ShareCompartir
ShareCompartir
FIGURE 1. Cumulative rate of hospitalizations during three influenza seasons, by age group --- Emerging Infections Program, United States, 2007--2010
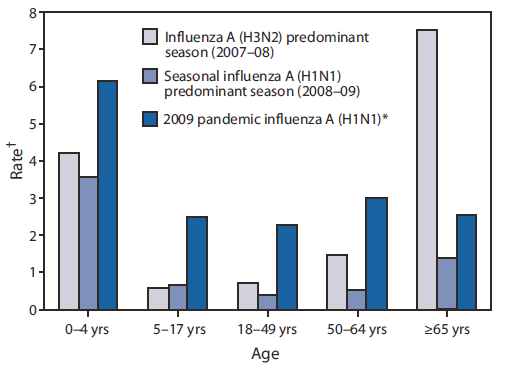
* 2009 Pandemic Influenza A(H1N1) hospitalization data from September 1, 2009--January 21, 2010.
† Per 10,000 population.
Alternate Text: The figure shows the cumulative rate of hospitalizations per 10,000 population by age group during three influenza seasons: 2007-08, 2008-09, and pandemic influenza A(H1N1) for September 1, 2009-January 21, 2010.