 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Human Immunodeficiency Virus (HIV) Risk, Prevention, and Testing Behaviors --- United States, National HIV Behavioral Surveillance System: Men Who Have Sex with Men, November 2003--April 2005Please note: An erratum has been published for this article. To view the erratum, please click here. Travis Sanchez, DVM1
Corresponding author: Travis Sanchez, DVM, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), 1600 Clifton Road, NE, MS E-46, Atlanta, GA 30333. Telephone: 404-639-1742; Fax: 404-639-8640; E-mail: [email protected]. AbstractProblem/Condition: For CDC's goal of reducing the number of new human immunodeficiency virus (HIV) infections to be achieved, data are needed to assess the prevalence of HIV-related risk behaviors at a given time, monitor trends in these behaviors, and assess the correlates of risk. These data also can be used to evaluate the extent to which current HIV-prevention programs are reaching targeted communities and direct future HIV-prevention activities to reduce HIV transmission. Reporting period: November 2003--April 2005. Description of system: The National HIV Behavioral Surveillance (NHBS) System collects risk behavior data from three populations at high risk for HIV infection: men who have sex with men (MSM), injection-drug users, and heterosexual adults in areas in which HIV is prevalent. Data collection began in 2003 among MSM in 17 U.S. metropolitan statistical areas (MSAs), and surveys have been conducted in 25 MSAs since 2005. Participants must be aged >18 years and reside in a participating MSA. Results: This report summarizes data gathered during the first cycle (i.e., data collection period) of NHBS (November 2003--April 2005) from approximately 10,000 MSM. The results indicated that >90% of participants had ever been tested for HIV. Of those, 77% had been tested during the preceding 12 months. In addition to their male sex partners, 14% of participants also had at least one female sex partner during the preceding 12 months. Unprotected anal intercourse was reported by 58% with a main male partner (someone with whom the participant had sex and to whom he felt most committed [e.g., a boyfriend, spouse, significant other, or life partner]) and by 34% with a casual male partner (someone with whom the participant had sex but who was not considered a main partner). Noninjection drugs were used by 42% of participants during the preceding 12 months; the most commonly used drugs were marijuana (77%), cocaine (37%), ecstasy (29%), poppers (28%), and stimulants (27%). A substantial proportion (80%) of participants had received free condoms during the preceding 12 months, but fewer had participated in individual- or group-level HIV prevention programs (15% and 8%, respectively). Interpretation: MSM surveyed engaged in sexual and drug-use behaviors that placed them at increased risk for HIV infection. The majority of MSM surveyed had been tested for HIV infection. Although a substantial proportion of participants had received free condoms, a much smaller proportion had participated in more intensive HIV-prevention programs. Public Health Action: NHBS data are used to assess and develop effective HIV-prevention programs and services. Continued collection and reporting of NHBS data from all targeted high-risk populations is needed to monitor behavior trends and assess future HIV prevention needs in these populations. The data are used for local HIV-prevention planning and monitoring in MSAs in which NHBS is conducted. IntroductionAt the end of 2004, approximately 500,000 persons were living with human immunodeficiency virus (HIV) or acquired immunodeficiency syndrome (AIDS) in the 35 U.S. areas with confidential name-based HIV infection reporting since 2000 (1). Certain behaviors (e.g., unprotected sexual intercourse and injection-drug use) are associated with high risk for HIV transmission. Through 2004, of all cases of HIV infection in the United States reported to CDC, 34% were attributed to male-male sexual contact, 14% to injection-drug use, and 20% to heterosexual contact (1). HIV testing is a cornerstone of HIV prevention in the United States (2). Persons who learn their HIV status might reduce risk behaviors and can be referred to appropriate care and treatment services. In addition to testing, other prevention activities in the United States are focused on behavior-change strategies and the provision of prevention information and materials (e.g., condoms). In 2002, CDC developed the National HIV Behavioral Surveillance (NHBS) System to help state and local health departments monitor selected behaviors and assess the use of prevention programs and services in groups at highest risk for HIV infection. Findings from NHBS enhance understanding of HIV risk and testing behaviors and can be used to develop and evaluate the use of HIV-prevention programs in these communities. This report summarizes results from the first NHBS cycle (i.e., data collection period), which was conducted during November 2003--April 2005 among men who have sex with men (MSM). This report provides descriptive data that serve as a baseline to monitor trends in behavior prevalence and that aid in assessing the scope of the problem and in identifying potential opportunities for HIV prevention in this population. MethodsOverviewThe overall strategy for NHBS involves conducting rotating cycles of surveillance in three populations at high risk for HIV: MSM (NHBS-MSM), injection-drug users (NHBS-IDU), and heterosexual adults in high-prevalence areas (NHBS-HET). The same basic eligibility criteria are used in all MSAs: being aged >18 years, a current resident of an MSA, not a previous participant in NHBS during the current cycle, and able to provide informed consent. For each survey cycle, a standardized questionnaire is used to collect information about behavioral risks for HIV, HIV testing history, and use of HIV-prevention services and programs. The face-to-face survey is administered by a trained interviewer using a handheld computer. A minimum of 500 eligible persons from each MSA are interviewed during each cycle. CDC has determined that NHBS is public health surveillance and is not classified as a research activity; all state and local jurisdictions are responsible for performing their own local human subjects protections review. Participating MSAsState and local health departments that were eligible to participate in NHBS were those whose jurisdictions included MSAs with the highest estimated prevalence of persons living with AIDS (Figure 1). Interviews were conducted in 17 eligible MSAs during the first cycle of NHBS-MSM: Atlanta, Georgia; Baltimore, Maryland; Boston, Massachusetts; Chicago, Illinois; Dallas, Texas; Denver, Colorado; Fort Lauderdale, Florida; Houston, Texas; Los Angeles, California; Miami, Florida; Newark, New Jersey; New York City, New York; Philadelphia, Pennsylvania; San Diego, California; San Francisco, California; San Juan, Puerto Rico; and Washington, District of Columbia. In the subsequent NHBS cycle (NHBS-IDU), data collection began in the following eight MSAs: Detroit, Michigan; Las Vegas, Nevada; Nassau-Suffolk, New York; New Haven, Connecticut; New Orleans, Louisiana; Norfolk, Virginia; Seattle, Washington; and St. Louis, Missouri. NHBS-MSM Sampling MethodInterviews for NHBS-MSM were obtained using time-space sampling methods (3). Details about the NHBS-MSM method will be described subsequently (4); the main steps are as follows:
Men who accepted the invitation to participate were escorted to a private area for the interview. Interviewers obtained informed consent and conducted face-to-face interviews with all participants. Each interview averaged 20 minutes and consisted of questions concerning participants' demographic characteristics, HIV testing history, sexual and drug-use behaviors, hepatitis vaccination, sexually transmitted disease (STD) diagnosis and testing, and use of HIV prevention services and programs. In exchange for their time in taking part in the interview, participants received $25 in cash or a gift certificate. HIV testing was conducted only in those NHBS MSAs that had participated in an earlier study of MSM (5). These HIV testing data have been published previously (6). Data AnalysisParticipantsThis surveillance summary presents the results of a descriptive analysis (no statistical tests were performed) of key behavioral surveillance indicators for MSM from the following MSAs that collected and submitted requested data during the NHBS-MSM cycle: Atlanta, Georgia; Baltimore, Maryland; Boston, Massachusetts; Chicago, Illinois; Denver, Colorado; Fort Lauderdale, Florida; Houston, Texas; Los Angeles, California; Miami, Florida; New York, New York; Newark, New Jersey; Philadelphia, Pennsylvania; San Diego, California; San Francisco, California; and San Juan, Puerto Rico. In addition to the overall eligibility criteria, three criteria were applied for inclusion in this report on MSM. During the interview, participants must have reported 1) being male, 2) having had at least one male sex partner during the 12 months preceding the interview, and 3) not being infected with HIV. Persons aware of their HIV infection were excluded from the report because the purpose of NHBS is to collect and report data on the behaviors of persons at risk for acquiring HIV infection, not the risk behaviors of those who know they are infected with HIV. The data were analyzed according to five demographic characteristics of participants: race/ethnicity, age group, education level, sexual identity, and MSA. The race/ethnicity categories were non-Hispanic white, non-Hispanic black, Hispanic, Asian or Pacific Islander, American Indian or Alaska Native, multiracial, and other. Age was grouped into five categories: ages 18--24 years, 25--34 years, 35--44 years, 45--54 years, and >55 years. Participants' education level was categorized as less than high school diploma, high school diploma or equivalent, and more than high school (i.e., at least some college or technical school education). Self-reported sexual identity was categorized as homosexual, bisexual, heterosexual, or other. HIV testing history, hepatitis vaccination, STD testing, and use of prevention services are presented by the type of health insurance the participant reported at the time of the interview. Health insurance was categorized as private (including membership in a health maintenance organization), public (e.g., Medicare or Medicaid), or none. BehaviorsThree time frames for self-reported behaviors were provided: ever (at any point in the participant's lifetime), during the preceding 12 months (during the 12 months preceding the date of the interview), and most recent (the most recent time the participant engaged in the behavior). HIV Testing Because knowledge of one's current HIV status through testing is a key goal of HIV prevention, data on HIV testing (ever and during the preceding 12 months) are presented. The facility administering the most recent HIV test and the reasons for not being tested for HIV also are presented. Participants selected reasons from a list and then were asked which reason was the main reason for not being tested during the preceding 12 months. Sexual Behavior Details about anal sex with male partners (preceding 12 months and most recent) are presented as high-risk behaviors for HIV transmission among MSM. Male sex partners were further defined as either main or casual partners. A main sex partner was someone with whom the participant had sex and to whom he felt most committed (e.g., a boyfriend, spouse, significant other, or life partner). A casual sex partner was someone with whom the participant had sex but who was not considered a main partner. Insertive anal sex was defined as a male participant placing his penis in the anus of his partner. Receptive anal sex was defined as a male partner placing his penis in a participant's anus. HIV serostatus of the sex partner was reported by all participants. For participants who reported that their most recent HIV test result was negative, the HIV serostatus of the most recent male sex partners is presented in the context of the type of anal sex behavior (condom use or insertive or receptive activity) during their most recent sexual encounter. For participants who reported both male and female sex partners, sexual behaviors during the preceding 12 months with partners of both sexes are presented. Drug Use Drug use can either lead directly to HIV transmission (injection-drug use) or facilitate sexual risk taking (any drug use). The use during the preceding 12 months of drugs that were not injected (noninjection drugs) and that were not prescribed for the participant is reported as the use of any type of drug, specific type of drug used, and whether the participant was under the influence of the drug during sex. Participants could report the use of multiple types of drugs during the preceding 12 months. Ever having participated in a drug and alcohol treatment program is reported for injection and noninjection-drug users. Hepatitis Vaccination and STD Testing Public health recommendations for sexually active MSM include vaccination for viral hepatitis and annual screening for STDs (7). Hepatitis vaccination was defined as having ever received a hepatitis vaccine (even 1 dose of hepatitis A vaccine, hepatitis B vaccine, or both). STD testing was defined as having a test for syphilis, gonorrhea, or some other STD during the preceding 12 months. Use of HIV Prevention Services and Programs Understanding the current use of HIV-prevention services and programs can assist in evaluating whether prevention activities are reaching the intended populations and can identify potential opportunities for additional services or programs. Data on the use of three HIV-prevention activities during the preceding 12 months are presented: receipt of free condoms, participation in an individual-level intervention, and participation in a group-level intervention. Free condoms might have been received at any location and need not have been provided as a specific part of a concerted HIV-prevention activity (e.g., provided for general STD prevention or for pregnancy prevention). Individual-level interventions were defined as one-on-one conversations with an outreach worker, counselor, or prevention worker concerning how to protect oneself against HIV and other STDs. Conversations that took place solely as a part of obtaining HIV testing (pretest and posttest counseling) were excluded. Group-level interventions were defined as small-group discussions about ways to protect oneself against HIV and other STDs. Definitions for both intervention levels were based on the intervention types in CDC's evaluation system (8). The type of provider of the prevention activity also is presented. ResultsDuring November 2003--April 2005, local staff approached 23,861 persons; brief eligibility interviews were completed with 19,488 (82%) persons, 17,322 (89%) of whom were eligible for an interview. Those not eligible were previous participants (407), persons aged <18 years (93), or persons not currently residing in the MSA (1,666). Of 17,322 persons determined to be eligible, 14,049 (81%) agreed to participate, 13,670 (97%) of whom completed an interview (response rate: 79%.) For purposes of this report, 3,640 interviews were excluded from participants who did not report having sex with another man during the 12 months before the interview, did not report being male, or reported being infected with HIV. This report includes data from 10,030 interviews. Characteristics of ParticipantsParticipants were of diverse racial and ethnic backgrounds and age groups but were most commonly non-Hispanic whites aged 25--44 years; 78% reported at least some college or technical school education (Table 1). Nearly all (98%) participants reported being homosexual or bisexual. The majority (66%) reported having private health insurance, but a substantial proportion (25%) had no health insurance. Although all venues on the sampling frame had an equal probability of being selected for sampling events, the majority of venues on the NHBS frame were bars, dance clubs or streets; 67% of participants were recruited in those venues. HIV TestingOf 9,249 (92%) participants who reported ever having an HIV test, 8,967 (97%) participants had received the results of their most recent HIV test, and 7,057 (77%) had been tested during the preceding 12 months (Table 2). HIV testing rates were high for all races and ethnicities and education levels. The primary venues in which HIV tests were administered included offices of private physicians (36%), public health clinics and community health centers (26%), and HIV counseling and testing programs (12%) (Table 3). A total of 2,973 (30%) participants had not been tested during the preceding 12 months. The most common reason for not having an HIV test was that the participant believed he had not done anything to acquire HIV. Other frequently reported reasons were fear of testing positive and lack of time for testing. Although structural barriers (e.g., lack of transportation, money, or insurance; not knowing where to get tested) and concerns about the confidentiality of HIV testing were commonly identified as one reason for not getting an HIV test, they were infrequently specified as the main reason for not being tested (Table 4). Sexual BehaviorType of Partner Of 10,030 participants, 7,628 (76%) reported having more than one male sex partner during the preceding 12 months. A total of 7,547 (75%) reported having a casual male sex partner (median: four; range: one to 300), 6,856 (68%) reported a main male sex partner (median: one; range: one to 100), and 4,373 (43%) reported having both types of partners during the preceding 12 months. Sexual Behavior with Male Partners A total of 4,699 (47%) participants reported having unprotected anal sex with a male partner during the preceding 12 months. The prevalence of anal sex with main male partners was highest for younger participants (Table 5). Anal sex was reported by a larger proportion of the men who identified themselves as homosexual or bisexual. Unprotected anal sex, however, was reported by similar proportions of men in all categories of sexual identity. Unprotected anal sex was more commonly reported with main male partners than with casual male partners. Although rates of anal sex and unprotected anal sex were similar for participants of all races and ethnicities, the rate of unprotected anal sex was highest for non-Hispanic white participants with their main male sex partners. Unprotected anal sex with casual male partners was least common among those with some college or technical school education. Of 8,947 HIV-negative participants, 4,165 (47%) did not know the serostatus of their most recent casual male partner, and 1,237 (14%) did not know that of their most recent main male partner (Figure 2). Of the 4,635 who did not know the serostatus of their male sex partner (either casual or main), 990 (21%) reported having unprotected anal sex during the most recent sexual encounter with that partner. The prevalence of anal sex and unprotected anal sex during the most recent sexual encounter was highest with main male partners (Table 6). More participants reported insertive anal sex than receptive anal sex, regardless of the partner's serostatus. Unprotected sex with HIV-positive main partners was generally less common than with HIV-negative partners. Although the total numbers were small, the highest prevalence of unprotected sex with an HIV-positive partner was during insertive anal sex with a casual partner. Sexual Behavior with Male and Female Partners Of 10,030 participants who reported having sex with men during the preceding 12 months, 1,450 (14%) reported having also engaged in anal, vaginal, or oral sex with a female partner during the preceding 12 months; of these, 209 (14%) had engaged only in oral sex with their male partners, and 120 (8%) had engaged only in oral sex with their female partners. Of participants who had vaginal or anal sex with both male and female partners, the highest prevalence of unprotected intercourse was with female partners (53%) (Table 7). However, this was not true of the participants who identified themselves as homosexual: more of them reported unprotected sex with their male partners. Drug UseNoninjection-Drug Use A total of 4,322 (43%) participants reported using a noninjection drug during the preceding 12 months; the prevalence of noninjection-drug use among participants did not differ by race or ethnicity or by education (Table 8). Among 4,322 participants who reported noninjection-drug use, the highest proportion (77%) used marijuana, followed by cocaine (37%), ecstasy (29%), poppers (amyl nitrate) (28%), and stimulants (27%) (Table 9). A total of 3,198 (74%) noninjection-drug users reported being under the influence of a drug during sex during the preceding 12 months; of 1,226 participants who reported using poppers, 1,097 (89%) reported being under the influence of poppers during sex. Other drugs commonly reported in conjunction with sex included marijuana, stimulants, noninjection cocaine and crack, and club drugs (e.g., ecstasy, gamma hydroxybutyrate [GHB], and ketamine). Of those who used a noninjection drug during the preceding 12 months, 670 (16%) had ever participated in a drug or alcohol treatment program. Injection-Drug Use A total of 566 (6%) participants reported having ever injected drugs for nonmedical purposes, and 194 (2%) had injected drugs during the preceding 12 months. Of these 194 participants, 52 (27%) had shared needles, syringes, or other drug-injection or preparation equipment during the preceding 12 months, and 101 (52%) had ever participated in a drug or alcohol treatment program. Hepatitis Vaccination and STD TestingHepatitis Vaccination Of the 10,030 participants, 5,333 (53%) reported that they had ever received >1 dose of hepatitis vaccine. Non-Hispanic black men (44%) and men who identified themselves as heterosexual (41%) reported the lowest rates of hepatitis vaccination (Table 10). Participants aged >55 years and those who were less educated were less likely to report hepatitis vaccination. The prevalence of hepatitis vaccination was lowest for those who had no health insurance (43%) or only public health insurance (45%) (Table 10). STD Testing Overall, 4,266 (43%) participants reported having been tested for syphilis, gonorrhea, or another STD during the preceding 12 months. STD testing was least common among non-Hispanic white and Asian/Pacific Islander participants (Table 10). Participants aged >35 years were less commonly tested than those aged <35 years. The rates of STD testing during the preceding 12 months were lowest for heterosexual participants and participants who had no health insurance. Use of HIV Prevention Services and ProgramsA total of 8,202 (82%) men reported participation in some type of HIV-prevention service or program during the preceding 12 months. Of these, 8,035 (98%) participants had received free condoms; 1,505 (15%) had engaged in an individual-level intervention, and 801 (8%) had engaged in a group-level intervention (Table 11). Non-Hispanic black or young (aged 18--24 years) men and those who had public health insurance were more likely to have participated in an individual- or group-level intervention. HIV/AIDS-focused community-based organizations were the most common providers of all types of HIV-prevention activities. Nearly one third of the men interviewed had received free condoms from other types of community venues (e.g., bars, clubs, bathhouses, Gay Pride events, restaurants, cafes, fitness clubs, and retail stores) (Table 12). DiscussionHIV TestingKnowledge of one's HIV serostatus (through HIV testing) has been key to preventing HIV transmission in the United States (2,9--12). Sexually active MSM should be tested at least annually for HIV (7). To increase the likelihood that persons at risk for infection are tested and receive their test results, CDC introduced the Advancing HIV Prevention Initiative in 2003 and has made rapid HIV tests available to health departments and community-based organizations for use in local HIV prevention programs (2). Key strategies for this initiative include using new testing technologies (e.g., rapid HIV testing) and integrating testing into medical care to ensure that persons are aware of their HIV serostatus and that infected persons obtain appropriate medical care and prevention services. The findings in this report concur with those from previous investigations that indicated that the majority of MSM had been tested for HIV and that a substantial proportion had been tested during the preceding 12 months (5,13). The prevalence of HIV testing (ever and during the preceding 12 months) is relatively consistent among groups of MSM. Given the reasons provided for not being tested for HIV during the preceding 12 months, certain MSM might benefit from efforts to increase their perception of personal risk and reduce structural barriers to annual HIV testing. The monitoring of HIV testing patterns will continue to be an important use of NHBS data. Sexual BehaviorMSM continue to be the largest population living with HIV in the United States (1). For the majority of MSM, unsafe sex with male partners is the most likely route of transmission of HIV infection (5,14,15). The sexual behavior that carries the highest risk for HIV transmission between MSM is unprotected anal sex between an infected partner and a partner who is not infected (16--18). Approximately 11% of HIV-negative participants reported having unprotected anal sex with a partner whose HIV status was unknown. According to another report of NHBS data, up to two thirds of non-Hispanic black MSM who reported during the interview that they were HIV-negative were, when tested, identified as being infected with HIV (6). The sexual transmission of HIV infection among MSM can be reduced by adopting effective protective behaviors: disclosure of accurate HIV serostatus between sex partners, reduction of the number of sex partners or mutual monogamy, and consistent and correct condom usage (2,9,19,20). NHBS data concerning sexual behavior can be used to monitor the effect of HIV-prevention initiatives on reducing the sexual transmission of HIV infection among MSM (19). Drug UseDrug use is associated with sexual risk behaviors among MSM (21), particularly unprotected anal sex (22--25). As a result of the changing patterns of drug use and the contexts in which it takes place, accurately assessing how substance abuse contributes to HIV transmission among MSM is complicated (26). Among NHBS participants, the prevalence of noninjection-drug use was high (43%), three quarters of noninjection drugs users reported being under the influence of these drugs during sex. Few participants who reported noninjection-drug use had ever participated in a drug treatment program. Treatment programs aimed at MSM, especially services that underscore HIV prevention, should address the use of drugs that are popular in this population (27--30). HIV-prevention programs should focus on decreasing drug use and reducing the high-risk sexual behaviors of MSM (31). NHBS data can be used to monitor emerging drug use trends among MSM and can inform the development or modification of HIV-prevention interventions for MSM who use drugs. Hepatitis Vaccination and STD TestingPublic health recommendations to prevent the spread of viral hepatitis through preexposure vaccination were first issued in 1982. Children, adolescents, and persons at increased risk for infection (e.g., MSM, injection-drug users, and health-care workers) should receive vaccine (7,32--34). Following these recommendations should increase the likelihood that sexually active MSM are vaccinated for hepatitis, but approximately half of NHBS participants reported never having received a hepatitis vaccination. Rates were even lower for non-Hispanic black MSM and those without private health insurance, underscoring the need for additional efforts with these groups. To prevent STDs among sexually active MSM, CDC recommends annual testing for syphilis, gonorrhea, and chlamydia (7). Fewer than half of the participants in this study reported having been tested for an STD during the preceding 12 months, and rates were even lower for sexually active older MSM and those with no health insurance. NHBS provides data for the ongoing monitoring of implementation of these prevention recommendations for MSM. Use of HIV-Prevention Services and ProgramsConsistent and correct use of condoms during sexual intercourse is effective in preventing sexually acquired HIV infection (35,36), and access to, and consistent use of, condoms continues to be an important HIV-prevention tool for sexually active persons (20,37,38). A substantial proportion of participants had received free condoms from multiple sources during the preceding 12 months. In 2001, CDC and its national partners introduced a strategic plan to reduce by 50% the number of new HIV infections (19). The plan called for increasing the proportion of MSM who consistently engage in behaviors that reduce their risk for acquiring HIV and urged that prevention efforts be focused on especially vulnerable MSM: young men and men who are members of racial or ethnic minority populations. HIV-prevention programs whose effectiveness has been demonstrated are the focus of these efforts, and they include individual- and group-level interventions (39). Although only a small proportion of men reported participation in an individual- or a group-level intervention, the largest proportions of men who had participated in these types of programs were young or members of racial/ethnic minority populations; these data suggest that these effective prevention programs are reaching the intended audience. As HIV-prevention activities for MSM continue to be developed and implemented, NHBS will be able to provide updated data regarding the delivery of these services and programs to the populations who most need them. LimitationsThe findings in this report are subject to at least six limitations. First, because a single standard for obtaining a representative sample of MSM that encompasses the diversity of the population has not been established, the external validity of the NHBS sample cannot be determined accurately (40). Second, findings from the MSAs in this study might not be generalizable to all other U.S. states or cities. Third, because the survey was administered by an interviewer, certain participants might not have accurately reported their behavior. For example, participants might have underreported a socially undesirable behavior that they were practicing (e.g., drug use) or might have overreported a socially desirable behavior that they were not practicing (e.g., using a condom during anal sex). Fourth, self-reported HIV serostatus and perceived knowledge of a partner's serostatus should be interpreted conservatively because this information might be inaccurate, especially in groups for which high rates of unrecognized HIV infection have been reported (6). Fifth, in certain instances, stratification by demographic characteristics might produce numbers that are too small for reliable interpretation. Because statistical tests were not performed, data should be interpreted with caution. Future statistical analyses of NHBS data are planned. Finally, although every attempt was made to develop, implement, and monitor a standard data collection protocol for this first year of NHBS, variations in the timing of data collection and the relative ease or difficulty of recruiting eligible men led to a wide range of MSA sample sizes. ConclusionFor CDC's HIV-prevention strategic plan goal of reducing the number of new HIV infections to be achieved (19), a multifaceted approach is required that includes prevention programs designed to reduce risk behaviors and increase knowledge of HIV serostatus, especially among populations at high risk for HIV infection. To monitor progress toward achieving the objective and evaluate prevention programs, key behavior indicators must be collected from the same populations over time. NHBS was designed to collect these key indicators from the groups at high risk for acquiring HIV infection. This report has described the prevalence of multiple indicators that are relevant to HIV risk and prevention among MSM and has provided additional detail about MSM of differing backgrounds. A better understanding of the behaviors and circumstances that are associated with HIV transmission can improve the ability to develop appropriate prevention responses. Of particular importance is the high proportion of participants of all races and ethnicities who reported engaging in unprotected anal sex. Although >90% of participants had been tested for HIV, and three quarters of participants had been tested recently, MSM should share their HIV test results with all their sex partners more consistently. Noninjection-drug use can amplify sexual risk-taking behavior, and the use of noninjection drugs in combination with sex is prevalent among participants. The combination of drug use and unprotected sex with partners of unknown HIV serostatus should be studied more fully to better explain how it contributes to sustained risk behavior and continued HIV transmission among MSM. NHBS is a key component of CDC's comprehensive approach to reducing the spread of HIV in the United States and will be the primary source of data for monitoring behaviors of populations at high risk for HIV infection. The data will be used to assess the local and national prevalence of HIV-related risk behaviors, monitor behavior trends, and identify the demographic and behavioral correlates of risk. NHBS data also will be used to assess current local HIV prevention programs and directing future prevention activities to reduce HIV transmission. Acknowledgments The National HIV Behavioral Surveillance (NHBS) System was developed with the assistance of Ida M. Onorato, MD, Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), CDC. The following members of the NHBS system working group developed the protocol and questionnaire for the NHBS-MSM survey: Luke Shouse, MD, Division of Public Health, Georgia Department of Human Resources, David Holtgrave, PhD, Ben Hadsock, Rollins School of Public Health, Emory University, Atlanta, Georgia; Liza Solomon, DrPH, Colin Flynn, ScM, Maryland Department of Health and Mental Hygiene, Frangiscos Sifakis, PhD, Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland; Abbie Averbach, MPH, Jennifer Coyle, MPH, Massachusetts Department of Public Health, Chris Smith, MA, Abt Associates Inc., Boston, Massachusetts; Carol Ciesielski, MD, Nik Prachand, MPH, Chicago Department of Health, Chicago, Illinois; Sharon Melville, MD, Richard Yeager, PhD, Texas Department of State Health Services, Austin, Texas; Anne Freeman, MSPH, Douglas Shehan, Douglas Kershaw, University of Texas Southwestern Medical Center, Dallas, Texas; Mark Thrun, MD, Julie Subiadur, Denver Public Health Department, Denver, Colorado; Marcia Wolverton, MPH, Hafeez Rehman, MD, City of Houston Department of Health, Jan Risser, PhD, Bernardo Useche, PhD, University of Texas at Houston School of Public Health, Houston, Texas; Trista Bingham, MPH, Denise Johnson, MPH, Nina Harawa, PhD, County of Los Angeles Department of Health Services, Los Angeles, California; Marlene LaLota, MPH, Florida Department of Health, Tallahassee, Florida; Lisa Metsch, MD, David Forrest, PhD, University of Miami School of Medicine, Miami and Fort Lauderdale, Florida; Chris Murrill, PhD, New York City Department of Health, Beryl Koblin, PhD, Michael Camacho, New York Blood Center, New York City, New York; Helene Cross, PhD, Barbara Bolden, PhD, Sally D'Errico, MEd, New Jersey Department of Health and Senior Services, Trenton, New Jersey; Henry Godette, North Jersey Community Research Initiative, Newark, New Jersey; Kathleen Brady, MD, Philadelphia Department of Public Health, Philadelphia, Pennsylvania; Assunta Ritieni, MHS, California Department of Health Services, Sacramento, California; Al Valesco, PhD, Velasco Consulting, Leticia Cazares, San Ysidro Health Center, San Diego, California; Willi McFarland, MD, H. Fisher Raymond, San Francisco Department of Public Health, San Francisco, California; Sandra Miranda De León, MPH, Yadira Rolón Colón, MS, Departmento de Salud, San Juan, Puerto Rico; Leonard Bates PhD, Christopher Hucks-Ortiz, MPH, Christopher Lane, District of Columbia HIV/AIDS Administration, Washington, DC; and members of the NHBS team, Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), CDC. Additional assistance in the production of this report was provided by Marie Morgan, Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), CDC. References
Table 1 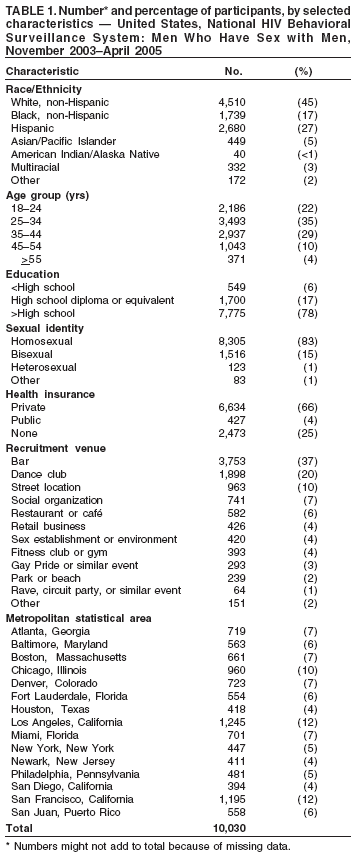 Return to top. Figure 1 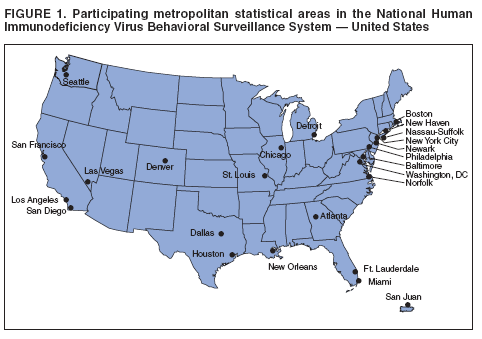 Return to top. Table 2 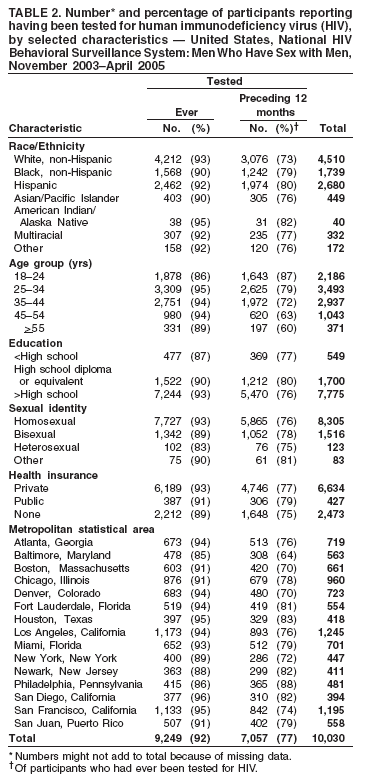 Return to top. Figure 2 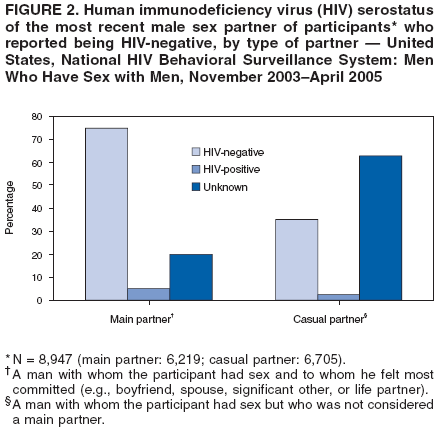 Return to top. Table 3 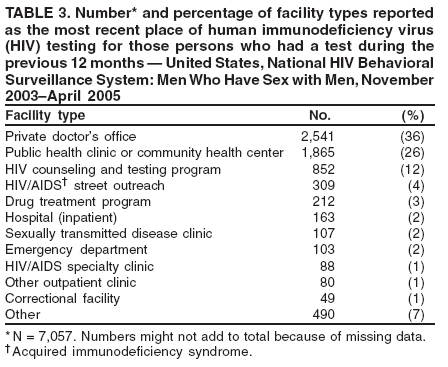 Return to top. Table 4 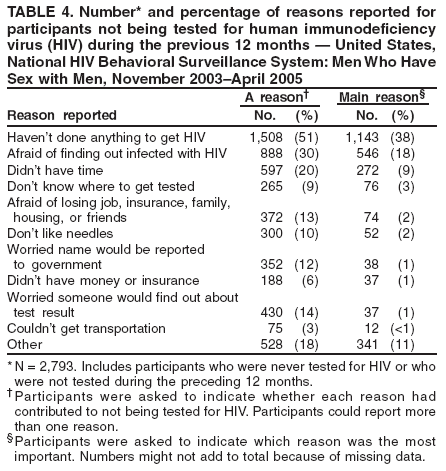 Return to top. Table 5 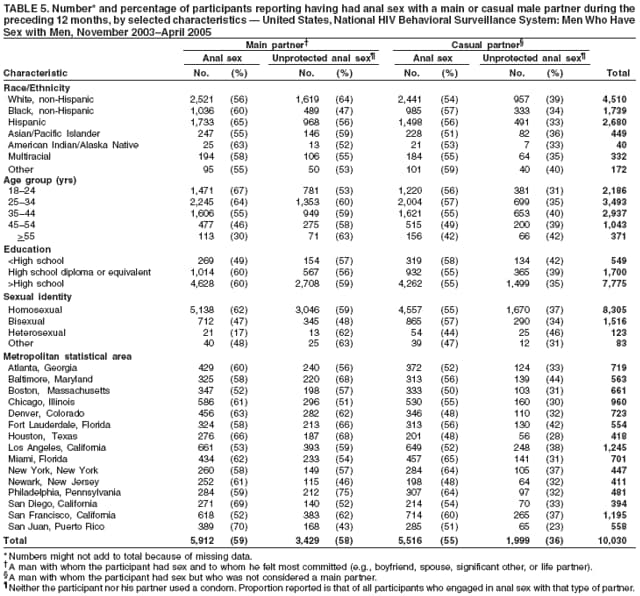 Return to top. Table 6 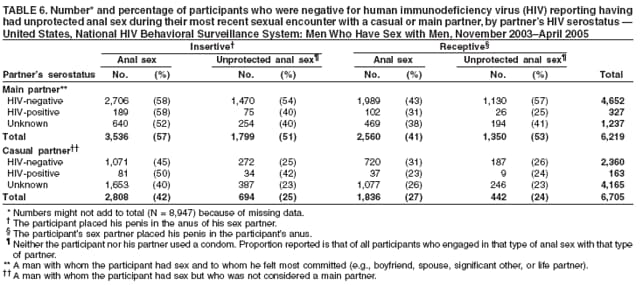 Return to top. Table 7 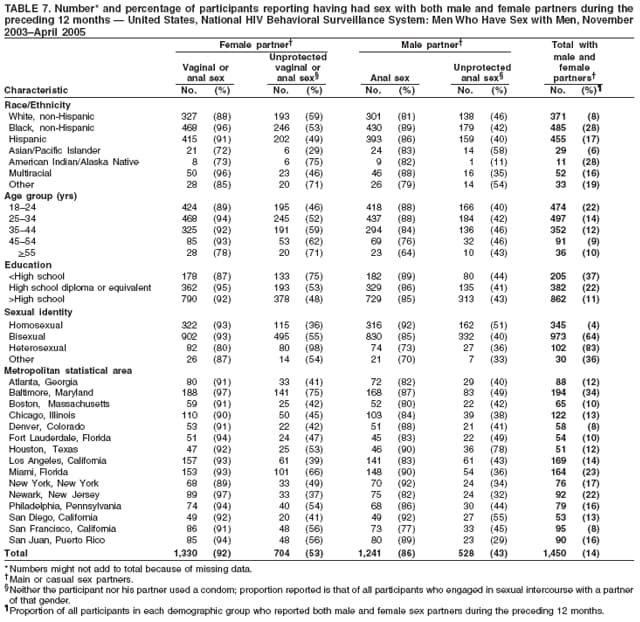 Return to top. Table 8 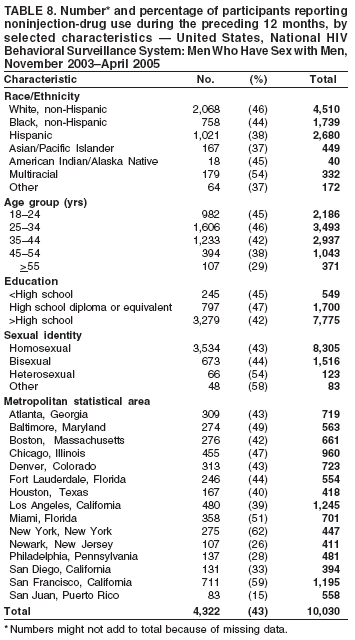 Return to top. Table 9 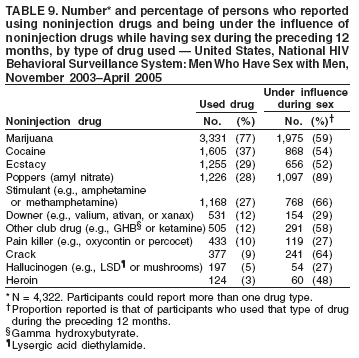 Return to top. Table 10  Return to top. Table 11 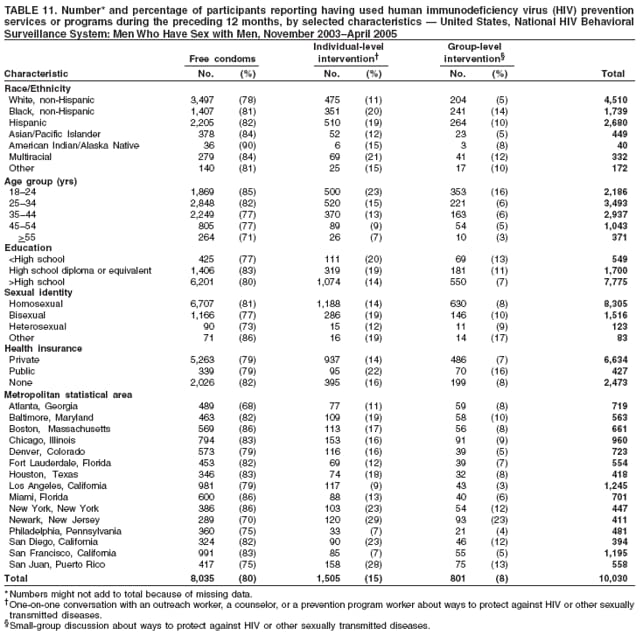 Return to top. Table 12 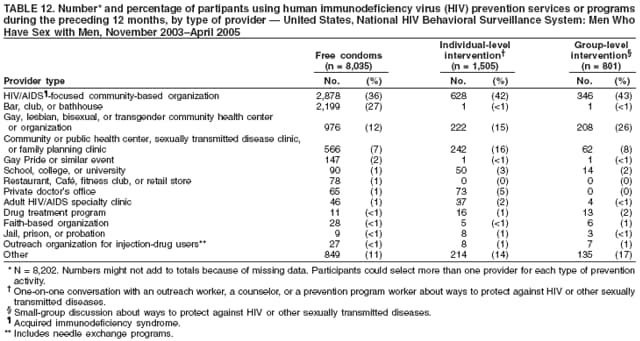 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/22/2006 |
|||||||||
|