.
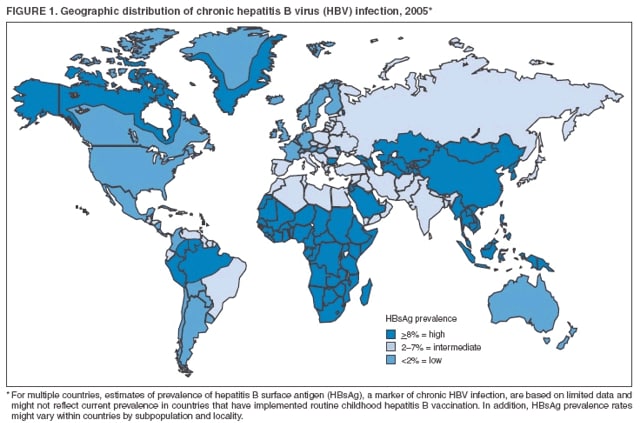
Implement immunization record reviews for all children aged 11--12 years and children and adolescents aged <19 years who were born in
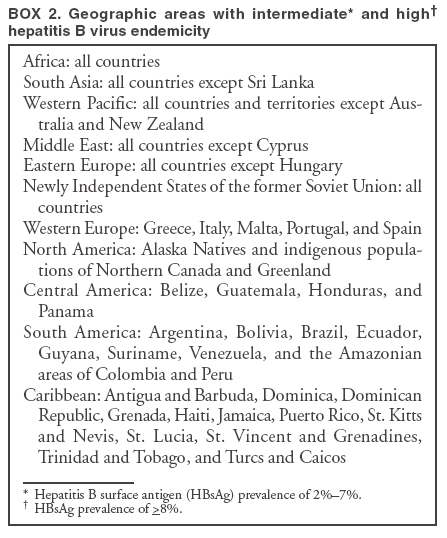
countries in which HBV endemicity is high or intermediate
(Figure 1 and Box 2); adopt hepatitis B vaccine requirements for
school entry; and vaccinate all unvaccinated adolescents in settings that provide health-care services to persons in this age group.
Background
Clinical Features and Natural History of HBV Infection
HBV is a 42-nm DNA virus classified in the
Hepadnaviridae family. The liver is the primary site of HBV replication. After
a susceptible person is exposed, the virus enters the liver via the bloodstream; no evidence exists indicating that the
virus replicates at mucosal surfaces. HBV infection can produce either asymptomatic or symptomatic infection. The
average incubation period is 90 days (range: 60--150 days) from
exposure to onset of jaundice and 60 days (range: 40--90 days)
from exposure to onset of abnormal serum alanine aminotransferase (ALT) levels
(17,18).
The onset of acute disease is usually insidious. Infants and young children (aged <10 years) are typically asymptomatic
(19). When present, clinical symptoms and signs might
include anorexia, malaise, nausea, vomiting, abdominal pain, and
jaundice. Extrahepatic manifestations of disease (e.g., skin rashes, arthralgias, and arthritis) also can occur
(20). The fatality rate among persons with reported acute hepatitis B is 0.5%--1.5%, with highest rates in adults aged >60 years
(21).
Although the consequences of acute hepatitis B can be
severe, the majority of serious sequelae associated with HBV
disease occur in persons who are chronically infected. Persons with chronic infection also serve as the major reservoir for
continued HBV transmission. Chronic infection occurs in approximately 90% of infected infants, 30% of infected children aged
<5 years, and <5% of infected persons aged
>5 years, with continuing viral replication in the liver and persistent viremia
(19,22--24). Primary infections also become chronic more frequently in immunosuppressed persons (e.g., hemodialysis patients
and persons with human immunodeficiency virus [HIV] infection)
(23,25,26). On the basis of data from follow-up studies
of persons infected with HBV as infants or young children, approximately 25% of those with chronic infection die
prematurely from cirrhosis or liver cancer; the majority remain asymptomatic until onset of cirrhosis or end-stage liver disease
(27--29).
No specific treatment exists for acute hepatitis B. Persons who have chronic HBV infection require medical evaluation
and regular monitoring (30,31). Therapeutic agents approved by the Food and Drug Administration (FDA) for treatment
of chronic hepatitis B can achieve sustained suppression of HBV replication and remission of liver disease in certain persons
(31). Periodic screening with alfa fetoprotein or imaging studies has been demonstrated to enhance early detection of HCC
(31). Chronically infected persons with HCC have been reported to have experienced long-term survival after resection or
ablation of small HCCs, and persons who were screened had a substantial survival advantage compared with historic controls
(31).
Reinfection or reactivation of latent HBV infection has been reported among certain groups of immunosuppressed
persons, including renal transplant recipients, HIV-infected patients, bone marrow transplant recipients, and patients
receiving chemotherapy (32--35). The frequency with which this phenomenon occurs is unknown.
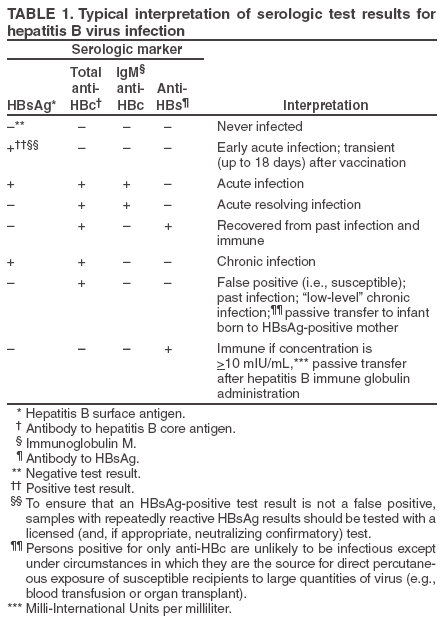
Interpretation of Serologic Markers of HBV Infection
The antigens and antibodies associated with HBV infection include HBsAg and antibody to HBsAg (anti-HBs), hepatitis
B core antigen (HBcAg) and antibody to HBcAg (anti-HBc), and hepatitis B e antigen (HBeAg) and antibody to HBeAg
(anti-HBe). At least one serologic marker is present during the different phases of HBV infection
(Table 1) (18,36). Serologic assays are commercially available for all markers
except HBcAg because no free HBcAg circulates in blood.
The presence of a confirmed HBsAg result is indicative of ongoing HBV infection. All HBsAg-positive persons should
be considered infectious. In newly infected persons, HBsAg is the only serologic marker detected during the first 3--5 weeks
after infection, and it persists for variable periods at very low levels. The average time from exposure to detection of HBsAg is
30 days (range: 6--60 days) (17,18). Highly sensitive single-sample nucleic acid tests can detect HBV DNA in the serum of
an infected person 10--20 days before detection of HBsAg
(37). Transient HBsAg positivity has been reported for up to 18
days after vaccination and is clinically insignificant
(38,39).
Anti-HBc appears at the onset of symptoms or liver test abnormalities in acute HBV infection and persists for life. Acute
or recently acquired infection can be distinguished by the presence of the IgM class of anti-HBc, which is detected at the onset
of acute hepatitis B and persists for up to 6 months if the disease resolves. In patients who develop chronic hepatitis B, IgM
anti-HBc can persist at low levels during viral replication and can result in positive tests for IgM anti-HBc
(40). In addition, false-positive IgM anti-HBc test results can occur. Because the positive predictive value is low in asymptomatic persons,
for diagnosis of acute hepatitis B, testing for IgM anti-HBc should be limited to persons with clinical evidence of acute
hepatitis or an epidemiologic link to a case.
In persons who recover from HBV infection, HBsAg is eliminated from the blood, usually within 3--4 months, and
anti-HBs develops during convalescence. The presence of anti-HBs typically indicates immunity from HBV infection. Infection
or immunization with one genotype of HBV confers immunity to all genotypes. In addition, anti-HBs can be detected for
several months after hepatitis B immune globulin (HBIG) administration. The majority of persons who recover from
natural infection will be positive for both anti-HBs and anti-HBc, whereas persons who respond to hepatitis B vaccine have only
anti-HBs. In persons who become chronically infected, HBsAg and anti-HBc persist, typically for life. HBsAg will
become undetectable in approximately 0.5%--2% of chronically infected persons yearly, and anti-HBs will occur in the majority
of these persons (41--44).
In certain persons, the only HBV serologic marker detected in serum is anti-HBc. Isolated anti-HBc can occur after
HBV infection among persons who have recovered but whose anti-HBs levels have waned or among persons in whom
anti-HBs failed to occur. Persons in the latter category include those with circulating HBsAg levels not detectable by commercial
assays. These persons are unlikely to be infectious except
under circumstances in which they are the source for direct
percutaneous exposure of susceptible recipients to substantial quantities of virus (e.g., through blood transfusion or following
liver transplantation) (45). HBV DNA has been detected in the blood of <5% of persons with isolated anti-HBc
(46). Typically, the frequency of isolated anti-HBc relates directly to the prevalence of HBV infection in the population. In populations with
a high prevalence of HBV infection, isolated anti-HBc likely indicates previous infection, with loss of anti-HBs. For persons
in populations with a low prevalence of HBV infection, an isolated anti-HBc result often represents a false-positive reaction.
The majority of these persons have a primary anti-HBs response after a 3-dose series of hepatitis B vaccine
(47,48). Infants who are born to HBsAg-positive mothers and who do not become infected might have detectable anti-HBc for
<24 months after birth from passively transferred maternal antibody.
HBeAg can be detected in the serum of persons with acute or chronic HBV infection. The presence of HBeAg
correlates with viral replication and high levels of virus (i.e., high infectivity)
(49,50). Anti-HBe correlates with the loss of
replicating virus and with lower levels of virus, although reversion to HBeAg positivity has been observed
(44).
Epidemiology of HBV Infection
Transmission
HBV is transmitted by percutaneous (i.e., puncture through the skin) or mucosal (i.e., direct contact with
mucous membranes) exposure to infectious blood or to body fluids that contain blood. All HBsAg-positive persons are infectious,
but those who are also HBeAg positive are more infectious
because their blood contains high titers of HBV (typically
107--109 virions/mL)
(49,50). Although HBsAg has been detected in multiple body fluids, only serum, semen, and saliva have
been demonstrated to be infectious (51,52). HBV is comparatively stable in the environment and remains viable for
>7 days on environmental surfaces at room temperature
(53). HBV at concentrations of
102--3 virions/mL can be present on environmental surfaces in the absence of any visible blood and still cause transmission
(53,54).
For infants and children, the two primary sources of HBV infection are perinatal transmission from infected mothers
and horizontal transmission from infected household contacts. Adolescents are at risk for HBV infection primarily through
high-risk sexual activity (i.e., sex with more than one partner and male sexual activity with other males) and injection-drug use
(21). Transmission of HBV via transfusion of blood and plasma-derived products is rare because of donor screening for HBsAg
and viral inactivation procedures.
For a newborn infant whose mother is positive for both HBsAg and HBeAg, the risk for chronic HBV infection is
70%--90%by age 6 months in the absence of postexposure immunoprophylaxis
(55--57). For infants of women who are
HBsAg positive but HBeAg negative, the risk for chronic
infection is <10% in the absence of postexposure immunoprophylaxis
(58--60). Rare cases of fulminant hepatitis B among perinatally infected infants also have been reported
(61,62). Studies suggest that breastfeeding by an
HBsAg-positive mother does not increase the risk for acquisition of HBV infection in the infant
(63).
Children who are not infected at birth remain at risk from long-term interpersonal contact with their infected mothers.
In one study, 38% of infants who were born to
HBsAg-positive mothers and who were not infected perinatally
became infected by age 4 years (64). In addition, children living with any chronically infected persons are at risk for
becoming infected through percutaneous or mucosal exposures to blood or infectious body fluids (e.g., sharing a toothbrush, contact with exudates
from dermatologic lesions, contact with HBsAg-contaminated surfaces). HBV transmission rates to susceptible household
contacts
of chronically infected persons have varied (range: 14%--60%)
(65,66). High rates of infection also have been reported
among unvaccinated long-term residents of institutions for the mentally handicapped
(67,68), and, in rare instances, person-to-person transmission has been reported in child care settings
(69,70).
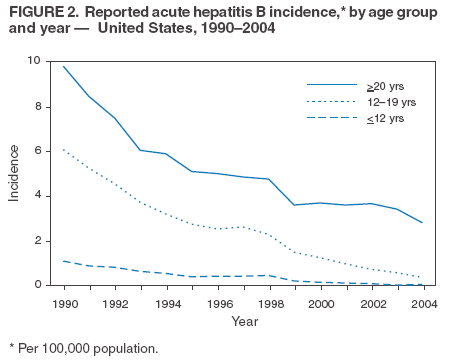
Incidence
During 1990--2004, overall incidence of reported acute hepatitis B declined 75%, from 8.5 to 2.1 per 100,000
population. The most dramatic declines occurred in the cohort of children to whom recommendations for routine infant and
adolescent vaccination have applied. Incidence among children aged <12 years and adolescents aged 12--19 years
declined 94%, from 1.1 to 0.36 and 6.1 to 2.8 per 100,000 population, respectively
(Figure 2). Since implementation of routine
childhood immunization, an estimated 6,800 perinatal infections and an additional 18,700 infections during the first 10 years of
life have been prevented annually in the United States
(71).
Although infections in infants and children aged <10 years represented <10% of all HBV infections before
implementation of childhood immunization programs, childhood infections resulted in an estimated 30%--40% of the chronic
HBV infections among persons who acquired their infections in the United States
(1). In two population-based studies
conducted among Asian/Pacific Islander children who were born in the United States before perinatal hepatitis B prevention
programs were widely implemented, 61%--66% of the chronic HBV infections occurred in children born to HBsAg-negative
mothers (72,73). A substantial proportion of these chronic infections would not have been prevented by a selective program
of identification and immunization of only infants born to HBsAg-positive mothers.
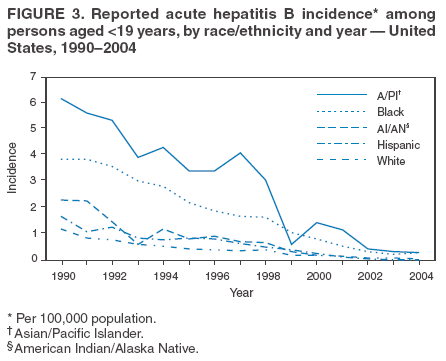
In addition to declines in incidence among all age groups, racial disparities in hepatitis B incidence among children
have been substantially reduced (Figure 3). The reduction of the disparity between Asian/Pacific Islander and other children
is consistent with recent observations noting a decline in seroprevalence of HBV infection after successful implementation
of routine hepatitis B vaccination among Asians who have recently immigrated to the United States
(74,75). However, as hepatitis B incidence has declined among U.S.-born children, unvaccinated foreign-born children account for a
high proportion of infections. During 2001--2002, of
19children born after 1991 in whom acute hepatitis B had been
verified, eight (42%) were foreign born (76).
Prevalence
In the U.S. population, the overall age-adjusted prevalence of HBV infection (including persons with chronic infection
and those with previous infection) was 4.9% in the third
National Health and Nutrition Examination Survey (NHANES
III, 1988--1994) (77). Foreign-born persons (particularly Asian/Pacific Islanders) who have emigrated from countries in
which HBV is endemic (Figure 1 and Box 2) contribute disproportionately to the burden of chronic HBV infection in the
United States. The prevalence of chronic HBV infection among foreign-born persons immigrating to the United States from
Central and Southeast Asia, the Middle East, and Africa varies (range: 5%--15%) and reflects the patterns of HBV infection in
the countries and regions of origin for these persons. During 1994--2003, approximately 40,000 immigrants with chronic
HBV infection were admitted annually to the United States for permanent residence
(78; CDC, unpublished data, 2005).
Prophylaxis AgainstHBV Infection
Hepatitis B Vaccine
HBsAg is the antigen used for hepatitis B vaccination
(79,80). Vaccine antigen can be purified from the plasma of
persons with chronic HBV infection or produced by recombinant DNA technology. Vaccines available in the United States
use recombinant DNA technology to express HBsAg in yeast, which is then purified from the cells by biochemical and
biophysical separation techniques (81,82). Hepatitis B vaccines licensed in the United States are formulated to contain
10--40 µg of HBsAg protein/mL. Since March 2000, hepatitis B vaccines produced for distribution in the United States do not
contain thimerosal as a preservative or contain only a trace amount (<1.0 mcg mercury/mL) from the manufacturing process
(83,84).
Hepatitis B vaccine is available as a single-antigen formulation and also in fixed combination with other vaccines.
Two single-antigen vaccines are available in the United States: Recombivax
HB® (Merck & Co., Inc., Whitehouse Station,
New Jersey) and Engerix-B® (GlaxoSmithKline Biologicals, Rixensart, Belgium). Of the three licensed combination vaccines,
one (Twinrix® [GlaxoSmithKline Biologicals, Rixensart, Belgium]) is used for vaccination of adults, and two
(Comvax® [Merck &
Co., Inc., Whitehouse Station, New Jersey] and
Pediarix® [GlaxoSmithKline Biologicals, Rixensart, Belgium]) are used
for vaccination of infants and young children. Twinrix contains recombinant HBsAg and inactivated hepatitis A
virus. Comvax contains recombinant HBsAg and Haemophilus
influenzae type b (Hib) polyribosylribitol phosphate conjugated to
Neisseria meningitidis outer membrane protein complex. Pediarix contains recombinant HBsAg, diphtheria and tetanus toxoids
and acellular pertussis adsorbed (DTaP), and inactivated poliovirus (IPV).
HBIG
HBIG provides passively acquired anti-HBs and temporary protection (i.e., 3--6 months) when administered in
standard doses. HBIG is typically used as an adjunct to hepatitis B vaccine for postexposure immunoprophylaxis to prevent
HBV infection. HBIG administered alone is the primary means of protection after an HBV exposure for nonresponders to
hepatitis B vaccination.
HBIG is prepared from the plasma of donors with high concentrations of anti-HBs. The plasma is screened to
eliminate donors who are positive for HBsAg, antibodies to HIV and hepatitis C virus (HCV), and HCV RNA. In addition,
proper manufacturing techniques for HBIG inactivate viruses (e.g., HBV, HCV, and HIV) from the final product
(85,86). No evidence exists that HBV, HCV, or HIV ever has been transmitted by HBIG commercially available in the United
States. HBIG that is commercially available in the United States does not contain thimerosal.
Vaccination Schedules and Results of Vaccination
Preexposure Vaccination
Infants and Children
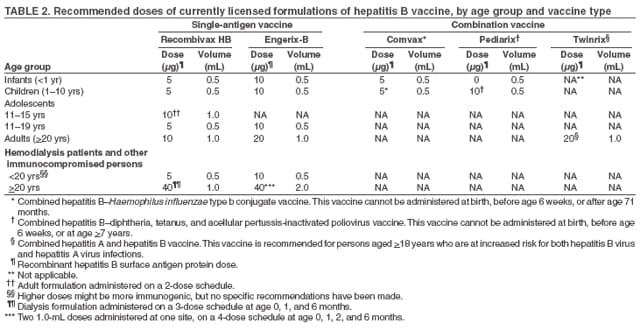
Primary vaccination consists of >3 intramuscular doses of hepatitis B vaccine
(Table 2). Vaccine schedules for infants and children
(Tables 3--5) are determined on the basis of immunogenicity
data and the need to integrate hepatitis B vaccine into
a harmonized childhood vaccination schedule. Although not all possible schedules for each product have been evaluated
in clinical trials, available licensed formulations for both single-antigen vaccines produce high (>95%) levels of
seroprotection among infants and children when administered
in multiple schedules (87--91).
The immunogenicity of the combined hepatitis B-Hib conjugate vaccine (Comvax) and the combined hepatitis
B-DTaP-IPV vaccine (Pediarix) is equivalent to that of their individual antigens administered separately. However, these
vaccines cannot be administered to infants aged <6 weeks; only single-antigen hepatitis B vaccine may be used for the birth dose.
Use of 4-dose hepatitis B vaccine schedules, including schedules with a birth dose, has not increased vaccine reactogenicity
(92,93). Anti-HBs responses after a 3-dose series of hepatitis B-containing combination vaccines among infants who were
previously vaccinated at birth with single-antigen hepatitis B vaccine are comparable to those observed after a 3-dose series
of combination vaccine without a birth dose
(93).
Birth Dose
Hepatitis B vaccine can be administered soon after birth with only minimal decrease in immunogenicity, compared
with administration at older ages, and no decrease in protective efficacy
(87). Administration of a birth dose of hepatitis B
vaccine is required for effective postexposure
immuno-prophylaxis to prevent perinatal HBV infection. Although
infants who require postexposure immunoprophylaxis should be identified by maternal HBsAg testing, administering a birth dose to infants
even without HBIG serves as a "safety net" to prevent perinatal infection among infants born to HBsAg-positive mothers who
are not identified because of errors in maternal HBsAg testing or failures in reporting of test results
(13). The birth dose also provides early protection to infants at risk for infection after the perinatal period. Administration of a birth dose has
been associated with higher rates of on-time completion of the hepatitis B vaccine series
(15,94). In certain populations, the birth dose has been associated with improved completion rates for all other infant vaccines
(95), although findings have not been consistent
(15,94).
Adolescents
Recommended vaccination schedules for adolescents balance available immunogenicity data with the need to
achieve compliance with vaccination in this age group (Tables 2 and
5). Both licensed single-antigen hepatitis B vaccines
administered intramuscularly at 0, 1, and 6 months produce a >95% sero-protection rate in adolescents. Equivalent seroprotection rates
are achieved among adolescents vaccinated at 0, 1--2, and 4 months and 0, 12, and 24 months. The adult (10
µg) dose of Recombivax-HB administered in a 2-dose schedule to children and adolescents aged 11--15 years at 0 and 4--6
months produces antibody levels equivalent to those obtained with the
5-µg dose administered on a 3-dose schedule
(96,97). However, no data on long-term antibody persistence or protection are available for 2-dose schedules. No combination
vaccines containing hepatitis B vaccine antigen are approved for use in adolescents aged 11--17 years.
Nonstandard Vaccine Schedules
No apparent effect on immunogenicity has been documented when minimum spacing of doses is not achieved
precisely. Increasing the interval between the first 2 doses has little effect on immunogenicity or final antibody concentration
(98--100). The third dose confers the maximum level of seroprotection but acts primarily as a booster and appears to provide optimal
long-term protection (101). Longer intervals between the last 2 doses result in higher final antibody levels but might increase the
risk for acquisition of HBV infection among persons who have a delayed response to vaccination. No differences
in immunogenicity have been observed when 1 or 2 doses of hepatitis B vaccine produced by one manufacturer are followed
by doses from a different manufacturer (102).
Response to Revaccination
A study of infants born to HBsAg-positive mothers who did not respond to a primary vaccine series indicated that all
those not infected with HBV responded satisfactorily to a
repeat 3-dose revaccination series (103). No data suggest that
children who have no detectable antibody after 6 doses of vaccine would benefit from additional doses.
Groups Requiring Different Vaccination Doses or Schedules
Preterm infants. Preterm infants weighing <2,000 g at birth have a decreased response to hepatitis B vaccine
administered before age 1 month (104--106). By age 1 month, medically stable preterm infants, regardless of initial birth weight
or gestational age, have a response to vaccination that is comparable to that of full-term infants
(107--110).
Hemodialysis patients and other immunocompromised persons.
Although data concerning the response of pediatric hemodialysis patients to vaccination with standard pediatric doses are lacking, protective levels of antibody occur in
75%--97% of those who receive higher dosages
(20-µg) on either the 3- or the 4-dose
schedule (111--114). Humoral response to hepatitis B vaccination is also reduced in other children and adolescents who are immunocompromised
(e.g., hematopoietic stem cell transplant recipients, patients undergoing chemotherapy, and HIV-infected persons)
(115--119). Modified dosing regimens, including a doubling of the standard antigen dose or administration of additional doses,
might increase response rates (120). However, data on response to these alternative vaccination schedules are limited
(121).
Immune Memory
Anti-HBs is the only easily measurable correlate of vaccine-induced protection. Immunocompetent persons who achieve
anti-HBs concentrations >10 mIU/mL after preexposure vaccination have virtually complete protection against both acute disease
and chronic infection even if anti-HBs concentrations
subsequently decline to <10 mIU/mL
(122--125). Although immunogenicity is lower among immunocompromised persons, those who achieve and maintain a protective antibody response before
exposure to HBV have a high level of protection from infection.
After primary immunization with hepatitis B vaccine, anti-HBs
concentrations decline rapidly within the first year and
more slowly thereafter. Among children who respond to a primary vaccine series with antibody levels
>10 mIU/mL, 15%--50% have low or undetectable
concentrations of anti-HBs (anti-HBs loss) 5--15 years after vaccination
(126--130). The persistence of detectable anti-HBs after vaccination, in the
absence of exposure to HBV, depends on the level of postvaccination
antibody concentration.
Despite declines in anti-HBs to <10 mIU/mL, nearly all vaccinated persons are still protected against HBV infection.
The mechanism for continued vaccine-induced protection is thought to be the preservation of immune memory through
selective expansion and differentiation of clones of antigen-specific B and T lymphocytes
(131). Persistence of vaccine-induced
immune
memory among persons who responded to a primary childhood vaccine series 13--23 years earlier but then had levels of
anti-HBs below 10 mIU/mL has been demonstrated by an anamnestic increase in anti-HBs levels in 67%--76% of these persons
2--4 weeks after administration of an additional vaccine dose
(132,133). Although direct measurement of immune memory
is not yet possible, these data indicate that a high proportion of vaccine recipients
retain immune memory and would develop an anti-HBs
response upon exposure to HBV.
Studies of cohorts of immunocompetent persons vaccinated as children or infants also indicate that, despite anti-HBs
loss years after immunization, nearly all vaccinated persons who respond to a primary series remain protected from HBV
infection. No clinical cases of hepatitis B have been observed in follow-up studies conducted 15--20 years after vaccination
among immunocompetent vaccinated persons with antibody levels
>10 mIU/mL. Certain studies have documented
breakthrough infections (detected by the presence of anti-HBc or HBV DNA) in a limited percentage of vaccinated persons
(130,131), but these infections are usually transient and
asymptomatic; chronic infections have been documented only rarely
(134). Breakthrough infections resulting in chronic
infection have been observed only among vaccinated infants born to
HBsAg-positive women.
Limited data are available on the duration of immune memory after hepatitis B vaccination in
immunocompromised persons (e.g., HIV-infected patients, dialysis patients, patients undergoing chemotherapy, or hematopoietic stem
cell transplant patients). No clinically important HBV infections have been documented among immunocompromised
persons who maintain protective levels of anti-HBs. In studies of long-term protection among HIV-infected persons,
breakthrough infections occurring after a decline in anti-HBs concentrations to <10 mIU/mL have been transient and asymptomatic
(135). However, among hemodialysis patients who respond to the vaccine, clinically significant HBV infection has been
documented in persons who have not maintained anti-HBs concentrations of
>10 mIU/mL (136).
Postexposure Prophylaxis
Both passive-active postexposure prophylaxis (PEP) with HBIG and hepatitis B vaccine and active PEP with hepatitis
B vaccine alone have been demonstrated to be highly effective in preventing transmission after exposure to HBV
(137--140). HBIG alone has also been demonstrated to be effective in preventing HBV transmission
(141--144), but with the availability of hepatitis B vaccine, HBIG typically is used as an adjunct to vaccination.
The major determinant of the effectiveness of PEP is early administration of the initial dose of vaccine. The effectiveness
of PEP diminishes the longer it is initiated after exposure
(17,145,146). Studies are limited on the maximum interval
after exposure during which PEP is effective, but the interval is unlikely to exceed 7 days for perinatal
(147) and needlestick (140--142) exposures and 14 days for sexual exposures
(122, 138,139,143,144).
No data are available on the efficacy of HBsAg-containing combination vaccines when used to complete the vaccine series
for PEP, but the efficacy of combination vaccines is expected to be similar to that of single-antigen vaccines because the
HBsAg component induces a comparable anti-HBs response.
Perinatal HBV Exposure
Passive-active PEP. PEP with hepatitis B vaccine and HBIG administered 12--24 hours after birth, followed by
completion of a 3-dose vaccine series, has been demonstrated to be 85%--95% effective in preventing acute and chronic HBV infection
in infants born to women who are positive for both HBsAg and HBeAg
(137). Although clinical trials have evaluated the
efficacy of passive-active PEP with hepatitis B vaccine and HBIG administered only within 24 hours of birth, studies of
passive immunoprophylaxis have demonstrated that HBIG provided protection when administered as late as 72 hours after
exposure. The majority of clinical trials have evaluated the efficacy of passive-active PEP when the second vaccine dose was
administered at age 1 month (137). Administration of HBIG plus vaccine at birth, 1 month, and 6 months and at birth, 2 months, and
6 months has demonstrated comparable efficacy in prevention of acute and chronic infection among infants born to
women who were both HBsAg and HBeAg positive (Cladd E. Stevens, MD, New York Blood Center, personal
communication, 1994).
Infants born to HBsAg-positive/HBeAg-negative mothers who receive passive-active PEP with HBIG and hepatitis
B vaccine should have the same high degree of protection as infants born to women who are HBsAg positive/HBeAg
positive. However, the efficacy of this regimen has not been examined in controlled clinical trials because the low infection rate
would require an unattainable sample size.
Active PEP. Active PEP with hepatitis B vaccine alone (i.e., without HBIG) is frequently used in certain remote areas
(e.g., Alaska and the Pacific Islands) where implementation of
maternal HBsAg testing is difficult because no access exists to
a laboratory. In randomized, placebo-controlled clinical trials, administration of hepatitis B vaccine in a 3- or 4-dose
schedule without HBIG beginning <12 hours after birth has been demonstrated to prevent 70%--95% of perinatal HBV
infections among infants born to women who are positive for both HBsAg and HBeAg
(58,148--152). Population-based studies in
areas with a high endemicity of HBV infection have demonstrated that active postexposure vaccination is highly effective
in preventing infection when the first dose is administered soon after birth, the second at age 1--2 months, and the third at
age 6--8 months (153--155).
Vaccine Safety
Hepatitis B vaccines have been demonstrated to be safe when administered to infants, children, adolescents, and
adults. Since 1982, an estimated >60 million adolescents and adults and >40 million infants and children have been vaccinated in
the United States.
Vaccine Reactogenicity
The most frequently reported side effects among persons receiving hepatitis B vaccine are pain at the injection
site (3%--29%) and fever >99.9° F(>37.7° C) (1%--6%)
(156,157). However, in placebo-controlled studies, these side
effects were reported no more frequently among persons
receiving hepatitis B vaccine than among persons receiving placebo
(87). Administration of hepatitis B vaccine soon after birth has not been associated with an increased rate of elevated
temperatures or microbiologic evaluations for possible sepsis in the first 21 days of life
(158).
Adverse Events
A causal association has been established between receipt of hepatitis B vaccine and anaphylaxis
(159). On the basis of data from the Vaccine Safety Datalink (VSD) project, the
estimated incidence of anaphylaxis among children and adolescents
who received hepatitis B vaccine is one case per 1.1 million vaccine doses distributed (95% confidence interval = 0.1--3.9)
(160).
Early postlicensure surveillance of adverse events suggested a possible association between Guillain-Barré syndrome
and receipt of the first dose of plasma-derived hepatitis B vaccine among U.S. adults
(161). However, in a subsequent analysis of Guillain-Barré syndrome cases reported to CDC, FDA, and vaccine manufacturers, among an estimated 2.5 million
adults who received >1 dose of recombinant hepatitis B vaccine during 1986--1990, the rate of Guillain-Barré
syndrome occurring after hepatitis B vaccination did not exceed the background rate among unvaccinated persons (CDC,
unpublished data, 1992). A review by persons with clinical expertise concluded that evidence was insufficient to reject or accept a
causal association between Guillain-Barré syndrome and hepatitis B vaccination
(159,162).
Multiple sclerosis (MS) has not been reported after hepatitis B vaccination among children. However, one retrospective
case-control study (163,164) reported an association between hepatitis B vaccine and MS among adults. Multiple other
studies (165--168) have demonstrated no association between hepatitis B vaccine and MS. Reviews of these data by panels of
persons with clinical expertise have favored rejection of a causal association between hepatitis B vaccination and MS
(169,170).
Chronic illnesses that have been reported in rare instances after hepatitis B vaccination include chronic fatigue
syndrome (171), neurologic disorders (e.g., leukoencephalitis, optic neuritis, and transverse myelitis)
(172--174), rheumatoid arthritis
(175,176), type 1 diabetes (177), and autoimmune disease
(178). No evidence of a causal association between these
conditions or other chronic illnesses and hepatitis B vaccine has been demonstrated
(159,169,170,179--182).
Reported episodes of alopecia (hair loss) after rechallenge with hepatitis B vaccine suggest that vaccination might, in
rare cases, trigger episodes of alopecia
(183). However, a population-based study determined no statistically
significant association between alopecia and hepatitis B vaccine
(184).
No evidence exists of a causal association between hepatitis B vaccination, including administration of the birth dose,
and sudden infant death syndrome (SIDS) or other causes of death during the first year of life
(185--187). Infant death rates, including rates of SIDS, declined substantially in the United States during the 1990s, coincident with an increase in
infant
hepatitis B vaccination coverage from <1% to >90% and implementation of efforts to reduce SIDS through infant
sleep positioning and separation from other persons in bed
(188).
The safety of hepatitis B vaccine and other vaccines is
assessed continuously through ongoing monitoring of data from VSD,
the Vaccine Adverse Events Reporting System (VAERS), and other surveillance systems. Any adverse events after vaccination should
be reported to VAERS; report forms and assistance are available from CDC at telephone 1-800-822-7967 or at
http://www.vaers.hhs.gov.
Contraindications and Precautions
Hepatitis B vaccination is contraindicated for persons with a history of hypersensitivity to yeast or to any
vaccine component (92,189--191). Despite a theoretic risk for allergic reaction to vaccination in persons with allergy to
Saccharomyces cerevisiae (baker's yeast), no evidence exists that documents adverse reactions after vaccination of persons with a history of
yeast allergy.
Persons with a history of serious adverse events (e.g., anaphylaxis) after receipt of hepatitis B vaccine should
not receive additional doses. As with other vaccines, vaccination of persons with moderate or severe acute illness, with or
without fever, should be deferred until the acute phase of the illness resolves
(192). Vaccination is not contraindicated in persons with a history of
MS, Guillain-Barré syndrome, autoimmune disease (e.g., systemic lupus erythematosis or rheumatoid arthritis), or other
chronic diseases.
Pregnancy is not a contraindication to vaccination. Limited data indicate no apparent risk for adverse events to
developing fetuses when hepatitis B vaccine is administered to pregnant women
(193). Current vaccines contain noninfectious
HBsAg and should cause no risk to the fetus.
Future Considerations
Implementation of the recommendations and strategies in this document should ultimately lead to the elimination of
HBV transmission in the United States. New information will have implications for this effort, and adjustments and changes
are expected to occur.
Long-Term Protection and Booster Doses
Studies are needed to assess long-term protection after vaccination and the possible need for booster doses of vaccine.
The longest follow-up studies of vaccine protection have been conducted in populations with an initially high endemicity of
HBV infection (i.e., >8% prevalence of chronic infection)
(130). Implementation of hepatitis B vaccination programs in
populations with a high endemicity of HBV infection has resulted in virtual elimination of new HBV infections by providing
vaccine-induced immunity to susceptible persons. In these populations, ongoing exposure of vaccinated persons to persons with chronic HBV infection might complicate future efforts to assess long-term hepatitis B vaccine efficacy. Assessment of efficacy provided
by hepatitis B immunization after 15--20 years will require studies among populations that continue to have exposures to
HBsAg-positive persons (e.g., communities of immigrants from highly endemic countries, populations of
injection-drug users, or health-care workers) and studies among populations with a low prevalence of infection.
Immunization Escape Mutants
Mutations in the S gene of HBV can lead to conformational changes in the
a determinant of the HBsAg protein, which
is the major target for neutralizing anti-HBs. These variants have been detected in humans infected with HBV, and concern
has been expressed that these variants might replicate in the presence of vaccine-induced anti-HBs or anti-HBs contained
in HBIG (194,195). Although no evidence suggests that S gene immunization escape mutants pose a threat to existing
programs using hepatitis B vaccines (196), further studies and enhanced surveillance to detect the emergence of these variants are
high priorities for monitoring the effectiveness of current vaccination strategies.
Recommendations for Hepatitis B Vaccination of Infants, Children,
and Adolescents
This section outlines updated ACIP recommendations and associated implementation strategies for hepatitis B
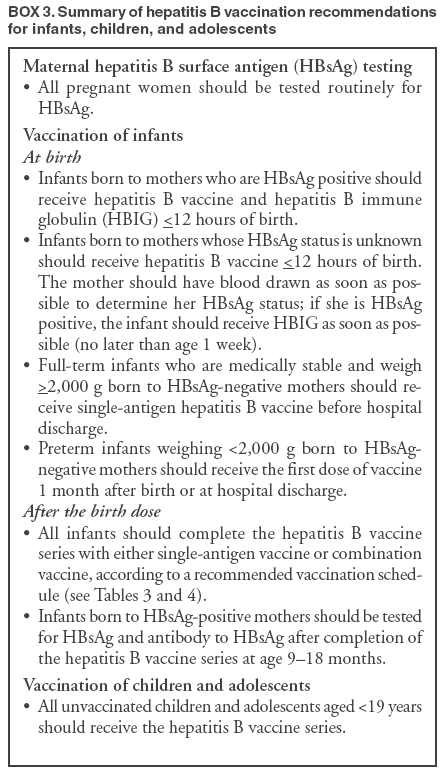
vaccination of infants, children, and adolescents. These recommendations have been summarized
(Box 3).
Prevention of Perinatal HBV Infection and Management of Pregnant Women
Recommendations
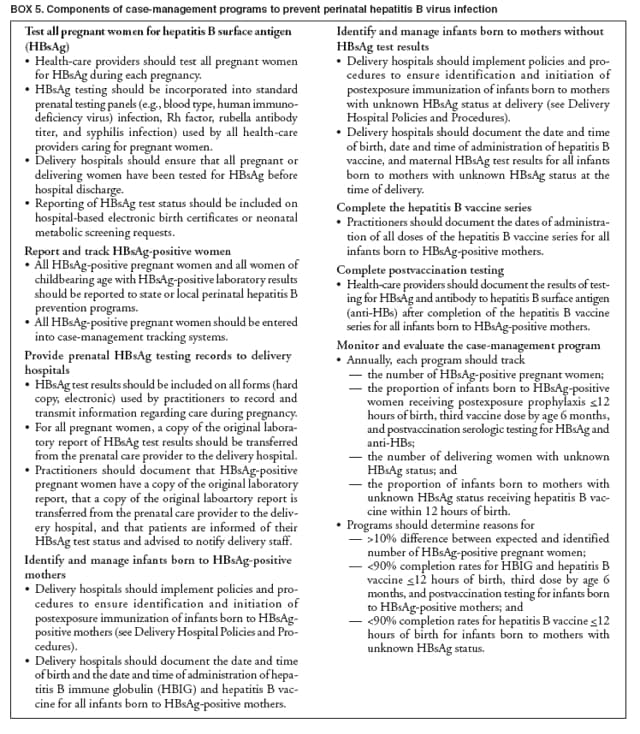
Prenatal HBsAg Testing
All pregnant women should be tested routinely for HBsAg during an early prenatal visit (e.g., first trimester) in each pregnancy,
even if they have been previously vaccinated or tested.
Women who were not screened prenatally, those who
engage in behaviors that put them at high risk for infection
(e.g., injection-drug use, having had more than one sex partner in the previous 6 months or an HBsAg-positive sex
partner, evaluation or treatment for a sexually transmitted disease [STD], or recent or current injection-drug use) and those
with clinical hepatitis should be tested at the time of admission to the hospital for delivery.
All laboratories that provide HBsAg testing of pregnant women should use an FDA-licensed or -approved HBsAg test
and should perform testing according to the manufacturer's labeling, including testing of initially reactive specimens with
a licensed neutralizing confirmatory test. When pregnant women are tested for HBsAg at the time of admission for
delivery, shortened testing protocols may be used and initially reactive results reported to expedite administration
of immunoprophylaxis to infants.
Women who are HBsAg positive should be referred to an appropriate case-management program to ensure that their
infants receive timely postexposure prophylaxis and follow-up (see Case-Management Programs to Prevent Perinatal HBV
Infection). In addition, a copy of the original laboratory report indicating
the pregnant woman's HBsAg status should be provided
to the hospital where delivery is planned and to the health-care provider who will care for the newborn.
Women who are HBsAg positive should be provided with or referred for appropriate counseling and medical
management (Appendix A). HBsAg-positive pregnant women should receive information concerning hepatitis B that discusses
--- modes of transmission;
--- perinatal concerns (e.g., infants born to
HBsAg-positive mothers may be breast fed);
--- prevention of HBV transmission to contacts, including the importance of postexposure prophylaxis for the
newborn infant and hepatitis B vaccination for household, sexual, and needle-sharing contacts;
--- substance abuse treatment, if appropriate; and
--- medical evaluation and possible treatment of chronic hepatitis B.
When HBsAg testing of pregnant women is not feasible (i.e., in remote areas without access to a laboratory), all
infants should receive hepatitis B vaccine
<12 hours of birth and should complete the hepatitis B vaccine
series according to a recommended schedule for infants born to HBsAg-positive mothers (Tables 2 and
3).
Management of Infants Born to Women Who Are HBsAg Positive
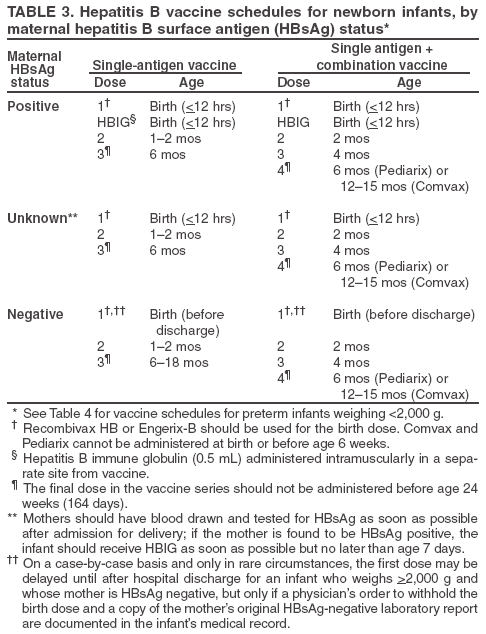
All infants born to HBsAg-positive women should receive single-antigen hepatitis B vaccine (Table 2) and HBIG
(0.5 mL) <12 hours of birth, administered at different injection sites. The vaccine series should be completed according to
a recommended schedule for infants born to HBsAg-positive mothers (Table 3). The final dose in the vaccine series
should not be administered before age 24 weeks (164 days).
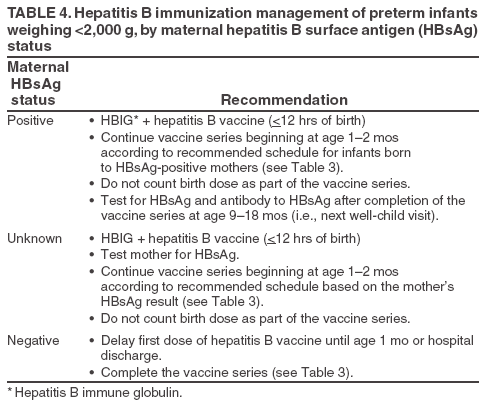
For preterm infants weighing <2,000 g, the initial vaccine dose (birth dose) should not be counted as part of the
vaccine series because of the potentially reduced immunogenicity
of hepatitis B vaccine in these infants; 3 additional doses
of vaccine (for a total of 4 doses) should be administered beginning when the infant reaches age 1 month (Tables 3 and
4).
Postvaccination testing for anti-HBs and HBsAg should be performed after completion of the vaccine series, at age
9--18 months (generally at the next well-child visit). Testing should not be performed before age 9 months to avoid detection
of anti-HBs from HBIG administered during infancy and to maximize the likelihood of detecting late HBV infection.
Anti-HBc testing of infants is not recommended because passively acquired maternal anti-HBc might be detected in
infants born to HBV-infected mothers to age 24 months.
--- HBsAg-negative infants with anti-HBs levels >10 mIU/mL are protected and need no further medical management.
--- HBsAg-negative infants with anti-HBs levels <10
mIU/mL should be revaccinated with a second 3-dose series and
retested 1--2 months after the final dose of vaccine.
--- Infants who are HBsAg positive should receive appropriate follow-up (Appendix A).
Infants of HBsAg-positive mothers may be breast fed
beginning immediately after birth.
Although not indicated in the manufacturer's package
labeling, HBsAg-containing combination vaccines may be used
for infants aged >6 weeks born to HBsAg-positive
mothers to complete the vaccine series after receipt
of a birth dose of single-antigen hepatitis B vaccine and HBIG.
Management of Infants Born to Women with Unknown HBsAg Status
Women admitted for delivery without documentation of HBsAg test results should have blood drawn and tested as
soon as possible after admission.
While test results are pending, all infants born to women without documentation of HBsAg test results should
receive the first dose of single-antigen hepatitis B vaccine (without HBIG)
<12 hours of birth (Tables 2 and 3).
--- If the mother is determined to be HBsAg positive, her infant should receive HBIG as soon as possible but no later
than age 7 days, and the vaccine series should be completed according to a recommended schedule for infants born
to HBsAg-positive mothers (Table 3).
--- If the mother is determined to be HBsAg negative, the vaccine series should be completed according to
a recommended schedule for infants born to HBsAg-negative mothers (Table 3).
--- If the mother has never been tested to determine her HBsAg status, the vaccine series should be completed
according to a recommended schedule for infants born to HBsAg-positive mothers (Table 3). Administration of HBIG is
not necessary for these infants.
Because of the potentially decreased immunogenicity of vaccine in preterm infants weighing <2,000 g,
these infants should receive both single-antigen hepatitis B vaccine and HBIG (0.5 mL) if the mother's HBsAg status cannot
be determined <12 hours of birth. The birth dose of vaccine should not be counted as part of the 3 doses required
to complete the vaccine series; 3 additional doses of vaccine (for a total of 4 doses) should be administered according to
a recommended schedule on the basis of the mother's HBsAg test result (Table 3).
Vaccination of Pregnant Women
Pregnant women who are identified as being at risk for HBV infection during pregnancy (e.g., having more than one
sex partner during the previous 6 months, been evaluated or treated for an STD, recent or current injection-drug use,
or having had an HBsAg-positive sex partner) should be vaccinated.
Pregnant women at risk for HBV infection during pregnancy should be counseled concerning other methods to
prevent HBV infection.
Implementation
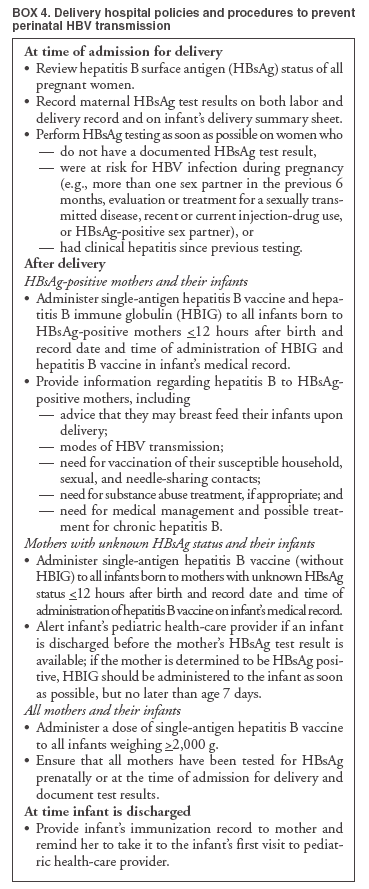
Delivery Hospital Policies and Procedures
All delivery hospitals should implement policies and procedures
(Box 4) to ensure 1) identification of infants born
to HBsAg-positive mothers and infants born to mothers with unknown HBsAg status (see Prenatal HBsAg Testing), and
2) initiation of immunization for these infants. Such policies and procedures should include the following standing orders:
--- for all pregnant women, review of HBsAg test results at the time of admission for delivery;
--- for women who do not have a documented HBsAg test result, HBsAg testing as soon as possible after
admission for delivery;
--- identification and management of all infants born to HBsAg-positive mothers;
--- identification and management of all infants born to mothers with unknown HBsAg status; and
--- for all infants, documentation on the infant's medical record of maternal HBsAg test results, infant hepatitis B
vaccine administration, and administration of HBIG (if appropriate).
Delivery hospitals should enroll in the federally funded Vaccines for Children (VFC) program to obtain free hepatitis
B vaccine for administration of the birth dose to newborns who are eligible (i.e., Medicaid eligible, American Indian
or Alaska Native, underinsured, or uninsured).
Case-Management Programs to Prevent Perinatal HBV Infection
States and localities should establish case-management programs
(Box 5), including appropriate policies, procedures,
laws, and regulations, to ensure that
--- all pregnant women are tested for HBsAg during each pregnancy, and
--- infants born to HBsAg-positive women and infants born to women with unknown HBsAg status
receive recommended case management.
The location of these programs and the methods by which they operate will depend on multiple factors (e.g.,
population density and annual caseload of HBsAg-positive women). Programs may be located in state or local health
departments, private health-care systems (e.g., health maintenance organizations), or institutions (e.g., correctional facility
systems). Program administrators will need to work with prenatal care providers, delivery hospital staff, pediatric care
providers, private health-care systems, and health departments.
Universal Vaccination of Infants
Recommendations
All infants should receive the hepatitis B vaccine series as part of the recommended childhood immunization
schedule (Table 5 and Appendix B). (For recommendations on management of infants born to HBsAg-positive mothers and
infants born to mothers with unknown HBsAg status, see Prevention of Perinatal HBV Infection and Management of
Pregnant Women.)
For all medically stable infants weighing
>2,000 g at birth and born to HBsAg-negative mothers, the first dose of
vaccine should be administered before hospital discharge. Only single-antigen hepatitis B vaccine should be used for the
birth dose.
On a case-by-case basis and only in rare circumstances, the first dose may be delayed until after hospital discharge for
an infant who weighs >2,000 g and whose mother is HBsAg negative.
--- When such a decision is made, a physician's order to withhold the birth dose and a copy of the original
laboratory report indicating that the mother was HBsAg negative during this pregnancy should be placed in the infant's
medical record.
--- For infants who do not receive a first dose before hospital discharge, the first dose should be administered no later
than age 2 months.
--- Situations in which the birth dose should not be
delayed include any high-risk sexual or drug-using practices of
the infant's mother during pregnancy (e.g., having had more than one sex partner during the previous 6 months or
an HBsAg-positive sex partner, evaluation or treatment for an STD, or recent or current injection-drug use) and
expected poor compliance with follow-up to initiate the vaccine series.
Preterm infants weighing <2,000 g and born to HBsAg-negative mothers should have their first vaccine dose
delayed until 1 month after birth or hospital discharge (Table 4). For these infants, a copy of the original laboratory report
indicating that the mother was HBsAg negative during this pregnancy should be placed in the infant's medical record.
The vaccine series should be completed according to a recommended schedule with either single-antigen vaccine or
a combination vaccine that contains the hepatitis B vaccine antigen (e.g., Hib-hepatitis B or
DTaP-IPV-hepatitis B) (Table 2). The final dose in the vaccine series should not be administered before age 24 weeks (164 days).
Administration of 4 doses of hepatitis B vaccine to
infants is permissible in certain situations (e.g., when
combination vaccines are administered after the birth dose).
In populations with currently or previously high rates of childhood HBV infection (i.e., Alaska Natives; Pacific
Islanders; and immigrant families from Asia, Africa, and other regions with intermediate or high endemic rates of infection [Figure 1 and Box 2]), the first dose of hepatitis B vaccine should be administered at birth and the final dose at age 6--12 months.
Implementation
All delivery hospitals should implement standing orders for administration of hepatitis B vaccination as part of
routine medical care of all medically stable infants weighing
>2,000 g at birth (Box 4).
All delivery hospitals should implement policies and procedures for management of infants weighing <2,000 g at
birth, including the following:
--- ensuring initiation of postexposure immunization of infants born to HBsAg-positive mothers and infants born
to mothers not screened for HBsAg prenatally (see Prevention of Perinatal HBV Infection and Management of
Pregnant Women), and
--- documentation of maternal HBsAg test results on the infant's medical record.
Prenatal care education should include information
regarding the rationale for and importance of newborn hepatitis
B vaccination.
States are encouraged to adopt regulations or laws that require hepatitis B vaccination for entry into child care and also
for entry into kindergarten and/or elementary school to ensure high vaccine coverage among infants and children.
Vaccination of Children and Adolescents Who Were Not Previously Vaccinated
Recommendations
Hepatitis B vaccination is recommended for all children and adolescents aged <19 years.
Children and adolescents who have not previously received hepatitis B vaccine should be vaccinated routinely at any
age with an appropriate dose and schedule (Tables 2 and
5). Selection of a vaccine schedule should consider the need
to achieve completion of the vaccine series. In all settings, vaccination should be initiated even though completion of
the vaccine series might not be ensured.
Implementation
To ensure high vaccination coverage among children and adolescents, the following measures are recommended:
--- All children aged 11--12 years should have a review of their immunization records and should complete the
vaccine series if they were not previously vaccinated or were incompletely vaccinated.
--- All children and adolescents aged <19 years (including internationally adopted children) who were born in Asia,
the Pacific Islands, Africa, or other intermediate- or high-endemic countries (Figure 1 and
Box 2) or who have at least
one parent who was born in one of these areas should have a review of their immunization records and should complete
the vaccine series if they were not previously vaccinated or were incompletely vaccinated.
--- States are encouraged to adopt regulations or laws that require hepatitis B vaccination before entry into middle
school or its equivalent.
--- Vaccination requirements should be considered for older high school students and for students before college
entry, when feasible.
--- States are encouraged to expand or implement immunization registries to include adolescents.
--- Hepatitis B vaccine should be offered to all unvaccinated adolescents in settings that provide health-care services to
this age group (Box 6), particularly those who engage in behaviors that place them at high risk for HBV infection.
Acknowledgments
Review of this report was provided by the following persons: R. Palmer Beasley, MD, School of Public Health, University of
Texas Health Science Center at Houston, Houston, Texas; F. Blaine Hollinger, MD, Baylor College of Medicine, Houston, Texas; Neal
A. Halsey, MD, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins School of Medicine, Baltimore, Maryland;
and Craig N. Shapiro, MD, Office of Global Health Affairs, U.S. Department of Health and Human Services, Washington, DC.
Allison Greenspan, MPH, Division of Viral Hepatitis, National Center for Infectious Diseases, CDC, provided vital assistance in the
preparation of this report.
References
West DJ, Margolis HS. Prevention of hepatitis B virus infection in the United States: a pediatric perspective. Pediatr Infect Dis J 1992;11:866--74.
Immunization Action Coalition. Hepatitis B prevention mandates. St. Paul, MN: Immunization Action Coalition; 2005. Available at
http://www.immunize.org/laws/hepb.htm.
National Committee for Quality Assurance. State of health care quality
report, 2003: adolescent immunization status. Washington, DC:
National Committee for Quality Assurance; 2005. Available at
http://
www.ncqa.org/sohc2003/adolescent_immunization_status.htm.
CDC. Hepatitis surveillance: report no. 56. Atlanta, GA: US Department of Health and Human Services, CDC; 1996.
Silverman NS, Darby MJ, Ronkin SL, Wapner RJ. Hepatitis B prevalence in an unregistered prenatal population. Implications for
neonatal therapy. JAMA 1991;266:2852--5.
Anderson TA, Wexler DL. States report hundreds of medical errors in perinatal hepatitis B prevention. St. Paul, MN: Immunization
Action Coalition; 2005. Available at
http://www.immunize.org/catg.d/p2062.htm.
Thomas AR, Fiore AE, Corwith HL, Cieslak PR, Margolis HS. Hepatitis B vaccine coverage among infants born to women without
prenatal screening for hepatitis B virus infection: effects of the Joint Statement on Thimerosal in Vaccines. Pediatr Infect Dis J 2004; 23:313--8.
Luman ET, Fiore AE, Strine TW, Barker LE. Impact of thimerosal-related changes in hepatitis B vaccine birth-dose recommendations
on childhood vaccination coverage. JAMA 2004;291:2351--8.
CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations
of the Advisory Committee on Immunization Practices (ACIP). Part 2: Immunization of adults. MMWR. In press.
Krugman S, Overby LR, Mushahwar IK, Ling CM, Frosner GG, Deinhardt F. Viral hepatitis, type B: studies on natural history and prevention
re-examined. N Engl J Med 1979;300:101--6.
Hoofnagle JH, DiBisceglie AM. Serologic diagnosis of acute and chronic viral hepatitis. Semin Liver Dis 1991;11:73--83.
McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and
subsequent development of the carrier state. J Infect Dis 1985;151:599--603.
Dienstag JL. Immunopathogenesis of the extrahepatic manifestations of hepatitis B virus infections. Springer Semin Immunopathol 1981;3:
461--72.
CDC. Hepatitis surveillance: report number 60. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 2005.
Edmunds WJ, Medley GF, Nokes DJ, Hall AJ, Whittle HC. The influence of age on the development of the hepatitis B carrier state. Proc Biol
Sci 1993;253:197--201.
Hyams KC. Risks of chronicity following acute hepatitis B virus infection: a review. Clin Infect Dis 1995;20:992--1000.
Beasley RP, Hwang LY, Lee GC, et al. Prevention of perinatally transmitted hepatitis B virus infections with hepatitis B immune globulin
and hepatitis B vaccine. Lancet 1983;2:1099--102.
Hadler SC, Judson FN, O'Malley PM, et al. Outcome of hepatitis B virus infection in homosexual men and its relation to prior
human immunodeficiency virus infection. J Infect Dis 1991;163:454--9.
Polish LB, Shapiro CN, Bauer F, et al. Nosocomial transmission of hepatitis B virus associated with the use of a spring-loaded finger-stick device.
N Engl J Med 1992;326:721--5.
Beasley RP, Hwang LY, Lin CC, Chin CS. Hepatocellular carcinoma and hepatitis B virus: a prospective study of 22,707 men in Taiwan.
Lancet 1981;2:1129--33.
Hoofnagle JH, Shafritz DA, Popper H. Chronic type B hepatitis and the "healthy" HBsAg carrier state. Hepatology 1987;7:758--63.
McMahon BJ, Alberts SR, Wainwright RB, Bulkow L, Lanier AP. Hepatitis B-related sequelae: prospective study in 1400 hepatitis B
surface antigen-positive Alaska Native carriers. Arch Intern Med 1990; 150:1051--4.
Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2001;34: 1225--41.
Lok AS, McMahon BJ. Chronic hepatitis B: update of recommendations. Hepatology 2004;39:857--61.
Ortiz-Interian CJ, de Medina MD, Perez GO, et al. Recurrence and clearance of hepatitis B surface antigenemia in a dialysis patient infected
with the human immunodeficiency virus. Am J Kidney Dis 1990;16:154--6.
Davis CL, Gretch DR, Carithers RL Jr. Hepatitis B and transplantation. Infect Dis Clin North Am 1995;9:925--41.
Martin BA, Rowe JM, Kouides PA, DiPersio JF. Hepatitis B reactivation following allogeneic bone marrow transplantation: case report and review
of the literature. Bone Marrow Transplant 1995;15:145--8.
Law JK, Ho JK, Hoskins PJ, Erb SR, Steinbrecher UP, Yoshida EM. Fatal reactivation of hepatitis B post-chemotherapy for lymphoma in
a hepatitis B surface antigen-negative, hepatitis B core antibody-positive patient: potential implications for future prophylaxis
recommendations. Leuk Lymphoma 2005;46:1085--9.
Hollinger FB, Liang TJ. Hepatitis B virus. In: Knipe DM, Howley PM, Griffin DE, et al., eds. Fields virology. 4th ed. Philadelphia, PA:
Lippincott Williams & Wilkins; 2001.
Biswas R, Tabor E, Hsia CC, et al. Comparative sensitivity of HBV NATs and HBsAg assays for detection of acute HBV infection.
Transfusion 2003;43:788--98.
Kloster B, Kramer R, Eastlund T, Grossman B, Zarvan B. Hepatitis B surface antigenemia in blood donors following vaccination.
Transfusion 1995;35:475--7.
Lunn ER, Hoggarth BJ, Cook WJ. Prolonged hepatitis B surface antigenemia after vaccination. Pediatrics 2000;105:E81--2.
Kao JH, Chen PJ, Lai MY, Chen DS. Acute exacerbations of chronic hepatitis B are rarely associated with superinfection of hepatitis B
virus. Hepatology 2001;34(4 Pt 1):817--23.
Alward WL, McMahon BJ, Hall DB, Heyward WL, Francis DP, Bender TR. The long-term serological course of asymptomatic hepatitis B
virus carriers and the development of primary hepatocellular carcinoma. J Infect Dis 1985;151:604--9.
Liaw YF, Sheen IS, Chen TJ, Chu CM, Pao CC. Incidence, determinants and significance of delayed clearance of serum HBsAg in chronic
hepatitis B virus infection: a prospective study. Hepatology 1991;13: 627--31.
Adachi H, Kaneko S, Matsushita E, Inagaki Y, Unoura M, Kobayashi K. Clearance of HBsAg in seven patients with chronic hepatitis
B. Hepatology 1992;16:1334--7.
McMahon BJ, Holck P, Bulkow L, Snowball M. Serologic and clinical outcomes of 1536 Alaska Natives chronically infected with hepatitis B
virus. Ann Intern Med 2001;135:759--68.
De Feo TM, Poli F, Mozzi F, Moretti MP, Scalamogna M. Risk of transmission of hepatitis B virus from anti-HBc positive cadaveric organ
donors: a collaborative study. Transplantation Proc 2005;37: 1238--9.
Silva AE, McMahon BJ, Parkinson AJ, Sjogren MH, Hoofnagle JH, Di Bisceglie AM. Hepatitis B virus DNA in persons with isolated antibody
to hepatitis B core antigen who subsequently received hepatitis B vaccine. Clin Infect Dis 1998;26:895--7.
Lai CL, Lau JY, Yeoh EK, Chang WK, Lin HJ. Significance of isolated anti-HBc seropositivity by ELISA: implications and the role
of radioimmunoassay. J Med Virol 1992;36:180--3.
McMahon BJ, Parkinson AJ, Helminiak C, et al. Response to hepatitis B vaccine of persons positive for antibody to hepatitis B core
antigen. Gastroenterology 1992;103:590--4.
Alter HJ, Seeff LB, Kaplan PM, et al. Type B hepatitis: the infectivity of blood positive for e antigen and DNA polymerase after
accidental needlestick exposure. N Engl J Med 1976;295:909--13.
Shikata T, Karasawa T, Abe K, et al. Hepatitis B e antigen and infectivity of hepatitis B virus. J Infect Dis 1977;136:571--6.
Alter HJ, Purcell RH, Gerin JL, et al. Transmission of hepatitis B to chimpanzees by hepatitis B surface antigen-positive saliva and semen.
Infect Immun 1977;16:928--33.
Bancroft WH, Snitbhan R, Scott RM, et al. Transmission of hepatitis B virus to gibbons by exposure to human saliva containing hepatitis B
surface antigen. J Infect Dis 1977;135:79--85.
Bond WW, Favero MS, Petersen NJ, Gravelle CR, Ebert JW, Maynard JE. Survival of hepatitis B virus after drying and storage for one
week. Lancet 1981;1(8219):550--1.
Favero MS, Bond WW, Petersen NJ, Berquist KR, Maynard JE. Detection methods for study of the stability of hepatitis B antigen on surfaces.
J Infect Dis 1974;129:210--2.
Okada K, Kamiyama I, Inomata M, Imai M, Miyakawa Y. e antigen and anti-e in the serum of asymptomatic carrier mothers as indicators
of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med 1976;294:746--9.
Beasley RP, Trepo C, Stevens CE, Szmuness W. The e antigen and vertical transmission of hepatitis B surface antigen. Am J
Epidemiol 1977;105:94--8.
Wong VC, Ip HM, Reesink HW, et al. Prevention of the HBsAg carrier state in newborn infants of mothers who are chronic carriers of HBsAg
and HBeAg by administration of hepatitis-B vaccine and hepatitis-B immunoglobulin: double-blind randomised placebo-controlled study.
Lancet 1984;1(8383):921--6.
Stevens CE, Neurath RA, Beasley RP, Szmuness W. HBeAg and anti-HBe detection by radioimmunoassay: correlation with vertical transmission
of hepatitis B virus in Taiwan. J Med Virol 1979;3:237--41.
Xu ZY, Liu CB, Francis DP, et al. Prevention of perinatal acquisition of hepatitis B virus carriage using vaccine: preliminary report of a
randomized, double-blind placebo-controlled and comparative trial. Pediatrics 1985;76:713--8.
Stevens CE, Toy PT, Tong MJ, et al. Perinatal hepatitis B virus transmission in the United States: prevention by passive-active
immunization. JAMA 1985;253:1740--5.
Fawaz KA, Grady GF, Kaplan MM, Gellis SS. Repetitive maternal-fetal transmission of fatal hepatitis B. N Engl J Med 1975;293: 1357--9.
Beasley RP, Stevens CE, Shiao IS, Meng HC. Evidence against breast-feeding as a mechanism for vertical transmission of hepatitis B.
Lancet 1975;2(7938):740--1.
Beasley RP, Hwang LY. Postnatal infectivity of hepatitis B surface antigen-carrier mothers. J Infect Dis 1983;147:185--90.
Steinberg SC, Alter HJ, Leventhal BG. The risk of hepatitis transmission to family contacts of leukemia patients. J Pediatr 1975;87: 753--6.
Nordenfelt E, Dahlquist E. HBsAg positive adopted children as a cause of intrafamilial spread of hepatitis B. Scand J Infect Dis 1978; 10:161--3.
Perrillo RP, Storch GA, Bodicky CJ, Campbell CR, Sanders GE. Survey of hepatitis B viral markers at a public day school and a
residential institution sharing mentally handicapped students. J Infect Dis 1984;149:796--800.
Perrillo RP, Strang S, Lowry OH. Different operating conditions affect risk of hepatitis B virus infection at two residential institutions for
the mentally disabled. Am J Epidemiol 1986;123:690--8.
Shapiro CN, McCaig LF, Gensheimer KF, et al. Hepatitis B virus transmission between children in day care. Pediatr Infect Dis J 1989; 8:870--5.
Deseda CC, Shapiro CN, Carroll K, Hinds W. Hepatitis B virus transmission between a child and staff member at a day-care center. Pediatr
Infect Dis J 1994;13:828--30.
Armstrong GL, Mast EE, Wojczynski M, Margolis HS. Childhood hepatitis B virus infections in the United States before hepatitis
B immunization. Pediatrics 2001;108:1123--8.
Hurie MB, Mast EE, Davis JP. Horizontal transmission of hepatitis B virus infection to United States-born children of Hmong refugees.
Pediatrics 1992;89:269--73.
Mahoney FJ, Lawrence M, Scott C, Le Q, Lambert S, Farley TA. Continuing risk for hepatitis B virus transmission among Southeast Asian
infants in Louisiana. Pediatrics 1995;96:1113--6.
Fiore A, Neeman R, Lee S, et al. Seroprevalence of hepatitis B virus (HBV) infection among Asian immigrants and their U.S.-born children
in Georgia [Abstract 586]. 41st annual meeting of the Infectious Diseases Society of America, San Diego, California, October 9--12, 2003.
Perz JF, Elm JL, Huggler JI, Farrington LA, Fiore AE, Effler PV. Effectiveness of universal infant hepatitis B vaccination program in
Hawaii [Abstract WA3-03]. Proceedings of the 11th International Symposium on Viral Hepatitis and Liver Disease, April 6--10, 2003, Sydney, Australia.
McQuillan GM, Coleman PJ, Kruszon-Moran D, Moyer LA, Lambert SB, Margolis HS. Prevalence of hepatitis B virus infection in the
United States: the National Health and Nutrition Examination Surveys, 1976 through 1994. Am J Public Health 1999;89:14--8.
US Department of Homeland Security. 2003 Yearbook of immigration statistics. Washington, DC: US Department of Homeland Security; 2004.
Purcell RH, Gerin JL. Hepatitis B subunit vaccine: a preliminary report of safety and efficacy tests in chimpanzees. Am J Med Sci
1975;270:395--9.
Hilleman MR, McAleer WJ, Buynak EB, McLean AA. Quality and safety of human hepatitis B vaccine. Dev Biol Stand 1983;54:3--12.
Emini EA, Ellis RW, Miller WJ, McAleer WJ, Scolnick EM, Gerety RJ. Production and immunological analysis of recombinant hepatitis B
vaccine. J Infect 1986;13(Suppl A):3--9.
Stephenne J. Development and production aspects of a recombinant yeast-derived hepatitis B vaccine. Vaccine 1990;8(Suppl):S69--73.
Wells MA, Wittek AE, Epstein JS, et al. Inactivation and partition of human T-cell lymphotrophic virus, type III, during ethanol fractionation
of plasma. Transfusion 1986;26:210--3.
Greenberg DP. Pediatric experience with recombinant hepatitis B vaccines and relevant safety and immunogenicity studies. Pediatr Infect Dis
J 1993;12:438--45.
Goldfarb J, Baley J, Medendorp SV, et al. Comparative study of the immunogenicity and safety of two dosing schedules of Engerix-B hepatitis
B vaccine in neonates. Pediatr Infect Dis J 1994;13:18--22.
Greenberg DP, Vadheim CM, Marcy SM, et al. Safety and immunogenicity of a recombinant hepatitis B vaccine administered to infants at 2, 4
and 6 months of age: the Kaiser-UCLA Vaccine Study Group. Vaccine 1996;14:811--6.
Greenberg DP, Vadheim CM, Wong VK, et al. Comparative safety and immunogenicity of two recombinant hepatitis B vaccines administered
to infants at two, four and six months of age. Pediatr Infect Dis J 1996;15:590--6.
Greenberg DP, Wong VK, Partridge S, Howe BJ, Ward JI. Safety and immunogenicity of a combination diphtheria-tetanus toxoids-
acellular pertussis-hepatitis B vaccine administered at two, four and six months of age compared with monovalent hepatitis B vaccine administered at
birth, one month and six months of age. Pediatr Infect Dis J 2002;21:769--76.
Merck & Co., Inc. Recombivax
HB®: hepatitis B vaccine (recombinant) [Package insert]. Whitehouse Station, NJ: Merck & Co., Inc.; 1998.
Pichichero ME, Blatter MM, Reisinger KS, et al. Impact of a birth dose of hepatitis B vaccine on the reactogenicity and immunogenicity
of diphtheria-tetanus-acellular pertussis-hepatitis B-inactivated
poliovirus-Haemophilus influenzae type b combination vaccination. Pediatr Infect Dis
J 2002;21:854--9.
Yusuf HR, Daniels D, Smith P, Coronado V, Rodewald L. Association between administration of hepatitis B vaccine at birth and completion of
the hepatitis B and 4:3:1:3 vaccine series. JAMA 2000;284:978--83.
Lauderdale DS, Oram RJ, Goldstein KP, Daum RS. Hepatitis B vaccination among children in inner-city public housing, 1991--1997.
JAMA 1999;282:1725--30.
Marsano LS, West DJ, Chan I, et al. A two-dose hepatitis B vaccine regimen: proof of priming and memory responses in young adults.
Vaccine 1998;16:624--9.
Hadler SC, de Monzon MA, Lugo DR, Perez M. Effect of timing of hepatitis B vaccine doses on response to vaccine in Yucpa Indians.
Vaccine 1989;7:106--10.
Wistrom J, Ahlm C, Lundberg S, Settergren B, Tarnvik A. Booster vaccination with recombinant hepatitis B vaccine four years after priming
with one single dose. Vaccine 1999;17:2162--5.
Halsey NA, Moulton LH, O'Donovan JC, et al. Hepatitis B vaccine administered to children and adolescents at yearly intervals.
Pediatrics 1999;103:1243--7.
Jilg W, Schmidt M, Deinhardt F. Vaccination against hepatitis B: comparison of three different vaccination schedules. J Infect Dis
1989;160:766--9.
Seto D, West DJ, Gilliam RR, Ioli VA, Ferrara DK, Rich B. Antibody responses of healthy neonates of two mixed regimens of hepatitis B
vaccine. Pediatr Infect Dis J 1999;18:840--1.
Tan KL, Goh KT, Oon CJ, Chan SH. Immunogenicity of recombinant yeast-derived hepatitis B vaccine in nonresponders to
perinatal immunization. JAMA 1994;271:859--61.
Lau YL, Tam AY, Ng KW, et al. Response of preterm infants to hepatitis B vaccine. J Pediatr 1992;121:962--5.
Losonsky GA, Wasserman SS, Stephens I, et al. Hepatitis B vaccination of premature infants: a reassessment of current recommendations
for delayed immunization. Pediatrics 1999;103:E14--20.
Linder N, Vishne TH, Levin E, et al. Hepatitis B vaccination: long-term follow-up of the immune response of preterm infants and comparison
of two vaccination protocols. Infection 2002;30:136--9.
Huang FY, Lee PI, Lee CY, Huang LM, Chang LY, Liu SC. Hepatitis B vaccination in preterm infants. Arch Dis Child 1997;77:F135--8.
Kim SC, Chung EK, Hodinka RL, et al. Immunogenicity of hepatitis B vaccine in preterm infants. Pediatrics 1997;99:534--6.
Patel DM, Butler J, Feldman S, Graves GR, Rhodes PG. Immunogenicity of hepatitis B vaccine in healthy very low birth weight infants. J
Pediatr 1997;131:641--3.
Belloni C, Chirico G, Pistorio A, Orsolini P, Tinelli C, Rondini G. Immunogenicity of hepatitis B vaccine in term and preterm infants.
Acta Paediatr 1998;87:336--8.
Callis LM, Clanxet J, Fortuny G, Caballeria J, Carrasco JL, Lardinois R. Hepatitis B virus infection and vaccination in children
undergoing hemodialysis. Acta Paediatr Scand 1985;74:213--8.
Drachman R, Isacsohn M, Rudensky B, Drukker A. Vaccination against hepatitis B in children and adolescent patients on dialysis. Nephrol
Dial Transplant 1989;4:372--4.
Watkins SL, Alexander SR, Brewer ED, et al. Response to recombinant hepatitis B vaccine in children and adolescents with chronic renal
failure. Am J Kidney Dis 2002;40:365--72.
Vazquez G, Mendoza-Guevara L, Alvarez T, et al. Comparison of the response to the recombinant vaccine against hepatitis B virus in dialyzed
and nondialyzed children with CRF using different doses and routes of administration. Adv Perit Dial 1997;13:291--6.
Collier AC, Corey L, Murphy VL, Handsfield HH. Antibody to human immunodeficiency virus (HIV) and suboptimal response to hepatitis
B vaccination. Ann Intern Med 1988;109:101--5.
Zuin G, Principi N, Tornaghi R, et al. Impaired response to hepatitis B vaccine in HIV infected children. Vaccine 1992;10:857--60.
Hovi L, Valle M, Siimes MA, Jalanko H, Saarinen UM. Impaired response to hepatitis B vaccine in children receiving anticancer
chemotherapy. Pediatr Infect Dis J 1995;14:931--5.
Polychronopoulou-Androulakaki S, Panagiotou JP, Kostaridou S, Kyratzopoulou A, Haidas S. Immune response of
immuno-com-pro-mised children with malignancies to a recombinant hepatitis B vaccine. Pediatr Hematol Oncol 1996;13:425--31.
Wilson CM, Ellenberg JH, Sawyer MK, et al. Serologic response to hepatitis B vaccine in HIV infected and high-risk HIV uninfected
adolescents in the REACH cohort. Reaching for excellence in adolescent care and health. J Adolesc Health 2001;29(Suppl 3):123--9.
Rey D, Krantz V, Partisani M, et al. Increasing the number of hepatitis B vaccine injections augments anti-HBs response rate in
HIV-infected patients: effects on HIV-1 viral load. Vaccine 2000;18: 1161--5.
Choudhury SA, Peters VB. Responses to hepatitis B vaccine boosters in human immunodeficiency virus-infected children. Pediatr Infect Dis
J 1995;14:65--7.
Szmuness W, Stevens CE, Harley EJ, et al. Hepatitis B vaccine: demonstration of efficacy in a controlled clinical trial in a high-risk population
in the United States. N Engl J Med 1980;303:833--41.
Francis DP, Hadler SC, Thompson SE, et al. The prevention of hepatitis B with vaccine: report of the Centers for Disease Control
multi-center efficacy trial among homosexual men. Ann Intern Med 1982; 97:362--6.
Hadler SC, Francis DP, Maynard JE, et al. Long-term immunogenicity and efficacy of hepatitis B vaccine in homosexual men. N Engl J
Med 1986;315:209--14.
Jack AD, Hall AJ, Maine N, Mendy M, Whittle HC. What level of hepatitis B antibody is protective? J Infect Dis 1999;179:489--92.
Mintai Z, Kezhou L, Lieming D, Smego RA Jr. Duration and efficacy of immune response to hepatitis B vaccine in high-risk Chinese
adolescents. Clin Infect Dis 1993;16:165--7.
Resti M, Azzari C, Mannelli F, Rossi ME, Lionetti P, Vierucci A. Ten-year follow-up study of neonatal hepatitis B immunization: are
booster injections indicated? Vaccine 1997;15:1338--40.
Viviani S, Jack A, Hall AJ, et al. Hepatitis B vaccination in infancy in The Gambia: protection against carriage at 9 years of age.
Vaccine 1999;17:2946--50.
Huang LM, Chiang BL, Lee CY, Lee PI, Chi WK, Chang MH. Long-term response to hepatitis B vaccination and response to booster in
children born to mothers with hepatitis B e antigen. Hepatology 1999;29:954--9.
Mast E, Mahoney F, Kane M, Margolis H. Hepatitis B vaccines. In: Plotkin SA, Orenstein WA, eds. Vaccines. 4th ed. Orlando, FL: W.B.
Saunders Co.; 2003:299--337.
Banatvala JE, Van Damme P. Hepatitis B vaccine---do we need boosters? J Viral Hepat 2003;10:1--6.
Petersen KM, Bulkow LR, McMahon BJ, et al. Duration of hepatitis B immunity in low risk children receiving hepatitis B vaccinations from
birth. Pediatr Infect Dis J 2004;23:650--5.
Dentinger CM, McMahon BJ, Fiore AE, et al. Anti-HBs persistence and response to a hepatitis B (HB) vaccine boost among Yup'ik Eskimos
23 years after HB vaccination [Poster 1028]. Annual Meeting of the Infectious Diseases Society of America, San Francisco, California, October
6--9, 2005.
Hadler SC, Coleman PJ, O'Malley P, Judson FN, Altman N. Evaluation of long-term protection by hepatitis B vaccine for seven to nine years
in homosexual men. In: Hollinger FB, Lemon SM, Margolis H, eds. Viral hepatitis and liver disease. Baltimore, MD: Williams & Wilkins; 1991.
Stevens CE, Alter HJ, Taylor PE, Zang EA, Harley EJ, Szmuness W. Hepatitis B vaccine in patients receiving hemodialysis. Immunogenicity
and efficacy. N Engl J Med 1984;311:496--501.
Andre FE, Zuckerman AJ. Review: protective efficacy of hepatitis B vaccines in neonates. J Med Virol 1994;44:144--51.
Roumeliotou-Karayannis A, Papaevangelou G, Tassopoulos N, Richardson SC, Krugman S. Post-exposure active immunoprophylaxis of spouses
of acute viral hepatitis B patients. Vaccine 1985;3:31--4.
Papaevangelou G, Roumeliotou-Karayannis A, Richardson SC, Nikolakakis P, Kalafatas P. Postexposure immunoprophylaxis of spouses of
patients with acute viral hepatitis B. In: Zuckerman AJ, ed. Viral hepatitis and liver disease. New York,
NY:Alan R. Liss, Inc.; 1988:992--4.
Mitsui T, Iwano K, Suzuki S, et al. Combined hepatitis B immune globulin and vaccine for postexposure prophylaxis of accidental hepatitis B
virus infection in hemodialysis staff members: comparison with immune globulin without vaccine in historical controls. Hepatology 1989;10:324--7.
Grady GF, Lee VA, Prince AM, et al. Hepatitis B immune globulin for accidental exposures among medical personnel: final report of a
multicenter controlled trial. J Infect Dis 1978;138:625--38.
Seeff LB, Wright EC, Zimmerman HJ, et al. Type B hepatitis after needle-stick exposure: prevention with hepatitis B immune globulin.
Final report of the Veterans Administration Cooperative Study. Ann Intern Med 1978;88:285--93.
Redeker AG, Mosley JW, Gocke DJ, McKee AP, Pollack W. Hepatitis B immune globulin as a prophylactic measure for spouses exposed to
acute type B hepatitis. N Engl J Med 1975;293:1055--9.
Perrillo RP, Campbell CR, Strang S, Bodicky CJ, Costigan DJ. Immune globulin and hepatitis B immune globulin. Prophylactic measures
for intimate contacts exposed to acute type B hepatitis. Arch Intern Med 1984;144:81--5.
Grady GF. Viral hepatitis: passive prophylaxis with globulins---state of the art in 1978. In: Vyas GN, Cohen SN, Schmid R, eds. Viral hepatitis:
a contemporary assessment of etiology, epidemiology, pathogenesis, and prevention. Philadelphia, PA: Franklin Institute Press, 1978:467--76.
Beasley RP, Stevens CE. Vertical transmission of HBV and interruption with globulin. In: Vyas GN, Cohen SN, Schmid R, eds. Viral hepatitis:
a contemporary assessment of etiology, epidemiology, pathogenesis, and prevention. Philadelphia, PA: Franklin Institute Press; 1978:333--45.
Marion SA, Tomm PM, Pi DW, Mathias RG. Long-term follow-up of hepatitis B vaccine in infants of carrier mothers. Am J
Epidemiol 1994;140:734--46.
Beasley RP, Hwang LY, Lee GC, et al. Prevention of perinatally transmitted hepatitis B virus infections with hepatitis B virus infections
with hepatitis B immune globulin and hepatitis B vaccine. Lancet 1983;2(8359):1099--102.
Lo KJ, Tsai YT, Lee SD, et al. Immunoprophylaxis of infection with hepatitis B virus in infants born to hepatitis B surface antigen-positive
carrier mothers. J Infect Dis 1985;152:817--22.
Poovorawan Y, Sanpavat S, Pongpunlert W, et al. Comparison of a recombinant DNA hepatitis B vaccine alone or in combination with hepatitis
B immune globulin for the prevention of perinatal acquisition of hepatitis B carriage. Vaccine 1990 (Suppl 8):S56--9.
Assateerawatt A, Tanphaichitr VS, Suvatte V, In-ngarm L. Immunogenicity and protective efficacy of low dose recombinant DNA hepatitis
B vaccine in normal and high-risk neonates. Asian Pac J Allergy Immunol 1991;9:89--93.
Milne A, West DJ, Chinh DV, Moyes CD, Poerschke G. Field evaluation of the efficacy and immunogenicity of recombinant hepatitis B
vaccine without HBIG in newborn Vietnamese infants. J Med Virol 2002;67:327--33.
Hsu HM, Chen DS, Chuang CH, et al. Efficacy of a mass hepatitis B vaccination program in Taiwan: studies on 3464 infants of hepatitis B
surface antigen-carrier mothers. JAMA 1988;260:2231--5.
Al Faleh FZ, Al Jeffri M, Ramia S, et al. Seroepidemiology of hepatitis B virus infection in Saudi children 8 years after a mass hepatitis
B vaccination programme. J Infect 1999;38:167--70.
Harpaz R, McMahon BJ, Margolis HS, et al. Elimination of new chronic hepatitis B virus infections: results of the Alaska immunization
program. J Infect Dis 2000;181:413--8.
Zajac BA, West DJ, McAleer WJ, Scolnick EM. Overview of clinical studies with hepatitis B vaccine made by recombinant DNA. J
Infect 1986;13(Suppl A):39--45.
Andre FE. Summary of safety and efficacy data on a yeast-derived hepatitis B vaccine. Am J Med 1989;87:S14--20.
Lewis E, Shinefield HR, Woodruff BA, et al. Safety of neonatal hepatitis B vaccine administration. Pediatr Infect Dis J 2001;20: 1049--54.
Stratton KR, Howe CJ, Johnston RB Jr, eds. Adverse events associated with childhood vaccines: evidence bearing on causality. Washington,
DC: Institute of Medicine, National Academy Press; 1994.
Bohlke K, Davis RL, Marcy SM, et al. Risk of anaphylaxis after vaccination of children and adolescents. Pediatrics 2003;112:815--20.
Shaw FE Jr, Graham DJ, Guess HA, et al. Postmarketing surveillance for neurologic adverse events reported after hepatitis B vaccination: experience of
the first three years. Amer J Epidemiol 1988;127:337--51.
Hernan MA, Jick SS, Olek MJ, Jick H. Recombinant hepatitis B vaccine and the risk of multiple sclerosis: a prospective study.
Neurology 2004;63:838--42.
MacIntyre CR, Kelly H, Jolley D, et al. Recombinant hepatitis B vaccine and the risk of multiple sclerosis: a prospective study [Letter].
Neurology 2005;64:1317.
Ascherio A, Zhang SM, Hernan MA, et al. Hepatitis B vaccination and the risk of multiple sclerosis. N Engl J Med 2001;344:327--32.
Confavreux C, Suissa S, Saddier P, Bourdes V, Vukusic S. Vaccinations and the risk of relapse in multiple sclerosis. N Engl J Med
2001;344:319--26.
DeStefano F, Verstraeten T, Chen RT. Hepatitis B vaccine and risk of multiple sclerosis. Expert Rev Vaccines 2002;1:461--6.
DeStefano F, Verstraeten T, Jackson LA, et al. Vaccinations and risk of central nervous system demyelinating diseases in adults. Arch
Neurol 2003;60:504--9.
Halsey NA, Duclos P, Van Damme P, Margolis H. Hepatitis B vaccine and central nervous system demyelinating diseases. Pediatr Infect Dis
J 1999;18:23--4.
Stratton K, Almario DA, McCormick MC, eds. Hepatitis B vaccine and central nervous system demyelinating disorders. Washington,
DC: Institute of Medicine, National Academy Press; 2002.
Anonymous. Alleged link between hepatitis B vaccine and chronic fatigue syndrome. Can Dis Wkly Rep 1991;17:215--6.
Herroelen L, de Keyser J, Ebinger G. Central-nervous-system demyelination after immunisation with recombinant hepatitis B vaccine.
Lancet 1991;338(8776):1174--5.
Trevisani F, Gattinara GC, Caraceni P, et al. Transverse myelitis following hepatitis B vaccination. J Hepatol 1993;19:317--8.
Konstantinou D, Paschalis C, Maraziotis T, Dimopoulos P, Bassaris H, Skoutelis A. Two episodes of leukoencephalitis associated with
recombinant hepatitis B vaccination in a single patient. Clin Infect Dis 2001;33:1772--3.
Pope JE, Stevens A, Howson W, Bell DA. The development of rheumatoid arthritis after recombinant hepatitis B vaccination. J
Rheumatol 1998;25:1687--93.
Maillefert JF, Sibilia J, Toussirot E, et al. Rheumatic disorders developed after hepatitis B vaccination. Rheumatology (Oxford) 1999;38:978--83.
Classen JB. Childhood immunisation and diabetes mellitus. N Z Med J 1996;109(1022):195.
Tudela P, Marti S, Bonal J. Systemic lupus erythematosus and vaccination against hepatitis B. Nephron 1992;62:236.
Institute for Vaccine Safety Diabetes Workshop Panel. Childhood immunization and type I diabetes: summary of an Institute for Vaccine
Safety workshop. Pediatr Infec Dis J 1999;18:217--22.
DeStefano F, Mullooly JP, Okoro CA, et al. Childhood vaccinations, vaccination timing, and risk of type 1 diabetes mellitus.
Pediatrics 2001;108:E112--6.
DeStefano F, Gu D, Kramarz P, et al. Childhood vaccinations and risk of asthma. Pediatr Infect Dis J 2002;21:498--504.
Stratton K, Wilson CB, McCormick MC, eds. Immunization safety review: multiple immunizations and immune dysfunction. Washington,
DC: Institute of Medicine, National Academy Press; 2002.
Wise RP, Kiminyo KP, Salive ME. Hair loss after routine immunizations. JAMA 1997;278:1176--8.
Schwalbe JA , Ray P, Black SB, et al. Risk of alopecia after hepatitis B vaccination [Abstract]. Annual Interscience Conference on
Antimicrobial Agents and Chemotherapy. San Diego, California, September 24--27, 1998.
Mitchell EA, Stewart AW, Clements M. Immunisation and the sudden infant death syndrome. Arch Dis Child 1995;73:498--501.
Niu MT, Salive ME, Ellenberg SS. Neonatal deaths after hepatitis B vaccine: the Vaccine Adverse Event Reporting System, 1991--1998.
Arch Pediatr Adolesc Med 1999;153:1279--82.
Eriksen EM, Perlman JA, Miller A, et al. Lack of association between hepatitis B birth immunization and neonatal death: a population-based
study from the Vaccine Safety Datalink Project. Pediatr Infect Dis J 2004;23:656--62.
Silvers LE, Ellenberg SS, Wise RP, Varricchio FE, Mootrey GT, Salive ME. The epidemiology of fatalities reported to the Vaccine Adverse
Event Reporting System 1990--1997. Pharmacoepidemiol Drug Saf 2001;10:279--85.
Levy M, Koren G. Hepatitis B vaccine in pregnancy: maternal and fetal safety. Am J Perinatol 1991;8:227--32.
Zuckerman AJ. Effect of hepatitis B virus mutants on efficacy of vaccination. Lancet 2000;355:1382--4.
Hsu HY, Chang MH, Liaw SH, Li YH, Chen HL. Changes of hepatitis B surface antigen variants in carrier children before and after
universal vaccination in Taiwan. Hepatology 1999;30:1312--7.
Mele A, Tancredi F, Romano L, et al. Effectiveness of hepatitis B vaccination in babies born to hepatitis B surface antigen-positive mothers in
Italy. J Infect Dis 2001;184:905--8.
Glossary
Terms and Abbreviations Used in This Report
ACIP
Advisory Committee on Immunization Practices
ALT
alanine aminotransferase
Anti-HBc
antibody to hepatitis B core antigen
Anti-HBe
antibody to hepatitis B e antigen
Anti-HBs
antibody to hepatitis B surface antigen
DTaP
diphtheria and tetanus toxoids and acellular pertussis adsorbed
FDA
Food and Drug Administration
HBcAg
hepatitis B core antigen
HBeAg
hepatitis B e antigen
HBIG
hepatitis B immune globulin
HBsAg
hepatitis B surface antigen
HBV
hepatitis B virus
HCC
hepatocellular carcinoma
HCV
hepatitis C virus
Hib
Haemophilus influenzae type b
HIV
human immunodeficiency virus
IgM
immunoglobulin M
IPV
inactivated poliovirus
MS
multiple sclerosis
NHANES
National Health and Nutrition Examination Survey
VAERS
Vaccine Adverse Events Reporting System
VSD
Vaccine Safety Datalink
Advisory Committee on Immunization Practices
Membership List, June 2005
Chairman: Myron J. Levin, MD, Professor of Pediatrics and Medicine, University of Colorado Health Sciences Center, Denver, Colorado.
Executive Secretary: Larry Pickering, MD, National Immunization Program, CDC, Atlanta, Georgia.
Members: Jon S. Abramson, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina; Ban Mishu Allos, MD,
Vanderbilt University School of Medicine, Nashville, Tennessee; Guthrie S. Birkhead, MD, New York State Department of Health, Albany, New York;
Judith Campbell, MD, Baylor College of Medicine, Houston, Texas; Reginald Finger, MD, Focus on the Family, Colorado Springs, Colorado; Janet
Gildsdorf, MD, University of Michigan, Ann Arbor, Michigan; Tracy Lieu, MD, Harvard Pilgrim Health Care and Harvard Medical School,
Boston, Massachusetts; Edgar Marcuse, MD, Children's Hospital and Regional Medical Center, Seattle, Washington; Julia Morita, MD, Chicago Department
of Health, Chicago, Illinois; Gregory Poland, MD, Mayo Clinic College of Medicine, Rochester, Minnesota; John B. Salamone, National Italian
American Foundation, Washington, DC; Patricia Stinchfield, Children's Hospital and Clinics, St. Paul, Minnesota; John J. Treanor, MD, University of
Rochester School of Medicine and Dentistry, Rochester, New York; Robin Womeodu, MD, University of Tennessee Health Sciences Center, Memphis, Tennessee.
Ex-Officio Members: James E. Cheek, MD, Indian Health Service, Albuquerque, New Mexico; Wayne Hachey, DO, Department of Defense,
Falls Church, Virginia; Geoffrey S. Evans, MD, Health Resources and Services Administration, Rockville, Maryland; Bruce Gellin, MD, National
Vaccine Program Office, Washington, DC; Linda Murphy, Centers for Medicare and Medicaid Services, Baltimore, Maryland; George T. Curlin, MD,
National Institutes of Health, Bethesda, Maryland; Norman Baylor, MD, Food and Drug Administration, Bethesda, Maryland; Kristin Lee Nichol,
MD, Department of Veterans Affairs, Minneapolis, Minnesota.
Liaison Representatives: American Academy of Family Physicians, Jonathan Temte, MD, Clarence, New York, and Richard Clover, MD,
Louisville, Kentucky; American Academy of Pediatrics, Margaret Rennels, MD, Baltimore, Maryland, and Carol Baker, MD, Houston, Texas; America's
Health Insurance Plans, Andrea Gelzer, MD, Hartford, Connecticut; American College Health Association, James C. Turner, MD, Charlottesville,
Virginia; American College of Obstetricians and Gynecologists, Stanley Gall, MD, Louisville, Kentucky; American College of Physicians, Kathleen Neuzil,
MD, Seattle, Washington; American Medical Association, Litjen Tan, PhD, Chicago, Illinois; American Pharmacists Association, Stephan L. Foster,
PharmD, Memphis, Tennessee; Association of Teachers of Preventive Medicine, W. Paul McKinney, MD, Louisville, Kentucky; Biotechnology
Industry Organization, Clement Lewin, PhD, Cambridge, Massachusetts; Canadian National Advisory Committee on Immunization, Monica Naus,
MD, Vancouver, British Columbia; Health-Care Infection Control Practices Advisory Committee, Steve Gordon, MD, Cleveland, Ohio; Infectious
Diseases Society of America, Samuel L. Katz, MD, Durham, North Carolina, and William Schaffner, MD, Nashville, Tennessee; London Department of
Health, David M. Salisbury, MD, London, United Kingdom; National Association of County and City Health Officials, Nancy Bennett, MD, Rochester,
New York; National Coalition for Adult Immunization, David A. Neumann, PhD, Bethesda, Maryland; National Immunization Council and Child
Health Program, Mexico, Romeo Rodriguez, Mexico City, Mexico; National Medical Association, Dennis A. Brooks, MD, Baltimore, Maryland;
National Vaccine Advisory Committee, Charles Helms, MD, PhD, Iowa City, Iowa; Pharmaceutical Research and Manufacturers of America, Damian A.
Braga, Swiftwater, Pennsylvania, and Peter Paradiso, PhD, Collegeville, Pennsylvania; and Society for Adolescent Medicine, Amy Middleman, MD,
Houston, Texas.
ACIP Hepatitis Vaccines Working Group
Chair: Tracy Lieu, MD, Boston, Massachusetts.
Members: Jon Abramson, MD, Winston-Salem, North Carolina; Beth Bell, MD, Atlanta, Georgia; James E. Cheek, MD, Albuquerque, New
Mexico; Anthony Fiore, MD, Atlanta, Georgia; Stephen Feinstone, MD, Bethesda, Maryland; Robert Frenck, MD, Torrance, California; Stanley Gall,
MD, Louisville, Kentucky; Janet Gildsdorf, MD, Ann Arbor, Michigan; Steve Gordon, MD, Cleveland, Ohio; Samuel L. Katz, MD, Durham,
North Carolina; Edgar Marcuse, MD, Seattle, Washington; Ban Mishu Allos, MD, Nashville, Tennessee; Eric Mast, MD, Atlanta, Georgia; Julia Morita,
MD, Chicago, Illinois; William Schaffner, MD, Nashville, Tennessee; Deborah Wexler, MD,
St. Paul, Minnesota.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].