|
|
|
|
|
|
|
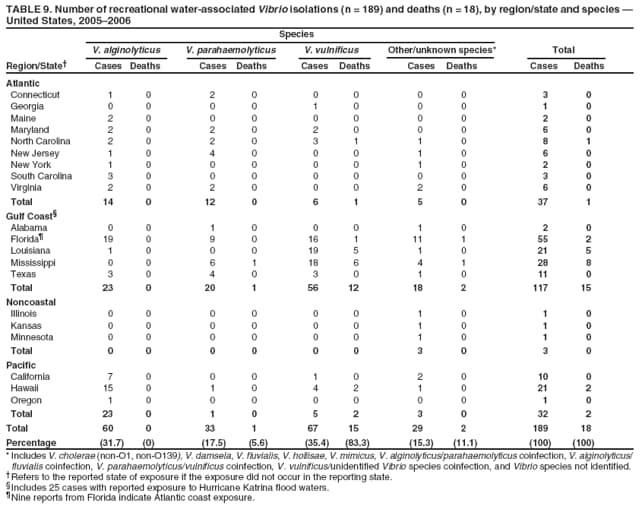
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
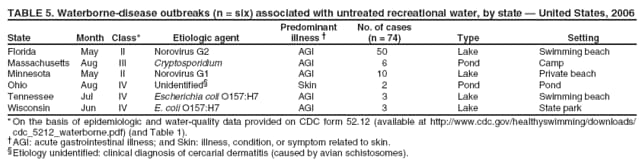
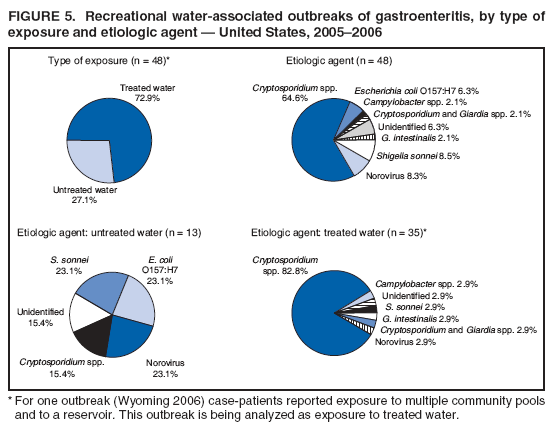
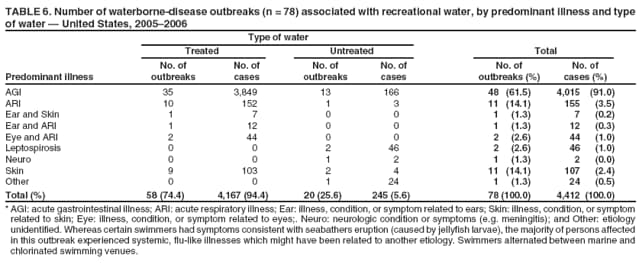
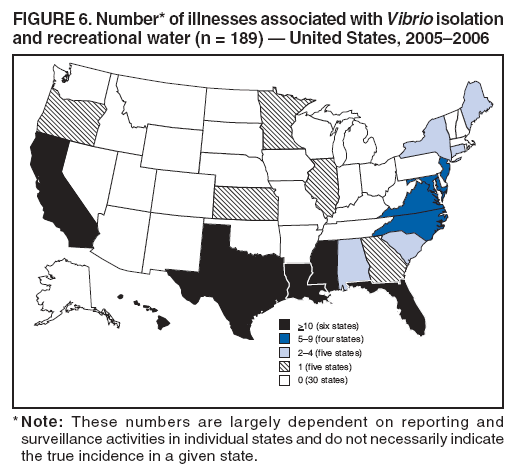
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Waterborne Disease and Outbreaks Associated with Recreational Water Use and Other Aquatic Facility-Associated Health Events --- United States, 2005--2006Jonathan S. Yoder, MSW, MPH1
Corresponding author: Jonathan S. Yoder, MSW, MPH, Division of Parasitic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, 4770 Buford Hwy., NE, MS F-22, Atlanta, GA 30341. Telephone: 770-488-3602; Fax: 770-488-7761. E-mail: [email protected]. AbstractProblem/Condition: Since 1971, CDC, the U.S. Environmental Protection Agency, and the Council of State and Territorial Epidemiologists have collaboratively maintained the Waterborne Disease and Outbreak Surveillance System for collecting and reporting data related to waterborne-disease outbreaks (WBDOs) associated with drinking water. In 1978, WBDOs associated with recreational water (natural and treated water) were added. This system is the primary source of data regarding the scope and effects of disease associated with recreational water in the United States. In addition, data are collected on individual cases of recreational water-associated illnesses and infections and health events occurring at aquatic facilities but not directly related to water exposure. Reporting Period: Data presented summarize WBDOs and case reports associated with recreational water use that occurred during January 2005--December 2006 and previously unreported disease reports and outbreaks during 1978--2004. Description of the System: Public health departments in the states, territories, localities, and the Freely Associated States (i.e., the Republic of the Marshall Islands, the Federated States of Micronesia, and the Republic of Palau, formerly parts of the U.S.-administered Trust Territory of the Pacific Islands) have primary responsibility for detecting, investigating, and voluntarily reporting WBDOs to CDC. Although the surveillance system includes data for WBDOs and cases associated with drinking water, recreational water, and water not intended for drinking, only cases and outbreaks associated with recreational water and health events at aquatic facilities are summarized in this report. Results: During 2005--2006, a total of 78 WBDOs associated with recreational water were reported by 31 states. Illness occurred in 4,412 persons, resulting in 116 hospitalizations and five deaths. The median outbreak size was 13 persons (range: 2--2,307 persons). Of the 78 WBDOs, 48 (61.5%) were outbreaks of gastroenteritis that resulted from infectious agents or chemicals; 11 (14.1%) were outbreaks of acute respiratory illness; and 11 (14.1%) were outbreaks of dermatitis or other skin conditions. The remaining eight were outbreaks of leptospirosis (n = two), primary amebic meningoencephalitis (n = one), and mixed or other illnesses (n = five). WBDOs associated with gastroenteritis resulted in 4,015 (91.0%) of 4,412 illnesses. Fifty-eight (74.4%) WBDOs occurred at treated water venues, resulting in 4,167 (94.4%) cases of illness. The etiologic agent was confirmed in 62 (79.5%) of the 78 WBDOs, suspected in 12 (15.4%), and unidentified in four (5.1%). Thirty-four (43.6%) WBDOs had a parasitic etiology; 22 (28.2%), bacterial; four (5.1%), viral; and two (2.6%), chemical or toxin. Among the 48 gastroenteritis outbreaks, Cryptosporidium was confirmed as the causal agent in 31 (64.6%), and all except two of these outbreaks occurred in treated water venues where Cryptosporidium caused 82.9% (29/35) of the gastroenteritis outbreaks. Case reports associated with recreational water exposure that were discussed and analyzed separately from outbreaks include three fatal Naegleria cases and 189 Vibrio illnesses reported to the Cholera and Other Vibrio Illness Surveillance System. For Vibrio reporting, the most commonly reported species were Vibrio vulnificus, V. alginolyticus, and V. parahaemolyticus. V. vulnificus illnesses associated with recreational water exposure had the highest Vibrio illness hospitalization (77.6%) and mortality (22.4%) rates. In addition, 32 aquatic facility-related health events not associated with recreational water use (e.g., pool chemical mixing accidents) that occurred during 1983--2006 were received from New York. These events, which caused illness in 364 persons, are included in this report but analyzed separately. Interpretations: The number of WBDOs summarized in this report and the trends in recreational water-associated disease and outbreaks demonstrate a substantial increase in number of reports from previous years. Outbreaks, especially the largest ones, occurred more frequently in the summer at treated water venues and caused gastrointestinal illness. Deficiencies leading to WBDOs included problems with water-quality, venue design, usage, and maintenance. Case reports of illness associated with recreational water use expand our understanding of the scope of waterborne illness by further underscoring the contribution of less well-recognized swimming venues (e.g., oceans) and illness (e.g., nongastrointestinal illness). Aquatic facilities are also a focus for injuries involving chemicals or equipment used routinely in the operation of swimming venues, thus illustrating the lack of training of some aquatics staff. Public Health Actions: CDC uses WBDO surveillance data to 1) identify the etiologic agents, types of aquatic venues, water-treatment systems, and deficiencies associated with outbreaks and case reports; 2) evaluate the adequacy of efforts (i.e., regulations and public awareness activities) to provide safe recreational water; 3) expand the scope of understanding about waterborne disease and health events associated with swimming and aquatics facilities; and 4) establish public health prevention priorities, data, and messaging that might lead to improved regulations, guidelines, and prevention measures at the local, state, and federal levels. IntroductionDuring 1920--1970, statistical data regarding waterborne-disease outbreaks (WBDOs) in the United States were collected by different researchers and federal agencies (1). Since 1971, CDC, the U.S. Environmental Protection Agency (EPA), and the Council of State and Territorial Epidemiologists (CSTE) have collaboratively maintained the Waterborne Disease and Outbreak Surveillance System (WBDOSS), a surveillance system that tracks the occurrences and causes of WBDOs and cases of disease associated with drinking water (2--11). In 1978, WBDOs associated with recreational water were added to the surveillance system. The types of outbreaks and disease case reports included in the Surveillance Summaries have expanded multiple times to more accurately reflect the scope of waterborne disease in the United States. Outbreaks of Pontiac fever (PF) were added in 1989 (9), outbreaks of Legionnaires' disease (LD)were added in 2001 (3,12), and single cases of Vibrio illness reported to the Cholera and Other Vibrio Illness Surveillance System that were associated with recreational water use were added in 2003. WBDOs associated with drinking water and water not intended for drinking are presented in a separate report (13). WBDO surveillance activities are intended to 1) characterize the epidemiology of waterborne disease; 2) identify trends in the etiologic agents and other factors associated with WBDOs; 3) identify major deficiencies in providing safe recreational water; 4) encourage public health personnel to detect and investigate WBDOs; 5) foster collaboration among local, state, federal, and international agencies on initiatives to prevent waterborne disease; and 6) collect data needed to support future prevention efforts. Additional data on cases of waterborne disease related to recreational water are gathered from separate disease surveillance systems and through supplementary surveillance activities (Figure 1). Some of these data are collected and analyzed in WBDOSS, and some are discussed in this report. These data are useful for expanding our understanding of the scope of waterborne disease, identifying important factors associated with unsafe or unhealthy recreational water, influencing research priorities, supporting public health recommendations, and encouraging improved water-quality policies and regulations. However, WBDOs and case reports summarized in this report are thought to represent only a portion of the illness associated with recreational water exposure. Reliable estimates of the number of unrecognized WBDOs are not available. In addition, the surveillance information described in this report does not include estimates of the number of recreational water illnesses (RWIs). BackgroundRegulation of Recreational Water QualityIn the United States, state and local governments establish and enforce regulations for protecting recreational water from naturally occurring or human-made contaminants. For treated water venues (e.g., swimming pools and water parks), no federal regulatory agency has authority, and no national guidelines for standards of design, construction, operation, disinfection, or filtration exist, except recent regulation to prevent entrapment injuries (14). Swimming pool codes are developed and enforced by state and local health departments; therefore, substantial variation is observed across the country in terms of policy, compliance, and enforcement (15). Efforts are underway to develop a Model Aquatic Health Code (available at http://www.cdc.gov/healthyswimming/model_code.htm) to be used as a national voluntary guideline. These data-driven and knowledge-based guidelines will be focused on promoting healthy recreational water experiences by preventing disease and injuries. The model code will be available to state and local health agencies needing guidance in writing, updating, and implementing state or local pool codes and might help standardize pool codes across the United States. EPA sets guidelines for recreational use of natural waters (e.g., lakes, rivers, and oceans). In 1986, EPA developed recommended bacterial water-quality criteria for coastal recreation waters (16) and recently established federal standards for those states and territories that have not yet adopted water-quality criteria that meet or exceed the 1986 criteria (17). For freshwater, full-body contact beaches (e.g., lakes and rivers), EPA has recommended that the monthly geometric mean water-quality indicator concentration be <33 CFU/100 mL for enterococci or <126 CFU/100 mL for Escherichia coli. For marine-water, full-body contact beaches, EPA has recommended that the monthly geometric mean water-quality indicator concentration be <35 CFU/100 mL for enterococci. However, state and local authorities have discretionary authority to determine which interventions should be used (e.g., posting signs to alert visitors of water contamination or closing the beach for swimming) when these limits have been exceeded. Beach Watch, EPA's Action Plan for Beaches and Recreational Waters (report available at http://www.epa.gov/waterscience/beaches/technical.html), was published in 1999 as part of the Clean Water Action Plan (available at http://www.epa.gov/beaches). The intent of Beach Watch is to assist state, tribal, and local authorities in strengthening and extending existing programs to protect users of fresh and marine recreational waters; as part of the BEACH Act of 2000, the U.S. Congress directed EPA to update its guidelines for recreational water use on the basis of improved water-quality indicators and testing. As a result, EPA has been collaborating with CDC since 2002 on the National Epidemiologic and Environmental Assessment of Recreational (NEEAR) Water Study at fresh and marine water recreational beaches in the United States. Information on the NEEAR is available at http://www.epa.gov/nheerl/neear. This study is being conducted to evaluate rapid new water-quality methods that are able to produce results in <2 hours and to correlate these indicators with health effects among beachgoers. Results from freshwater Great Lakes beaches have demonstrated an association between an increasing signal detected by a quantitative polymerase chain reaction-based test method for enterococci and human health effects (18, 19). Children aged <10 years were at greater risk for gastrointestinal illness following exposure (19) to water with elevated levels of enterococci. MethodsData SourcesPublic health departments in individual states, territories, localities, and the Freely Associated States (FAS)* have the primary responsibility for detection and investigation of WBDOs. The outbreaks are voluntarily reported to CDC through a standard form (i.e., CDC form 52.12; available at http://www.cdc.gov/healthyswimming/downloads/cdc_5212_waterborne.pdf). The form solicits data on WBDO, including characteristics of person, place, and time and results of epidemiologic studies, disease symptoms, diagnostic testing, and water sampling. Information gathered regarding the setting of the outbreak includes the type of aquatic facility, water source and treatment, sanitary measures in place, and possible factors contributing to the contamination of the water. Public health professionals in each state or locality are designated as WBDO surveillance coordinators, and CDC annually requests reports from coordinators in all states and localities and conducts as much follow-up correspondence as needed to resolve unaddressed questions. Although national reporting only includes WBDOs, single cases of certain waterborne diseases (e.g., primary amebic meningoencephalitis (PAM) and chemical toxin poisoning) are also solicited from coordinators. Outbreaks, cases, or other health events, where applicable, are assigned to a state on the basis of the location of the exposure rather than state of residence of ill persons. Numeric and text data from the CDC waterborne disease outbreak form and any supporting documentation are entered into a database for analysis. Although all WBDOs are collected through the same CDC reporting system, the recreational water-associated outbreaks are analyzed and published separately from drinking water-associated outbreaks and other WBDOs (13). Information on WBDOs and cases is sometimes solicited from other CDC surveillance systems and confirmed with the state or locality for inclusion in WBDOSS or Surveillance Summary (Figure 1). Vibrio illnesses associated with recreational water exposure were received from the Cholera and Other Vibrio Illness Surveillance System. Definitions†Waterborne Disease Outbreaks The unit of analysis for the summary is an outbreak, not an individual case of a waterborne disease. To be defined as a WBDO associated with recreational water, an event must meet two criteria. First, two or more persons must be epidemiologically linked by the location of the exposure to recreational water, time, and illness. Recreational water settings include swimming pools, wading pools, spas, waterslides, interactive fountains, wet decks, and fresh and marine bodies of water. Second, the epidemiologic evidence must implicate water or volatilization of water-associated compounds into the air surrounding an aquatic facility as the probable source of the illness. For this report, WBDOs are separated by venue as untreated (i.e., fresh and marine surface water) or treated (i.e., filtered or disinfected [e.g., chlorinated]) water. WBDOs associated with ships are not included in this report. Case Reports of Waterborne Illness or Reports of Aquatic Facility-Associated Health EventsThis report also includes 1) individual cases of laboratory-confirmed PAM associated with recreational water use, 2) single cases of wound infections or other Vibrio infections associated with recreational water use, 3) single cases of chemical and toxin poisoning if water or air-quality data indicate contamination by the chemical or toxin, and 4) outbreaks or case reports of health events associated with aquatic facilities but not associated with the recreational water but rather contaminated aquatic facility air (e.g., mixing of chemicals in the pump room might release toxic gas that injures staff or facility users) (Figure 1). Because these four event categories do not meet WBDO definition, they are analyzed separately from WBDOs. Strength of Evidence Classification for Waterborne-Disease OutbreaksWBDOs reported to WBDOSS are classified according to the strength of evidence that implicates water as the vehicle of transmission (Table 1). The classification scheme (i.e., Classes I--IV) is based on the epidemiologic and water-quality data provided on WBDO report form. Although in certain instances WBDOs without water-quality data were included in this report, outbreaks that lacked any epidemiologic data linking the outbreak to water were excluded. Class I indicates that adequate epidemiologic and water-quality data were reported (Table 1). However, the classification does not necessarily imply that an investigation was conducted optimally. Likewise, a classification of II, III, or IV does not imply that an investigation was inadequate or incomplete. Outbreaks and investigations occur under varying circumstances, and not all outbreaks can or should be rigorously investigated. In addition, outbreaks that affect fewer persons are more likely to receive classifications of III or IV because of the limited sample size available for data analysis. Changes in the 2005--2006 Surveillance SummaryThe definition of a waterborne outbreak has been modified for this report to be consistent with generally accepted public health practice (i.e., two or more epidemiologically linked cases associated with use of recreational water). Health events at aquatic facilities not associated with direct exposures to recreational water are, for the first time, presented and discussed but not analyzed as waterborne outbreaks. Definition Previously, the definition of a recreational waterborne disease outbreak included certain single cases of waterborne disease. The definition of a recreational waterborne-disease outbreak has been clarified to include two or more persons who have been epidemiologically linked to recreational water by location of exposure, time, and illness. Exposures include contact with or accidental ingestion of water and certain inhalation exposures (e.g., exposure to water-associated compounds [e.g., chloramines] volatilizing into the air of the aquatic facility). Single cases of PAM, recreational water-associated Vibrio illness, and illness related to chemical exposure caused by water are included in WBDOSS but are not classified or analyzed as outbreaks. These single cases are analyzed separately. Aquatic Facility-Related Health Events not Associated with Recreational Water Previous Surveillance Summaries only included outbreaks in which the vehicle of transmission was water or airborne chemical products originating from water (e.g., chloramines). Nonwater-related illnesses resulting from chemical inhalation or exposure at aquatic facilities have not been discussed in previous Surveillance Summaries. This report includes, as a separate analysis, chemical injury (e.g., mixing of pool chemicals that release toxic gas) cases and outbreaks at aquatic facilities in which direct exposure to water was not the cause of illness. Whereas these events are not classified or analyzed as waterborne outbreaks, they highlight important public health and safety concerns related to the design, operation, and maintenance of recreational water venues and are targeted to the same audiences who are the focus of the waterborne disease and outbreaks already included in this report. ResultsWaterborne-Disease OutbreaksExcluding Vibrio and PAM cases and aquatic facility-related health events, a total of 78 outbreaks (38 in 2005 and 40 in 2006) associated with recreational water were reported to CDC (Tables 2--5). This is the highest number of outbreaks reported for a 2-year summary since reporting began in 1978. Of the 50 states and 10 territories, localities, and FAS participating in WBDOSS, 31 states reported WBDOs (Figure 2). Descriptions of selected WBDOs are presented in this report (Appendix B, Selected Descriptions of Waterborne Disease and Outbreaks [WBDOs] Associated with Recreational Water). These 78 outbreaks affected 4,412 persons and resulted in five deaths. The median outbreak size was 13 persons (range: 2--2,307 persons). Minnesota reported the highest number of WBDOs (nine), New York and Florida each reported seven WBDOs, and Wisconsin reported six WBDOs. During 2005--2006, treated water venues were associated with 58 (74.4%) of the recreational water outbreaks and 4,167 (94.4%) of the cases (Tables 2 and 3; Figure 3). Untreated venues were associated with 20 (25.6%) of WBDOs but only 245 (5.6%) of the cases (Tables 4 and 5). Of the 78 WBDOs, 48 (61.5%) were outbreaks of acute gastroenteritis illness (AGI), 11 (14.1%) were outbreaks of dermatitis or other skin conditions, and 11 (14.1%) were outbreaks of acute respiratory illness (ARI). The remaining WBDOs resulted in leptospirosis (n = two), PAM (n = one), and mixed or other illnesses (n = five) (Table 6, Figure 3). WBDOs associated with gastroenteritis accounted for 4,015 (91.0%) of the cases of illness. The route of entry implicated for each WBDO was ingestion for 48 outbreaks (61.5%), inhalation for 10 (12.8%), contact for 8 (10.3%), combined routes for nine (11.5%), and other (Naegleria and Leptospira) for three (3.8%) Figure 3). WBDOs occurred in every calendar month. However, the summer months (June through August) accounted for 51 (65.4%) WBDOs and 3,890 (88.2%) cases (Figure 4). Gastroenteritis was particularly clustered during these months with 40/48 (83.3%) outbreaks and 3,777/4,015 (94.1%) cases being reported. Etiologic Agents Of the 78 WBDOs associated with recreational water, the etiologic agent was confirmed in 62 (79.5%), suspected in 12 (15.4%) and unidentified in four (5.1%) (Table 7). Thirty-four (43.6%) outbreaks were confirmed as being caused by parasites; 22 (28.2%), bacteria; four (5.1%), viruses; and two (2.6%), chemicals (Figure 3). Of the 47 outbreaks associated with treated water venues with an identified etiologic agent: 31 (66.0%) involved parasites; 14 (29.8%), bacteria; one (2.1%), a virus; and one (2.1%) a chemical (Table 7). Parasites were responsible for approximately 20 times more cases than bacteria (3,784 versus 167). Of the 15 WBDOs associated with untreated water venues with an identified etiologic agent, eight (53.3%) involved bacteria; three (20.0%) parasites; three (20.0%) viruses; and one (6.7%) a chemical. Parasites Of the 48 outbreaks of gastroenteritis, 33 (68.8%) were parasitic in origin, including 31 (93.9%) caused by Cryptosporidium, one (3.0%) caused by Giardia intestinalis, and one (3.0%) caused by both Cryptosporidium and Giardia (Tables 2--7; Figure 5). Of the 13 gastroenteritis outbreaks associated with untreated water venues, only two (15.4%) were caused by parasites. Two cryptosporidiosis outbreaks occurred; one in an untreated lake and the other in an untreated pond, causing 27 and six cases of illness, respectively. In contrast, parasites were the most common causes of gastroenteritis outbreaks associated with treated water venues; Cryptosporidium was the most common parasitic agent, causing 29 (82.9%) of the 35 outbreaks of gastroenteritis. Thirty-one of these parasitic gastroenteritis outbreaks occurred in treated water venues, causing illness in 3,784 persons. Three of these outbreaks each caused over 100 (range: 116--2,307 persons) cases of illness. In June 2005, an outbreak caused by C. hominis transmitted through a New York spray park resulted in 2,307 cases, mostly among young children. In August 2005, a C. hominis outbreak spread through multiple Ohio pools and resulted in 523 cases; this outbreak subsequently was linked to an outbreak in an adjoining state (Kentucky). In June 2006, an outbreak caused by Cryptosporidium at a water park in Missouri caused gastroenteritis in 116 persons The one additional parasitic outbreak was caused by Naegleria fowleri and led to the death of two persons in Oklahoma. Despite an investigation by local public health authorities, the location of suspected common exposure (i.e., exposure in which the two persons probably became ill at the same time and place) was not identified. Bacteria Eight reported gastroenteritis outbreaks of confirmed bacterial origin were reported (Figure 5), two of which were at treated water venues. An outbreak of Campylobacter jejuni occurred in a fill-and-drain pool at a Wyoming home in July 2005, resulting in five children and one adult becoming ill. This same type of pool was the setting for a Shigella sonnei outbreak at a California home in July 2006, leading to nine persons becoming ill, including three who were hospitalized. Both of these outbreaks were caused by a lack of disinfection and heavy use of these pools by young diaper-aged children. The other six outbreaks of gastroenteritis, caused by bacteria, were associated with swimming in lakes, including three additional shigellosis outbreaks and three outbreaks of E. coli O157:H7 infection. All six lake-associated outbreaks occurred during June and July and five were associated with exposure to lake water during holidays or weekends. Four of the bacterial outbreaks involved 28 cases of dermatitis caused by Pseudomonas aeruginosa; one of these outbreaks also resulted in ear infections. All four outbreaks of Pseudomonas infection occurred at treated water venues that involved heated spa water (some of these outbreaks also involved pools). Five additional outbreaks were suspected to have been caused by Pseudomonas on the basis of the clinical symptoms and exposure to a spa. Eight outbreaks caused by Legionella were associated with treated recreational water venues during 2005--2006, causing 124 cases of legionellosis (i.e., LD and PF) and resulted in three deaths. The largest of these outbreaks was linked to a spa at an Illinois hotel and involved 43 persons, including three cases of LD resulting in one death. The environmental investigation documented inadequate disinfection in the spa and isolated both L. pneumophila and L. maceachernii from the spa water. Two outbreaks in untreated recreational water were caused by Leptospira. Leptospirosis was diagnosed in 43 persons who participated in an adventure race in Florida in November 2005. A July 2005 outbreak of leptospirosis in California involved three persons who had contact with water from a low flowing stream at the time of exposure Viruses Four outbreaks of confirmed viral origin occurred, all of which caused gastroenteritis. Norovirus was identified as the etiologic agent in each of the outbreaks; three occurred at lake swimming beaches, and one occurred in a treated water setting. These four norovirus outbreaks resulted in 86 cases of gastroenteritis. For the two outbreaks where lake water fecal indicator testing was conducted; no water quality-violations were documented. The water might have been contaminated by ill swimmers at the time of exposure rather than by ongoing point source water contamination. The treated venue outbreak occurred in a hotel pool and was related to inadequate disinfection and continued use by ill swimmers. One additional outbreak that was suspected to have been caused by norovirus resulted in 13 cases. Chemicals During 2005--2006, two outbreaks associated with chemicals involved 22 persons. In June 2005, a chemical-associated outbreak occurred in a Michigan lake causing respiratory symptoms in three swimmers. This outbreak was attributed to the unapproved addition of excessive amounts of copper sulfate to the lake water for aquatic nuisance control. The other outbreak occurred in a treated water venue. In July 2005, the recirculation pump at a community pool was shut down for maintenance; however, the liquid chlorine (i.e., NaOCl) and muriatic (i.e., hydrochloric) acid continued to feed into the system and probably released chlorine gas in the piping. When the pump was restarted, a concentrated bolus of these swimming pool chemicals and chlorine gas was sent into a small pool where it caused respiratory distress in 19 persons. Three additional outbreaks in treated venues were suspected of being caused by disinfection by-products (e.g., chloramines) on the basis of symptoms and settings (i.e., indoor pool). Suspected Agents Twelve outbreaks were reported in which no etiologic agent was confirmed; however, investigation reports indicated a suspected agent on the basis of symptoms, type of water, setting, and background information (Table 7). Five of these 12 outbreaks were suspected to be caused by P. aeruginosa in treated spas. One outbreak, which caused rashes in nine children, was suspected of being caused by low pH. Three chemical-related outbreaks were suspected to be associated with exposure to excess chloramines (i.e., disinfection by-products of chlorination) (20--22) in the indoor pools and surrounding areas (i.e., indoor pool air), which resulted in ARI, and eye irritation. Norovirus was the suspected pathogen in one gastroenteritis outbreak associated with a lake on the basis of epidemiologic and clinical evidence. Two outbreaks were suspected to be the result of contact with avian schistosomes, causing cercarial dermatitis Unidentified Etiologic Agents Data collected during investigations of four outbreaks of unidentified etiology were not sufficient to suggest an etiologic agent. Gastroenteritis was reported as the predominant illness in two of these outbreaks, and ARI and ear infections were reported for the third one. The AGI outbreak in a treated venue (Minnesota 2005) caused illness in 32 persons over the course of nearly a month; 15 persons reportedly continued to swim while ill. Stool samples tested negative for bacteria, viruses, and parasites. A lake-associated AGI outbreak sickened 10 persons and caused five hospitalizations. Environmental testing revealed water-quality violations (e.g., elevated E. coli levels). An outbreak of ARI and ear infections among lifeguards occurred in a pool that had not officially opened for the season. The water was reportedly cloudy and possibly contaminated by water leaking from a pipe in the facility. Finally, an outbreak of influenza-like illness linked to an ocean beach was associated with marine and pool water; possible etiologies might include contact with jellyfish larvae and other etiologies may have contributed to some of these illnesses. Single Cases of Waterborne DiseaseVibriosis Cases Associated with Recreational Water During 2005--2006, a total of 189 vibriosis cases associated with recreational water use or exposure to flood water were reported from 20 states; representing 14.7% (189/1287) of the total number of vibriosis cases reported in 2005--2006 (62). Eighty-five (45.0%) of 189 patients were hospitalized, and 18 (9.5%) died (Table 8). The most frequently isolated Vibrio species was Vibrio vulnificus, which was isolated from 67 (35.4%) persons; 52 (77.6%) were hospitalized, and 15 (22.4%) died. V. alginolyticus was isolated from 60 (31.7%) persons; seven (11.7%) were hospitalized, and none died. V. parahaemolyticus was isolated from 33 (17.5%) persons; 12 (36.4%) were hospitalized, and one (3.0%) died. Other Vibrio species (including V. cholerae non-O1, non-O139, V. damsela, V. fluvialis, V. hollisae, V. mimicus, V. alginolyticus/parahaemolyticus coinfection, V. alginolyticus/fluvialis coinfection, V. parahaemolyticus/vulnificus coinfection, V. vulnificus/unidentified Vibrio species coinfection and Vibrio species not identified) were identified in 29 (15.3%) persons; 14 (48.3%) were hospitalized, and two (6.9%) died. Geographic location. Nearly all Vibrio patients reported that they were exposed to recreational water in a coastal state (Figure 6). The most frequently reported location was the Gulf Coast (61.9%); Atlantic Coast states, excluding Florida (19.6%); Pacific Coast states (16.9%); and inland states (1.6%) (Table 9). Florida and Mississippi reported the highest number of cases, 55 and 28 cases, respectively (Figure 6; Table 9). Seasonality. The temporal distribution of illness in patients from whom Vibrio species were isolated displayed a clear seasonal peak during the summer (Figure 7). The greatest frequency of Vibrio cases occurred during July through September. Exposures. Activities associated with Vibrio cases included swimming, diving, or wading in water (70.9%); walking or falling on the shore or rocks (32.8%); and boating, skiing, or surfing (19.6%). Twenty-five case-patients reported exposure to Hurricane Katrina flood waters. Signs/Symptoms. Symptoms associated with Vibrio illnesses included cellulitis (56.6%), fever (36.0%), muscle pain (21.2%), bullae (15.9%), ear infections (14.3%), nausea (13.8%), and shock (10.1%). V. vulnificus accounted for the majority of skin infections (e.g., cellulitis, bullae), causing 70 (50.7%) of 138. V. vulnificus also accounted for the majority of severe illnesses, including those with fever (51.5%), bacteremia (75.0%), shock (73.7%), and amputations (83.3%). V. alginolyticus accounted for the majority of ear infections (24 [92.3%] of 26). Other symptoms and infections were reported in low frequencies (e.g., bladder infections, hematuria, eye infections, respiratory symptoms, sinus infections, diarrhea, and vomiting). Naegleria Infections In addition to the outbreak of PAM (two cases), three individual fatal cases of PAM caused by N. fowleri were reported in 2005--2006 (Table 10). A child in Texas died in September 2005, 13 days after swimming in a lake. In August 2006, a child died of PAM associated with N. fowleri after swimming, using a personal watercraft, and tubing in an Arizona lake. In August 2006, a child died after swimming in a Georgia pond. Previously Unreported Outbreaks Thirty-one previously unreported recreational water-associated outbreaks and one case of waterborne disease during 1978--2004 were received and entered into WBDO database (Table 11). These outbreaks were summarized but not included in analysis for this report. One outbreak of leptospirosis in Hawaii was associated with exposure to flood water (48). Reports on the remaining 30 events were received from Minnesota, New York, and Tennessee. These states participate in the Environmental Health Specialist Network Water program (EHS-Net Water), which is an EPA and CDC funded initiative that supports a waterborne-disease environmental health specialist in each site. These three sites identified outbreaks and case reports that were previously unreported to CDC and reported them as part of a retrospective review of waterborne disease outbreaks in these states. The 31 previously unreported outbreaks affected 673 persons; 25 (80.6%) of the outbreaks occurred in treated water venues. Surveillance Reports Not Classified as Waterborne Disease and OutbreaksOne report from New Hampshire was not included in this summary. In February 2005, three children had lesions believed to be caused by Molluscum contagiosum. These children all swam at the same community pool; however, after investigation, it was not clear that these lesions were associated with waterborne transmission of this organism versus other modes of transmission (e.g., person to person or contact with contaminated towels or objects). Aquatic Facility-related Health Events not Associated with Recreational Water Thirty-two reports of nonwater related health events that occurred during 1983--2006 and were associated with aquatic facilities were reported by New York (Table 12). Although they are not counted as waterborne-disease cases or outbreaks for analysis purposes, they are included in this report because they illustrate important lessons about pool maintenance and operation. Most of these events, 90.6% (29/32), were caused by improper use of chemicals; incompatible pool chemicals (e.g., acid and bleach) were mixed, which resulted in the release of chlorine gas. Persons at these aquatic facilities experienced respiratory distress. Two additional events were caused by carbon monoxide in indoor pools, and one event was caused by liquid chlorine splashing into the eye of an aquatic facility employee. DiscussionTrends in Reporting OutbreaksA total of 78 recreational water--associated WBDOs were reported to CDC during 2005--2006. This represents an increase from the 2003--2004 Surveillance Summary (n = 62) and is the largest number of outbreaks ever reported in a 2-year period (Figure 8). Overall, the number of reported recreational water-associated WBDOs reported annually have increased substantially since 1978, when CDC first began receiving these reports (Figure 8). These increases probably are a result of a combination of factors, such as the emergence of pathogens (e.g., Cryptosporidium), increased participation in aquatic activities, and increases in the number of aquatic venues. Increased recognition, investigation, and reporting of recreational water-associated outbreaks also might be contributing factors. An unprecedented number of states reported outbreaks during 2005--2006, and WBDOs demonstrate geographic variation (Figure 2). Differences in reporting between states might be attributable to several factors, including ability to detect outbreaks, availability of laboratory testing, variable requirements for notifiable diseases, and the surveillance and investigation capacity of individual state and local public health agencies. These differences in the ability to detect, investigate, and report WBDOs probably lead to reporting and surveillance bias. Therefore, the states with the majority of outbreaks reported for this period might not be the states in which the majority of outbreaks actually occurred. An increase or decrease in the number of WBDOs reported might reflect either an actual change in the incidence of outbreaks or a change in the sensitivity of surveillance systems. Etiologic agents with shorter incubation periods might be more easily linked to water exposures, facilitating the recognition of outbreaks. Additional factors that might influence which WBDOs are reported include the size and location of the outbreak, severity of illness, and the geographic dispersion of ill persons. Larger outbreaks are more likely to be identified by public health authorities. In contrast, smaller outbreaks (e.g., those associated with private residential pools and spas) might go undetected because fewer persons are ill, and they might attribute illness to other common exposures. In addition, outbreaks of gastroenteritis associated with large venues that draw from a wide geographic range (e.g., large lakes and marine beaches) might be difficult to detect because potentially infected persons disperse widely from the site of exposure and, therefore, might be less likely to be identified as part of an outbreak. Prospective epidemiology studies, such as the EPA's NEEAR Water Study (18), have revealed elevated rates of gastroenteritis in swimmers compared with nonswimmers on all beaches studied. Multiple other prospective studies of gastroenteritis associated with beach swimming have also indicated elevated rates of illness associated with swimming in lakes and oceans, though few outbreaks have been detected (23,24). Consistent with this finding, no ocean-associated outbreaks and only one Great Lakes-associated outbreak of gastroenteritis has been reported since 1978 (12). These endemic recreational water-associated illnesses are not captured by WBDOSS, supporting the need for more studies to estimate the magnitude of risk for illness for routine, nonoutbreak-associated exposures at recreational water venues. WBDOs associated with recreational water use occur year-round, but the numbers of reported WBDOs and cases are highest during the annual summer swim season (Figure 4). For public health professionals and swimming venue operators, the seasonality of waterborne-disease outbreaks can help determine the allocation of resources so that health education messages are targeted to populations during times of the year when the risk for preventable illness is highest. Swimming PoolsSwimming pools are designed to be chemically treated and filtered to reduce the risk for illness associated with exposure to infectious pathogens. Despite the availability of these disinfection measures, pools remain susceptible to contamination because of chlorine-resistant organisms (i.e., Cryptosporidium) or inadequate treatment resulting from poor operation or maintenance. In addition, an emerging focus of concern at swimming pools is the risk for chemical injury from improper handling of pool chemicals. Infectious Gastroenteritis Approximately 87% of all cases reported to WBDOSS during 2005--2006 were involved in infectious gastroenteritis outbreaks associated with treated recreational water venues. Two outbreaks were caused by chlorine-sensitive agents (Giardia in Massachusetts, July 2005, and norovirus in Wisconsin, May 2006) and might have been prevented or reduced in scale by proper aquatic monitoring, maintenance, and/or operation practices. Investigation of the Massachusetts giardiasis outbreak revealed that although the chlorine levels recorded on the pool log were below the recommended level, no documented response existed that indicated that chlorine was added or that the pool was closed. Previous outbreak investigations have demonstrated that the implementation of appropriate pool operation practices (e.g., adequate disinfection) effectively stops the transmission of chlorine-sensitive pathogens (25). During 2005--2006, Cryptosporidium spp. caused 31 recreational water--associated outbreaks, which involved 3,751 persons; 99.1% of these cases were associated with treated water venues. The number of the cryptosporidiosis outbreaks reported annually has substantially increased from nine in 1997--1998 to 31 in 2005--2006 (Table 7). This increase is particularly noticeable in the proportion of AGI outbreaks associated with Cryptosporidium in treated recreational water venues (Figures 5 and 9). These increases contribute to the observed increases in the total number of recreational water--associated outbreaks and, more specifically, outbreaks of gastroenteritis. Concurrently, cases of cryptosporidiosis reported to CDC have nearly doubled since 2004 (26). Although the reasons for increased cryptosporidiosis case and outbreak reporting are not completely understood, outbreaks associated with treated recreational water venues continue to be an important means of transmitting Cryptosporidium. During 1997--2006, Cryptosporidium was infrequently attributed to outbreaks associated with lakes and rivers (12.7% of outbreaks), although it caused 68.3% of outbreaks associated with treated venues (Figure 9). This observation is consistent with the finding that Cryptosporidium requires extended contact time with chlorine for inactivation; oocysts can survive for days in the chlorine levels that are typically recommended for swimming pools (1--3 ppm free chlorine; 27). The continued reporting of cryptosporidiosis outbreaks associated with the use of treated recreational water venues underscores the importance of other prevention measures that reach beyond conventional pool chlorination and filtration, which are the primary barriers to infectious disease transmission (28). WBDOs of crypto-sporidiosis have stimulated the use of alternative treatment technologies and other potential risk-reduction steps to keep swimming venues safe. Ultraviolet light (29--31) and ozonation (27,32) disinfection effectively inactivate Cryptosporidium and are available for use at aquatic venues. Other potential risk-reduction steps include increased circulation flow rates, flocculants, remedial biocidal shock treatments [i.e., routine hyperchlorination: 20 ppm free chlorine for 12.75 hours or the equivalent (31,33)], and occupancy-dependent water replacement. In addition, cryptosporidiosis outbreaks highlight the need for improved operator training and continued education of the general public concerning healthy swimming practices to reduce the risk for RWI. Because Cryptosporidium is resistant to the chlorine levels used in pools, outbreaks can occur, even in facilities that are well-maintained. Therefore, rapid public health response and increased community involvement are needed to prevent the expansion of these outbreaks (34). One cryptosporidiosis outbreak (Iowa, June 2005) that occurred in a community swimming pool demonstrates how a rapid community-wide public health response during the early stages of an outbreak can help control the potential spread of illness into the community. In Iowa, detection and investigation started 2 weeks after exposure. The response included mitigating actions (e.g., ordering hyperchlorination of the implicated pool and all pools within a 20-mile radius and then confirming compliance; containing the outbreak through collaborative efforts between epidemiologists and environmental health specialists; posting signs at the implicated pool's entrance; instructing those with diarrhea not to enter the pool; and educating the public about good hygiene practices). The investigation indicated that no transmission had apparently occurred outside of the single implicated community pool, suggesting that these control measures might have prevented further spread. An interstate cryptosporidiosis outbreak (Kentucky, June 2005; and Ohio, August 2005) highlighted the need for additional intra-agency collaboration (e.g., between epidemiologists detecting cases and environmental health specialists permitting and inspecting pools) and communication between states. Modification of swimming behavior is a critical component in reducing recreational water-associated outbreaks. Swimming is essentially communal bathing, and continued swimming during diarrheal illness and the common occurrence of swallowing recreational water pose a public health challenge. Multiple findings underscore the relation between human behavior and disease transmission at recreational water venues. First, in multiple outbreaks, fecal accidents were observed at the implicated pools on the days when the outbreak exposures were thought to have occurred (Florida, August 2006; and Illinois, July 2006). Second, at least five outbreaks (New York, June 2005; Ohio, August 2005; Illinois, July 2006; Minnesota, September 2006; and South Carolina, July 2006) were caused by Cryptosporidium hominis, indicating a human source of water contamination. Third, swallowing water at the implicated recreational water venue was associated with illness in three outbreaks (Colorado, August 2006; Florida, June 2005; and New York, June 2005). All of these outbreaks highlight how recreational water can amplify transmission of fecal-oral pathogens. These findings underscore the need for public education about the importance of not swimming during diarrheal illness and not swallowing recreational water, and the importance of clarifying with the public that recreational water is neither drinking water nor sterile. Aquatic facilities should be diligent about informing patrons of these public health concerns and emphasizing that persons with diarrhea should not swim and all swimmers should practice good hygiene. These policies should apply to all patrons, particularly young children and visitors from high-risk settings (e.g., child care centers), which have diarrhea exclusion policies but might not enforce them routinely. They also should apply to all aquatics facility staff. Standardized policies for restricting staff who are ill with diarrhea from entering pools, similar to restricting ill foodhandlers from food preparation, should be established, implemented, and enforced (35). Finally, good hygiene is essential to ensure the cleanliness of swimmers entering pools. An adequate number of functioning, accessible hygiene facilities (i.e., toilets, diaper-changing areas, and showers) should be located near pools and should provide hot water and handwashing access to promote compliance. Documented fecal contamination of persons (36) suggests that swimmers should be encouraged to shower thoroughly (i.e., washing the perianal surface in particular) before going to or entering the pool. Diaper-changing facilities, with handwashing stations, should be located close to or at the poolside to encourage hygienic diaper-changing and handwashing. Chemical Toxicity During 2005--2006, pool chemicals or disinfection by-products were confirmed as the etiologic agent in one (Ohio, July 2005) and suspected to be the etiologic agent in four (Minnesota, April 2005; Illinois, June 2006; Nebraska, December 2006; and New York, March 2006) pool-associated outbreaks. Chemicals are added to pool water to protect against microbial and algal growth, improve the water quality, maximize the efficacy of the disinfection process (e.g., pH control), and prevent corrosion and scaling of equipment. However, these same chemicals can become sources of illness or injury if they are not properly handled or if water quality and ventilation are poor. In an ARI outbreak in Ohio, a pool recirculation pump shut down for unknown reasons, but the chemical feed pump continued to feed hypochlorous acid and muriatic (hydrochloric) acid into the recirculation system, resulting in the release of chlorine gas into the pool that was still in use by swimmers when the recirculation pump was restarted. Nineteen persons became ill, of whom four of them were hospitalized. A dermatitis outbreak (Illinois) was suspected to have resulted from water chemistry deficiencies (pH <7 and chlorine level at 0 ppm) that occurred when the automatic chemical-feeding system malfunctioned. These outbreaks underscore the need for engineering controls (e.g., an electrical interlock system that shuts down the chemical feed pump when the recirculation pump shuts down), regular systems checks, and preventive maintenance of equipment. Three additional outbreaks of acute respiratory symptoms or eye irritation were suspected to have resulted from an accumulation of chloramines in the water and air of indoor pools. Chloramines are disinfection by-products that result from chlorine oxidation of nitrogenous compounds (e.g., perspiration, saliva, urine, and body oils) commonly shed into pools by swimmers (20). Chloramines are produced in the water and volatilize into the surrounding air. In indoor pool settings, chloramines can accumulate in the enclosed space if ventilation is inadequate (21). The resulting high levels of chloramines can cause ocular, respiratory tract, and mucous membrane irritation (20); these high levels in indoor pool settings are also potentially linked to asthma (37). The investigation of the Nebraska outbreak, which resulted in one young swimmer being admitted to a pediatric intensive-care unit for severe chemical epiglottitis and laryngotracheobronchitis, revealed inadequate facility maintenance that resulted in prolonged deterioration of the water chemistry (e.g., 0.8 ppm free chlorine, 4.2 ppm combined chlorine, and a pH = 3.95) (38). The shortage of laboratories that perform analyses for airborne chloramines and the variability in indoor air quality from day-to-day impedes investigators' ability to respond to reports of ocular and respiratory distress related to indoor pools or to obtain rapid and quantitative air measurements at implicated pools. Water-testing data useful for evaluating an indoor air-quality problem include the pH level and total (i.e., free plus combined chlorine) and free chlorine concentrations, which can be used to calculate the level of combined chlorine in the water. Levels that exceed test kit capacity should be re-measured by making dilutions using distilled water. These outbreaks underscore the need to train pool operators and aquatic staff so that they routinely monitor and maintain water chemistry to protect the health of patrons and staff. Air-quality improvements in indoor pools will require technological improvements in water chemistry and treatment and air circulation and ventilation. New studies suggest that installation of ultraviolet treatment devices in pool water recirculation systems can reduce pool chloramine levels (39) and also can effectively inactivate pathogens (including chlorine-resistant Cryptosporidium) (39,40). Plans to improve air quality also can be aided by working with the public to improve swimmer hygiene. The resulting reduction in urine and other nitrogenous waste (e.g., decreased public urination in pools and increased showering before entering pools) should lead to reductions in chloramine levels in both water and air. Such an effort should raise public awareness about the role of urine and sweat in creating the irritants associated with indoor pool swimming. Operators should encourage showering before entering any pool or spa and facilitate frequent bathroom breaks for swimmers, particularly for young children (e.g., instituting adult-only swim times and short closures for water-quality testing). Multiple challenges are associated with understanding the numbers of water-related, chemical illnesses at aquatic venues. Lack of rapid testing and routine testing for chloramines suggests that surveillance for recreational water-associated outbreaks of acute chemical poisoning is likely to have multiple barriers, resulting in underestimation of the true magnitude of the problem. Acute chemical-related WBDOs might be more likely to involve first responders than the traditional epidemiologic or environmental health staff investigating other WBDOs and reporting to WBDOSS. As a result, more efficient reporting will require building strong and effective intra- and interagency communication networks within health departments and with other groups (e.g., first responders and pool operators) to improve the reporting of WBDOs associated with recreational water. SpasSpas are susceptible to human contamination by the same pathogens that contaminate swimming and wading pools, but outbreaks of gastrointestinal illness from spas might be limited because spa usage does not involve as much full body (e.g., head-to-toe submersion) activities as pools, resulting in less water ingestion. However, spa operation is challenging because of difficulty with maintaining disinfectant levels at higher water temperatures or with aeration and the relatively high bather load to water volume typical of spas. As a result, these venues are ideal for amplification of naturally occurring environmental contaminants (e.g., thermophilic pathogens, P. aeruginosa, and Legionella). Skin Infections Spa-associated outbreaks are commonly associated with dermatitis and folliculitis; P. aeruginosa is the most commonly reported agent implicated in these settings (41). During 2005--2006, four WBDOs caused by Pseudomonas (Connecticut, April 2005; New Mexico, April 2005; Wisconsin, July 2005; and Kansas, December 2006), and five WBDOs suspected to have been caused by Pseudomonas (Minnesota, March 2005; Vermont, February 2005; Georgia, February 2006; Tennessee, March 2006; and Wisconsin, February 2006) were reported; four of these outbreaks involved spas, and five involved both spas and pools. The frequent co-location and use of both spas and pools by patrons means that it can be epidemiologically difficult to implicate a particular pool or spa at a single venue. However, amplification of Pseudomonas is most likely to occur at the higher temperatures in spas (42). Nearly all of the Pseudomonas-associated outbreaks occurred as a result of spa use at a hotel, motel, or rented cabin, underscoring the need for improved recreational water quality in these transient visitation, travel-associated settings. Multiple outbreaks included large gatherings (e.g., birthday pool party [Connecticut] and sports tournament [Minnesota]), which can rapidly overwhelm the disinfection capacity of spas and lead to bacterial amplification. In addition, these gatherings often occurred on weekends (Wisconsin), when hotel staff trained in spa maintenance are likely to be off duty. Hotels and motels should consider having only trained employees operate and maintain pools and spas, particularly on weekends when usage is typically highest. Enhanced water-quality monitoring and maintenance should be considered when a large group or event at a hotel is scheduled. Users should be educated about not adding contaminants that might disrupt the spa's water chemistry (e.g., shampoo [Minnesota] and wine [Georgia]). To prevent spa-associated outbreaks, operators must understand the risk factors and steps that can be taken to limit transmission of pathogens, particularly thermophiles. Proper chlorination or bromination effectively kills Pseudomonas and other skin-infecting bacteria. A review of 18 Pseudomonas outbreaks demonstrated that inadequate disinfection was associated with all outbreaks linked to spas (43). Bacterial amplification and biofilm build-up can be prevented by properly maintaining spas, ensuring that chlorine or bromine levels consistently remain >2 ppm, and that pH levels remain in a range of 7.2--7.8. Poor maintenance of spas has been well-documented (44), and studies have demonstrated that Pseudomonas and other bacteria can remain protected in spa biofilms, even in the presence of adequate disinfectant, then rapidly proliferate if the disinfectant level drops (42). Legionellosis Legionellae, which cause both LD and PF, are ubiquitous in freshwater environments (45). Environmental conditions in whirlpool spas (e.g., warm temperatures and water aerosolization) promote the amplification and transmission of the bacteria when combined with low or erratic disinfectant levels. Exposure to Legionella is more likely to occur in the absence of adequate levels of disinfectant, underscoring the importance of maintaining adequate disinfectant levels and pH control. When lapses in preventive measures result in a legionellosis outbreak, morbidity can be reduced by rapid recognition of the outbreak, identification of its source, and immediate implementation of remediation. Remediation methods include cleaning and disinfecting the spa to eliminate Legionella colonization and performing follow-up cultures for Legionella to ensure that re-colonization does not occur (46). All eight legionellosis WBDOs associated with recreational water during 2005--2006 were associated with spas. Five of these outbreaks occurred at hotels which highlights the role of travel in Legionella transmission and illustrates the potential difficulty of detecting travel-associated illnesses when travelers disperse to their resident state or country. CDC's supplementary reporting system for legionellosis collects exposure and travel information. In a 2005 CSTE position statement (http://www.cste.org/PS/2005pdf/final2005/05-ID-01final.pdf), surveillance and active follow up of potential travel-associated case reports was recommended position statement to improve detection of travel-associated clusters of illness and to increase opportunities for disease prevention. During 2005--2006, a total of 10 clusters were identified (47) although not all met WBDO definition. After CSTE's recommendations in 2005, CDC 1) improved communication with international, state, and local public health partners concerning travel-associated LD cases; 2) developed a standardized notification and tracking system; and 3) created a dedicated e-mail address for case reporting ([email protected]). In addition, CDC's legionellosis website (http://www.cdc.gov/legionella) has been updated to provide useful tools for investigating legionellosis outbreaks (including sample questionnaires), sample letters for hotel management, and protocols for environmental assessments of water systems. Interactive Fountains/Wet Decks and Fill-and-Drain PoolsInfectious Gastroenteritis Certain treated water venues (e.g., interactive fountains, which also are called wet decks or spray parks) might be overlooked as potential sites for transmission of infection or pool regulation because they do not have standing water as traditionally found in swimming pools. These venues are particularly prone to contamination by fecal material, vomit, and dirt because of the young users of the small volume of recirculating water. These contaminants can potentially drain into the water reservoir and be sprayed back on users, increasing the likelihood of contaminated water ingestion. The use of interactive fountains has previously been associated with outbreaks of gastroenteritis (48), and outbreaks reported here (Louisiana, August 2005; New York, June 2005; California, July, 2006; and Florida, May 2006) demonstrate that transmission continues to occur in these settings. Not all states regulate interactive fountains which might increase chance of improper design, maintenance, or operation in these venues. In one of the largest outbreaks reported to the WBDOSS, approximately 2,300 persons developed cryptosporidiosis following exposure to a New York spray park. The environmental investigation revealed that recycled water was not adequately filtered and disinfected. In response, New York passed emergency legislation requiring that supplementary disinfection (e.g., ultraviolet radiation or ozonation) be installed on water returning through the sprayers. Designs that improve water treatment for these interactive fountains are needed to reduce the risk for RWIs. Reports of investigations from three additional cryptosporidiosis outbreaks (California, 2006; Florida, 2006; and New York 2005) indicated inadequate disinfection levels (<1.0 ppm chlorine) and the use of sand or cartridge filters, both of which might not be adequate for Cryptosporidium oocyst removal. Filters with diatomaceous earth might be more effective at removing oocysts than sand or cartridge filters. The use of tap water to fill or operate temporary aquatic venues (e.g., fill-and-drain pools) used by young children continues to be a public health challenge (California, July 2006; and Wyoming, July 2005). Lack of disinfection and the traditional use by toddlers and diaper-aged children have resulted in multiple outbreaks being associated with use in both residential and institutional settings (12,49,50). In the California outbreak, nine persons became ill with AGI after attending a pool party where guests swam in a plastic pool filled with untreated tap water. Three children were hospitalized; S. sonnei was confirmed in stool samples from six ill persons. In Wyoming, an outbreak of campylobacteriosis occurred after two families filled a pool with untreated water from a shallow well. In addition, a dog known to roll around in cow feces entered the pool. The potential risk for infection associated with using temporary pools filled with tap water without additional disinfection and filtration should be considered before they are used in residential settings. To reduce the risk for pathogen transmission, persons with gastroenteritis should be excluded, and the pool should be drained and cleaned daily. On the basis of documented outbreaks, fill-and-drain pools should be eliminated from institutional settings or large group events (50). Lakes and RiversInfectious Gastroenteritis Although the proportion of AGI outbreaks associated with untreated venues (e.g., lakes and rivers) relative to treated venues decreased over the previous decade, the number of outbreaks associated with untreated venues has remained relatively constant (Figure 10). During 2005--2006, a total of 13 outbreaks of gastroenteritis associated with untreated freshwater venues were reported; all of these were linked to swimming in lakes or ponds. Freshwater venues have a higher proportion of outbreaks caused by bacterial and viral etiologic agents compared with treated water venues (Figure 5). Multiple studies have determined the utility of water-quality monitoring (16) for assessing the associated risk for swimmer illness (18) in large bodies of water (e.g., Great Lakes and the ocean). However, the small inland water bodies associated with the outbreaks in this report do not have consistent external sources of contamination (e.g., sewer overflow), suggesting that swimmers might be an important source of water contamination and infection transmission. As with treated venues, human behavior plays a key role in the spread of pathogens in untreated bodies of water. Modification of swimmer behavior might be a more critical factor in natural water venues that lack the benefit of disinfection and filtration barriers to transmission. Recommendations for swimmer hygiene in natural waters are the same as those previously discussed for treated pools. In addition, beach managers and swimmers should be aware that shallow, poorly circulated swimming areas, although desirable to many swimmers, might pose a higher risk of exposure to certain pathogens compared to deeper, well circulated swimming areas. Potential methods to improve circulation of water through beach areas should be explored to reduce the longevity of focal, swimmer-derived contamination and waterborne-disease transmission. Reducing exposure to high fecal indicator bacterial levels at sites affected by runoff can be achieved by avoiding swimming immediately after heavy rainfall (reducing exposure to any increase in contaminated runoff) and by not swimming near storm drains or pipes that might release contamination into water bodies (24). Primary Amebic Meningoencephalitis During 2005--2006, five fatal cases of PAM caused by N. fowleri were reported; for two of these cases, there was possibly a common exposure to either a creek or a small spray park. For the remaining three cases, no common exposure was identified (Tables 4, 10). This rare disease is of public health importance because of the high fatality rate associated with infection (>99%) (51) and the public alarm it raises for use of natural waters in the southern tier states in the United States. N. fowleri is a free-living ameba that proliferates in warm freshwater and hot springs. Disease occurs when the ameba coincidentally enters the nasal passages, travels to the olfactory lobe of the brain, and infects brain tissue. The five cases all occurred in southern tier states (Arizona, Georgia, Oklahoma, and Texas) during warm weather months (Tables 4, 10). Three of the five children who died of PAM during 2005--2006 had participated in activities in warm water before onset of symptoms, similar to other known cases of PAM. The source of exposure for the two Oklahoma cases could not be determined despite a public health investigation. The low number of Naegleria infections makes it difficult to determine why certain persons become infected compared with the millions of others with the same or similar exposures to waters across the United States. As a result, the efficacy of existing risk-reduction strategies are uncertain. The finding of Naegleria in the majority of lake water surveys conducted in southern tier states suggests that this minimal likelihood of Naegleria infection always will be associated with swimming in warm, freshwater lakes, rivers, and hot springs. While the most certain way to prevent infections is to refrain from swimming in these freshwater bodies, swimmers might reduce their risk for PAM by not swimming or jumping into bodies of warm freshwater, hot springs, and thermally polluted water (e.g., water around power plants); not swimming or jumping into freshwater during periods of high water temperature and low water volume; holding the nose shut or using nose clips when jumping or diving into bodies of warm freshwater; and refraining from digging in or stirring up sediment while swimming in shallow, warm, freshwater areas. CDC is collaborating with CSTE to more effectively describe the scope of Naegleria infections in the United States, improve surveillance, and analyze available exposure and environmental occurrence data to develop more evidence-based risk-reduction measures and messages (52). Leptospirosis Although infections caused by Leptospira are considered to be more common in tropical and semitropical areas of the world (53), outbreaks reported during 2005--2006 illustrate the potential risk for leptospirosis outbreaks associated with recreational water contact in the United States. Leptospira can be found in the urine of infected wild and domesticated animals, so contamination of natural waters can occur where infected animals live. The route of transmission in humans usually is through contaminated water contact with broken or abraded skin or through contact with the mucosal surfaces of the eye, mouth, nasopharynx, or esophagus. Exposure might also occur through inhalation, ingestion, or prolonged immersion in water, resulting in increased permeability of the skin. Increased skin permeability might play a role in infections resulting from contact with contaminated surface water after flooding (54) or with prolonged use of contaminated surface waters as part of sports or other events (e.g., triathlons) (55,56). Two outbreaks of leptospirosis involving 46 persons were reported for 2005--2006 as well as a previously unreported outbreak in Hawaii in 2004 (57). One outbreak in California (July 2005) was associated with persons working in a drought-affected stream. The second larger outbreak occurred in Florida (November 2005) and was associated with participation in an adventure race. This is consistent with previous outbreaks in other similar competitive venues (55,56). To reduce risk for infection, persons should wear protective clothing, avoid swimming when they have open wounds or abrasions and avoid water contaminated by animal urine. Cercarial Dermatitis During the 2005--2006 surveillance period, two WBDOs of suspected cercarial dermatitis caused by avian schistosomes were reported (California, July 2005 Ohio August 2006). Although the diagnosis was not confirmed, this self-limited disease is known to occur among persons exposed to lakes across the United States where infected birds contaminate water supporting the intermediate host snail (58). The risk for acquiring cercarial dermatitis might be reduced by warning swimmers of potentially contaminated lakes, avoiding shallow swimming areas where infected snails reside, instituting a snail control program, and by not attracting birds to swimming areas (e.g., by not feeding them). Marine WaterNo waterborne disease outbreaks associated with marine waters were reported to WBDOSS before 2005--2006; however, evidence from multiple sources demonstrates that contamination of marine waters is common and that swimmers in marine waters are at increased risk for acquiring AGI (23,59). States and territories report water-quality testing results and notification data for their coastal and Great Lakes recreational water to EPA. In 2006, 32% of monitored beaches were affected at least once by either an advisory or closing as a result of the EPA microbial fecal indicator limits being exceeded or water-quality standards not being met (17). Multiple studies have linked these water-quality indicators with increased risk for RWIs (23,59,60), although RWIs also can occur when water-quality indicators are within established limits (24). The reasons for a lack of reported marine-associated outbreaks might include the wide geographic spread of beachgoers, the fact that some of the marine-associated illnesses are not enteric illnesses typically linked to waterborne causes, and a lack of illness attribution to marine waters. Vibrio Illness Although WBDOs associated with marine waters might be difficult to detect, single cases of Vibrio infections from marine water exposure might be more likely to be reported because of the severity of the illness associated with infection. The number of Vibrio infections associated with water exposures during 2005--2006 (n = 189) was higher than the number reported in 2003--2004 (n = 142), although recreational water exposure constitutes only a small fraction (14.7%) of the 1,287 vibriosis cases from all exposures reported in 2005--2006 (61). Some of the increase in reported cases for 2005 might be attributable to flood water exposure in the Gulf Coast immediately following Hurricane Katrina (62) when active case-finding facilitated identification of Vibrio infections. Reported hurricane-related infections were primarily among persons with wounds who waded through flood waters. The majority of hurricane-related Vibrio infections were caused by V. vulnificus, which predominately occurs in the Gulf Coast. Wound infections from V. vulnificus can cause severe illness and sequelae, including septicemia and the need for amputation. For nonfoodborne cases of V. vulnificus infection, the hospitalization rate is approximately 90% and the case fatality rate is 17%--24% (63,64), similar to the 22.3% case fatality rate among cases reported during 2005--2006 (Table 8). Disease is more common and severe among persons with preexisting wounds and other medical conditions (e.g., diabetes, heart disease, or liver disease) (64,65). V. parahaemolyticus and nontoxigenic V. cholerae infections were also reported among persons with hurricane-related Vibrio infections. The burden of wound-related vibriosis is unknown, although an estimated 8,000 Vibrio infections occur annually, including an estimated 2,800 annual cases not associated with food exposure (64). CSTE added vibriosis to the list of nationally notifiable diseases in January 2007. Vibriosis is reportable in 35 states, although all other states and territories can report vibriosis cases to CDC. Cases are reported to CDC by using the Cholera and Other Vibrio Illness Surveillance report form, which is available at http://www.cdc.gov/nationalsurveillance/PDFs/CDC5279_COVISvibriosis.pdf. Annual summaries of national data on vibriosis are available at http://www.cdc.gov/nationalsurveillance/cholera_vibrio_surveillance.html. Improved surveillance and reporting are designed to increase understanding of the magnitude and distribution of Vibrio illness related to marine water, to better characterize the risk and contributing environmental factors, and to guide the development of appropriate prevention messages (e.g., persons with wound or certain preexisting conditions not swim in warm marine water). Seabather's Eruption One outbreak was reported for 2005--2006 in which swimmers were exposed to marine water. Certain ill persons had symptoms consistent with Seabather's Eruption, a skin condition caused by contact with toxins from stinging jellyfish larvae. However, the majority of persons also exhibited an influenza-like illness which, although previously associated with Seabather's Eruption (66), could also indicate another water-associated etiology. Seabather's Eruption occurs primarily in the marine waters off Florida, the Gulf of Mexico, and the Caribbean Sea particularly during spring and summer months. Whereas risk factors associated with developing Seabather's Eruption are not fully understood, swimmers might be able to reduce their risk by removing bathing suits and thoroughly showering to remove jellyfish larvae after marine water exposure (67). Ongoing research is needed to understand the water conditions that lead to increased risk for illness among swimmers so that appropriate risk-reduction messages can be given to ocean beach visitors. Previously Unreported OutbreaksThe retrospective review of waterborne-disease outbreaks in Minnesota, New York, and Tennessee by EHS-Net Water staff resulted in the reporting of 30 previously unreported recreational water--associated outbreaks and case reports (Table 11). The addition of previously unreported outbreaks increases understanding about the epidemiology of waterborne disease in these jurisdictions. The success of the EHS-Net Water surveillance improvement effort underscores the utility of acquiring personnel who can focus on waterborne disease detection, investigation, and reporting (13). An additional outbreak from 2004 was reported by Hawaii (57). Aquatic Facility-Related Health Events not Associated with Recreational Water UseAll 32 aquatic facility--related health events not associated with recreational water use (Table 12) were reported by New York, which had captured these events through a system, which mandates reporting of chemical injuries. Three events, all of which involved mixing of incompatible pool chemicals that resulted in the release of chlorine gas, were reported during 2005--2006. The first outbreak of ARI resulted from a spill of 50--75 gallons of hypochlorous acid (i.e., bleach), which might have interacted with other chemicals in the spill area. The second event resulted from using a container that was previously used for hypochlorous acid as a container for the acid used to adjust pool pH. Subsequent contact of the pool acid with the hypochlorous acid residue released a chlorine gas plume. The third event involved adding both calcium hypochlorite (chlorine) and trichloro-s-triazinetrione (a chlorinated isocyanurate commonly called trichlor) to the pool chlorinator system, which resulted in a release of chlorine gas. The material safety data sheet for trichloro-s-triazinetrione states that it is not to be mixed with other chemicals, especially calcium hypochlorite; alkalis; and other swimming pool/spa chemicals in their concentrated forms. These events and others (Table 12) highlight the need for new or improved 1) pump room and chemical storage area design and construction (e.g., improved ventilation, and chemical containment and separation), 2) chemical packaging (e.g., to easily differentiate between key pool chemicals), 3) chemical storage (e.g., to prevent mixing accidents), 4) staff training on how to safely store and handle chemicals and maintain and repair chemical-using pool systems, and 5) emergency response protocols. PreventionPrevention of RWIs is likely to be accomplished only through a concerted team effort by public health professionals, swimming venue operators, and the general public. Operators at treated water venues are equipped with various methods that should be employed to prevent outbreaks. The traditional reliance on two water-treatment barriers at treated water venues, chlorination and filtration, likely needs to be expanded to include in-line (i.e., usually installed after filtration and before chlorination) supplemental disinfection (e.g., ultraviolet treatment and ozonation) to increase the level of protection against pathogens, particularly chlorine-resistant Cryptosporidium. Such supplemental disinfection systems will not eliminate waterborne-disease transmission (because these systems are circulation-time dependent), so improved monitoring of water-quality and facility-maintenance programs and improved policies to educate the public and decrease contamination of aquatic facilities with bodily waste also are critical. In response to the lack of protective barriers at untreated swimming venues (e.g., lakes and oceans), beach managers and public health officials should implement water-quality testing programs and educate swimmers concerning appropriate prevention measures (e.g., not swimming after heavy rainfall). Specific efforts should address environmental pathogens unlikely to be prevented by current water-quality guidelines (e.g., illnesses caused by Vibrio and otitis media infections). Public health professionals should 1) improve training for pool inspectors, 2) update and improve pool codes to stay current with changing designs and needs demonstrated by outbreaks summarized in this report, 3) lead and collaborate with aquatic staff to educate the general public, and 4) develop expertise in detecting and investigating recreational water-associated outbreaks, particularly those associated with chemicals. Safe handling and use of chemicals at aquatic facilities needs to be a standard training element that is regularly reinforced. In addition, to improve overall indoor air quality, public health professionals and pool managers need to understand the importance of implementing improvements in pool water quality, swimmer hygiene, air-turnover rates, and ventilation. Educating swimmers can play a vital role in reducing RWIs by encouraging them to follow basic guidelines for healthy swimming. Fecal shedding of pathogens is common (36), so reducing the risk for water-related infection is best achieved by implementing diarrhea-exclusion policies, using appropriate hygiene measures, and advising the public to avoid swallowing recreational water. In addition, the public can inform themselves about RWI prevention. They can become activist swimmers (e.g., checking chlorine and pH levels themselves) and advocate for healthy swimming venues. ConclusionData collected by WBDOSS are used to characterize the epidemiology of waterborne disease and outbreaks associated with both recreational and drinking water. Swimming is a common activity in the United States (68). Certain disease-causing agents are transmitted through shared bodies of water, and new waterborne pathogens that infect humans (e.g., Cryptosporidium and toxigenic E. coli) have emerged in the previous 3 decades. RWIs and outbreaks are associated with both treated and untreated water and with every type of aquatic venue. Common themes derived from the outbreaks in this report include 1) low disinfectant levels or poor filtration; 2) inadequate water-quality monitoring; 3) high bather loads during large events; 4) breakdowns of equipment and delayed detection or repair times; 5) not using ultraviolet radiation or ozonation to treat for Cryptosporidium in pools and interactive fountains; 6) accumulation of combined chlorines in pools accompanied by inadequate indoor air ventilation; 7) inadequately trained aquatic staff, particularly on safe chemical handling practices, 8) lack of communication within and between public health agencies; 9) outbreaks occurring on weekends when trained staff might be off duty; 10) lack of awareness by the general public of appropriate healthy swimming behaviors; and 11) lack of health department familiarity with chemical-associated RWIs. Although no easy solution exists for reducing WBDOs associated with recreational water, a sustained effort by the swimming public, the aquatic management sector, and public health agencies can reduce the associated risk. The millions of persons in the United States who use recreational water every year can best reduce their risk by staying informed regarding the health and safety concerns associated with swimming. Public health officials should lead this educational effort to promote healthy swimming behaviors. Prevention methods discussed in this report should help make swimming experiences healthier, safer and more enjoyable. The aquatic sector also can benefit from the recommendations, which address changes that are needed in operation, maintenance, and chemical handling procedures. Large numbers of violations of state and local pool codes occur each year (15,44), indicating that improved pool operation, disinfection policies, and enforcement are needed to prevent RWIs (33). In addition, improvements in indoor air quality monitoring and widespread dissemination of validated testing protocols are needed to support improved air quality in indoor swimming pool settings. As a result of recommendations from a 2005 national workshop on how to prevent RWIs, CDC is sponsoring development of a national model aquatic health code (MAHC), which involves public health and aquatics sector personnel from across the country and is designed to transform the typical health department program into a data-driven, knowledge-based, risk-reduction effort to prevent disease and injuries and promote healthy recreational water experiences. MAHC will provide uniform guidelines for the design, construction, operation, and maintenance of swimming pools and other disinfected swimming venues. Although nonregulatory in nature, the MAHC should ensure that the best available standards and practices for protecting public health are available for adoption by state and local agencies. Further information is available at http://www.cdc.gov/healthyswimming/model_code.htm. Public health professionals at all levels of government should lead a multidisciplinary approach to prevent RWI that includes surveillance, health education, epidemiologic studies, laboratory support, and environmental health research. Educational resources and campaigns are needed for swimmers, parents, aquatic venue operators, and public health staff. Improved communications, particularly during outbreak investigations, between all areas of the public health system (e.g., infectious disease, environmental health, and surveillance staff) and between agencies in neighboring jurisdictions can 1) enhance awareness concerning ongoing occurrences of RWIs, 2) facilitate reporting to WBDOSS in a timelier manner, and 3) strengthen WBDO investigations and responses to protect the public. The timely collection of clinical specimens and water samples for testing during a WBDO investigation and prompt initiation of an environmental investigation will result in more rapid identification of the etiologic agent and determination of the conditions leading to the outbreak. However, the capacity of public health departments and laboratories to detect and investigate potential WBDOs varies and needs to be strengthened to meet these challenges. WBDO investigations typically require input from various disciplines, including infectious disease epidemiology, environmental health, clinical medicine, water and sanitation engineering, chemists/toxicologists, and microbiology. Additional cross-training of existing personnel in these areas or additional staffing and resources are needed to improve WBDO detection, investigation, and reporting. Other methods of improving surveillance at the local, state, and federal levels include additional review and follow-up of information gathered through other mechanisms (e.g., media reports or emergency responder reports of illness associated with recreational water venues). CSTE passed a 2006 position statement making waterborne-disease outbreaks, as a unit of reporting, nationally notifiable and reportable to CDC starting in 2007. Adoption of this CSTE recommendation at the state level through state-specific legislative action might improve reporting of waterborne outbreaks. In addition, to improve timeliness and completeness of reporting, CDC and EPA are collaborating with public health jurisdictions to implement electronic reporting of WBDOs through the National Outbreak Reporting System (NORS). NORS will be a more systematic data collection tool that will provide public health agencies and waterborne-disease researchers with the evidence base they need to identify the causes of WBDOs and understand the interrelated factors contributing to these outbreaks. EHS-Net Water, a collaborative project between EPA, CDC, and five state health departments, is an effort to improve WBDO identification, investigation, response, and reporting. Environmental health specialists initially focused on understanding their state-specific surveillance systems, leading to the reporting of numerous historical outbreaks to WBDOSS. Although this project has focused primarily on improving drinking water-associated disease outbreak surveillance, it also has markedly improved our understanding of recreational water-associated outbreaks in EHS-Net Water states, which demonstrates the value of investing water-specific resources in certain jurisdictions. Focusing on improving awareness, training, resources, and communication will improve the quality of the data in WBDOSS. These efforts should make public health activities related to waterborne disease more efficient and, in turn, reduce the burden of recreational water-associated disease and injury (Box). Acknowledgments The authors thank the following persons for their contributions to this report: state, local, and territorial waterborne-disease surveillance coordinators; state, local, and territorial epidemiologists and environmental health personnel; Mark Eberhard, PhD, Monica Parise, MD, Bonnie Mull, MPH, Division of Parasitic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC; Lorraine Backer, PhD, Division of Environmental Hazards and Health Effects, National Center for Environmental Health, CDC; Charles Otto, Vince Radke, MPH, Division of Emergency and Environmental Health Services, National Center for Environmental Health, CDC; Sean Shadomy, DVM, MPH, Division of Foodborne, Bacterial and Mycotic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC. References
* Composed of the Republic of the Marshall Islands, the Federated States of Micronesia, and the Republic of Palau; formerly parts of the U.S.-administered Trust Territory of the Pacific Islands. † Additional terms have been defined (Appendix A, Glossary of Definitions). Table 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 9/4/2008 |
|||||||||
|